Mass gathering medicine (MGM) is an exciting niche field of emergency medicine focused on providing emergency medical care at large events. Mass gatherings, as the name implies, are events in which “large numbers of people assemble in public or private spaces to celebrate or participate in musical, sporting, cultural, religious, political, and other events.” (1, p 231) With such large numbers of people accumulating in relatively small areas, mass gatherings (MG) have the potential to overwhelm local resources and place participants at increased risk of injury, illness, and potential for mass-casualty scenarios (2). Injury and illness patterns vary greatly from event to event and are influenced by a myriad of factors including weather, crowd demographics, type of event, the presence of alcohol or drugs on site, and venue characteristics (3,4). Also called “event medicine” or “festival medicine,” MGM goes beyond just providing immediate health care to participants; MGM focuses on alleviating the stress these events place on the local area health infrastructure.

The State of Affairs in Canadian Mass Gathering Medicine
Canadian MGM is in its relative infancy (2). Until recently, MGM has generally been viewed as the realm of pre-hospital providers, and the majority of medical companies providing care at MGM events in Canada still reflect this perception. Interestingly, while there are many stakeholders invested in the success of an event in Canada, there is no universal obligation to consider the impact that the event will have on the local health infrastructure, i.e., no requirements to involve local hospitals or health authorities in event planning (5). This also means there is no universal requirement to have MGM teams on site, and event organizers are free to select a medical plan and provider that they feel will best suit their event and budget.
Long-standing legacy organizations such as Red Cross and St. John’s Ambulance are a welcome sight for many at events, and provide opportunities for first aid providers to volunteer within their communities and provide first aid. Alternatively, event organizers may choose private medical companies, which range in experience (and price!) from first aid teams to physician-led, critical care teams (1).

Mass Gathering Medicine: The New Frontier
As MGM moves out of its infancy, observational and cohort studies continue to demonstrate the need for a coordinated medical plans at large events to alleviate flooding of emergency rooms and overwhelming local area health infrastructure (4-7). Current Canadian MGM leaders, including Dr. Adam Lund and Dr. Sheila Turris are starting to develop event planning models. These models will assist future MGM planners in anticipating the medical needs of an event, but more research and development is needed before any model is ready for prime time (2). MGM needs physician leadership and further research to implement these models. We need to stop thinking of MGM as “prehospital medicine,” and instead recognize it as a new frontier of emergency medicine.
Mass gathering medicine is generally accepted in the realm of emergency medicine (1). There is significant overlap in the skills required for medical care provided at mass gathering events and the emergency department including triage, critical care expertise, resource allocation, and the ability to work in a multi-disciplinary team. Additionally, mass gathering physicians require additional skills in areas such as risk assessment, event medical planning, logistics, communications, finite resource allocation and resupply, and working in variable weather environments.
Practice Makes Perfect
Large scale mass gathering events have such potential for disruption within the local area that they have been compared to “planned disasters” (8). Many aspects of the planning and provision of medical care at mass gathering events directly overlap with the skills needed to respond to a mass-casualty event (1). As such, these events may provide a unique opportunity for an emergency physician to enhance their skills and preparedness for work in disaster medicine.
The table below summarizes the common themes in both mass gathering and disaster medicine, highlighting some of the similarities and differences.
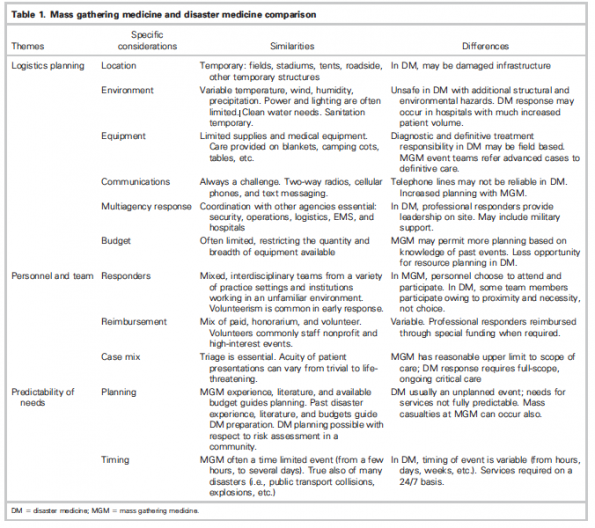
Lund et al. 2011 (1)
While efforts are made in most communities to train for disasters, these are often limited to tabletop exercises and/or costly simulations. Given the similarities between mass gathering and disaster medicine, mass gatherings can provide medical professionals with a “controlled and readily available proxy”(1 p. 233) to access practical experience and training applicable to disaster medicine.
Take Home Message
Mass gathering medicine is an exciting niche area of emergency medicine with the ability to provide controlled environments for healthcare providers to develop skills applicable to disaster medicine. Still in its infancy, mass gathering medicine is primed to be an established specialty. However, more research, support, and physician leadership is needed to develop sufficient guidelines and planning models to assist event planners in anticipating medical needs at events.
References
- Lund, Adam, Samuel J. Gutman, and Sheila A. Turris. “EMS: Mass Gathering Medicine: A Practical Means of Enhancing Disaster Preparedness in Canada.” CJEM : Journal of the Canadian Association of Emergency Physicians; Pickering 13, no. 4 (July 2011): 231–36.
- Turris, Sheila A., Adam Lund, Alison Hutton, Ron Bowles, Elizabeth Ellerson, Malinda Steenkamp, Jamie Ranse, and Paul Arbon. “Mass-Gathering Health Research Foundational Theory: Part 2 – Event Modeling for Mass Gatherings.” Prehospital and Disaster Medicine 29, no. 6 (December 2014): 655–63. https://doi.org/10.1017/S1049023X14001228.
- Moore, Riley, Kelly Williamson, Mark Sochor, and William J. Brady. “Large-Event Medicine—Event Characteristics Impacting Medical Need.” The American Journal of Emergency Medicine 29, no. 9 (November 2011): 1217–21. https://doi.org/10.1016/j.ajem.2010.07.018.
- Schwartz, Brian, Sarah Nafziger, Andrew Milsten, Jeffrey Luk, and Arthur Yancey II. “Mass Gathering Medical Care: Resource Document for the National Association of EMS Physicians Position Statement.” Prehospital Emergency Care 19, no. 4 (October 2, 2015): 559–68. https://doi.org/10.3109/10903127.2015.1051680.
- Lund, Adam, Sheila A. Turris, and Ron Bowles. “Conceptualizing the Impact of Special Events on Community Health Service Levels: An Operational Analysis.” Prehospital and Disaster Medicine 29, no. 5 (October 2014): 525–31. https://doi.org/10.1017/S1049023X14000880.
- Lund, Adam, and Sheila A. Turris. “Mass-Gathering Medicine: Risks and Patient Presentations at a 2-Day Electronic Dance Music Event.” Prehospital and Disaster Medicine 30, no. 3 (June 2015): 271–78. https://doi.org/10.1017/S1049023X15004598.
- Rabb, Haddon, and Jillian Coleby. “Hurt on the Hill: A Longitudinal Analysis of Obstacle Course Racing Injuries.” Orthopaedic Journal of Sports Medicine 6, no. 6 (June 1, 2018): 2325967118779854. https://doi.org/10.1177/2325967118779854.
- Fink, Sheri. “New York City Marathon’s Medical Director Brings a New Philosophy to Patient Care.” The New York Times, November 7, 2010, sec. Sports. https://www.nytimes.com/2010/11/08/sports/08medical.html.