

Migraine headaches are not a benign disease – they have a significant impact on quality of life, ability to function, and pose a considerable economic and societal burden.
Prevalence tends to peak during peoples’ period of highest productivity.
According to the World Health Organization’s (WHO) update on Global Burden of Disease (2004), a severe migraine is considered to be as disabling as being quadriplegic, having active psychosis or even having terminal stage cancer.
Acute Migraine Abortive Treatment
THE CLASSIC MIGRAINE COCKTAIL
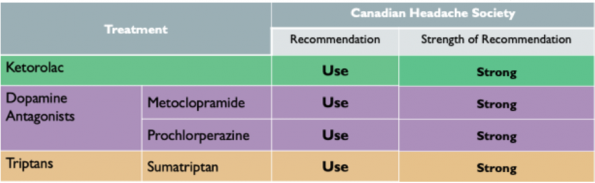
The Canadian Headache Society recommends 3 acute therapies that should be offered as first-line to all patients presenting with an acute migraine which are supported by a strong recommendation with high quality evidence.
- Ketorolac
- Dopamine Antagonists (Metoclopramide or Prochlorperazine)
- Triptans
For other acute therapy options (Magnesium, Dexamethasone) please refer to Dr. Tamara McColl’s Grand Rounds summary on “Novel Migraine Therapy in the ED” from 2015.
Magnesium appears to be an effective adjunct for migraines refractory to first-line therapies.
Dexamethasone has been shown to decrease the recurrence of episodic migraines.
ACUTE MIGRAINE ADJUNCTS – THE DO’S AND THE DON’TS

IV Valproic Acid (VPA)
Valproic acid (PO) is commonly used for migraine prevention which has led to an interest in exploring whether the IV formulation can be used as an abortive therapy
VPA increases GABA levels in the central tracts associated with headache pain.
3 main benefits of antiepileptics for migraine treatment:
-
- Lower incidence of cardiovascular adverse effects (suitable for those with contraindications to triptans or ergotamine)
- Lack of sedating properties
- Low potential for addiction or medication-overuse
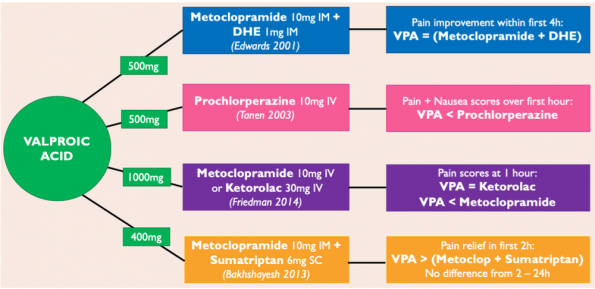
Several studies have been done comparing various doses of VPA to standard therapy with mixed results:
-
- Edwards et al. (2001) showed that IV VPA was considered equally effective as the combination of Metoclopramide + Dihydroergotamine at improving headache pain within the first 4 hours after treatment.
- Tanen et al. (2003) found that IV VPA was significantly less effective at reducing pain and nausea scores when compared to prochlorperazine.
- Friedman et al. (2014) found IV VPA as effective as ketorolac but less effective than metoclopramide.
- An RCT by Bakhshayesh et al. (2013) concluded that IV valproic acid was significantly more effective at reducing pain in the first 2 hours of treatment in patients with prolonged migraines, however, there was no benefit to associated symptoms over standard therapy.
Side effects from a single dose of IV VPA were uncommon but did include nausea, dizziness and flushing. There were no adverse events noted in any of the trials.
Take-Home Points: Evidence for IV VPA in acute migraines treatment is mixed and the optimal dose is uncertain. Most studies performed to date are small and have limited quality. Growing evidence for IV VPA may have a role and may provide another treatment option for failed ED therapy. IV VPA may be available as per special access depending on your ED site.
Sphenopalatine Ganglion Block (SPG block)
The SPG is located behind the middle nasal turbinate and is implicated in headache syndromes. It has sparked interest as a target for a local block in the treatment of migraine headaches.
Several methods available:
- Method of Barre
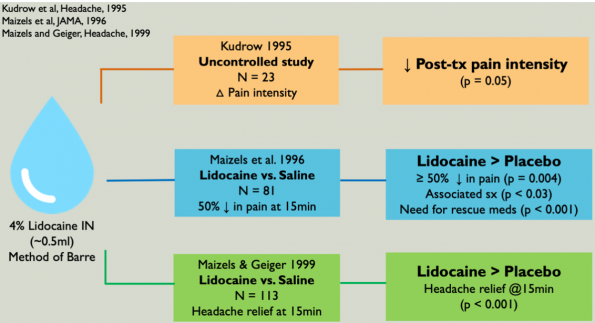
- Mojica et al. (1996) conducted a review study examining the efficacy of SPG blocks in primary headache disorders.
- Reviewed the Method of Barre un which patients lie supine with their neck extended over the edge of the bed by 45 degrees and rotate 30 degrees towards the affected side. 0.5ml of Lidocaine 4% is instilled into nares over 30 seconds.
- Concluded that intranasal lidocaine (via SPG block) is effective in treating various headaches (including migraines).
-
- Limitations of theses studies include:
- Small sample size
- Potential for unblinding
- Technique dependent
- Limitations of theses studies include:
2. Tx360 targeted device
-
- Schaffer et al. (2015) conducted an RCT on 93 patients, testing the efficacy of an SPG block for the treatment of acute anterior headache using a targeted Tx360 device, and compared 0.3ml of 0.5% Bupivacaine vs 0.3ml of Normal Saline.
- The Tx360 technique involves the insertion of a long soft tube/applicator through the nose, targeting the SPG.
- They concluded that this technique was not more effective than placebo at achieving significant acute pain relief at 15 mins [ARR 7.5% (-13% – 27%)], however, it was more likely to achieve pain freedom at 24 hrs [ARR 24.7% (2.6% – 43.6%)].
Take-Home points: Evidence is mixed. Hypothesis-generating outcomes suggest there could be a benefit at 24 hour. Most studies to date have been small. Overall SPG blocks are a low-risk option for any patient presenting with migraine
Ketamine
Sub-dissociative doses of ketamine have been used in a variety of pain conditions, and as such, its effectiveness in headache disorders such as migraine is an area of interest.
IV Ketamine
- Etchinson et al. (2018) did an RCT evaluating low dose-ketamine in the treatment of migraines by randomizing patients with acute migraine to receive 0.2mg/kg of IV ketamine or an equivalent volume or normal saline administered over 1 min.
- There was no significant difference between the ketamine and placebo groups [mean difference -1.0 (IQR -2-1); p=0.5] in pain score reduction at 30 mins.
- They concluded that Ketamine 0.2mg/kg was not an effective therapy for acute migraine pain in the ED.
- Limitations of this study:
- Small sample size, single centre ED
- Convenience sample
- Dosage chosen (may need a higher dose to see a true effect)
Intranasal Ketamine
- Banish et al. (2019) conducted a controlled superiority trial (the THINK trial – Treatment of Headache with Intranasal Ketamine).
- They included 53 patients with any primary headache disorder and compared intranasal (IN) ketamine 0.75mg/kg vs the combination of Metoclopramide 10mg IV + Diphenhydramine 25mg IV (with the additional option of Ketorolac 30mg IV or Dexamethasone 10mg IV).
- The primary outcome was the change in pain scores from study start to 30 mins after treatment.
- Concluded that IN ketamine was not superior to common IV ED therapies for headache pain [effect size 6.8 (-5.8-19.4)].
- Limitations of this study:
- Not limited to migraine headaches
- Small sample size
- Imperfect binding
- Superiority trial design
Take-Home points: The best available evidence does not demonstrate benefit with ketamine in the acute treatment of migraine pain in the ED.
Think Twice About Opioids
Research has shown many EDs across North America continue to use opioids in the treatment of migraines. The evidence strongly urges providers to avoid opioids in the treatment of migraines.
When used for migraines opioids:
- Are not effective
- Result in longer ED stays
- Are known to interfere with triptan effectiveness
- Have the potential for addiction and increase the likelihood for return ED visits.
- Increases the likelihood of the developing medication-overuse headaches, as well as the progression of episodic into to chronic migraines.
Take-Home points: Do not use opioids in the treatment of migraines.
Abortives and Preventatives
Migraines will have a recurrence 2/3 of the time within 28 hours of discharge from the ED – this is a major problem. We need to recognize chronic migraines as a complication of poorly controlled episodic migraines, making it crucial to properly control acute migraine attacks.
Top 3 recommended abortive therapies:
- Acetaminophen
- NSAIDS (Ibuprofen or Naproxen)
- Triptans
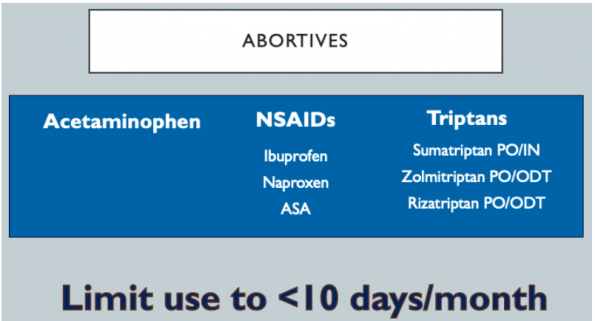
The medications in the top 3 therapies list can be used up to 10 days/month alone or in combination. This limit is to prevent medication-overuse headaches. Don’t be afraid of utilizing triptans but be aware of their contraindications:
- Coronary artery disease
- Peripheral vascular disease
- Uncontrolled hypertension
- Recent MAOI use (within 2 weeks)
- Recent ergotamine use (within 24 hrs)
- Hemiplegic or basilar migraine
- Pregnancy or lactation
Take-Home points: Migraine recurrence rates are high and therefore patients suffering from migraines should be offered abortive management.
PREVENTATIVES

These medications are prescribed for long term daily use with the goal of reducing headache frequency, duration, and severity. The under-prescribing of preventatives is perhaps the most important quality gap in the ED delivery of migraine care.
Why are preventatives important?
- A retrospective study done Silberstein et al. (2003) looked at how long-term resource utilization was affected by the use of migraine preventive medication when added onto a regimen that already included acute therapy.
- They found that the use of preventative therapy for migraines:
- ED visits decreased by 82%
- Outpatient clinic visits decreased by 51%
- The number of CT scans ordered decreased by 75%
- A systematic review and meta-analysis done by Shamliyan et al. (2013) included 66 RCTs evaluating the benefit of prophylactic meds in reducing monthly migraine frequency by at least 50%.
- A 2007 surgery of over 160 000 patients with a migraine found that 40% qualified to prophylaxis but only 12% received it.
- Clearly, there is a huge gap between what we could be offering and what we are offering for our patients with migraines.
Why should we, as emergency physicians, start prescribing preventatives?
- Certainly, there is a role for primary care providers (PCP) in offering theses medications, the responsibility does not just like on them but also us as emergency physicians due to the following findings:
- Migraine patients presenting to ED are more likely to have uncontrolled migraines
- Many patients presenting to ED do not have a PCP.
- A minority of migraines are offered migraine prophylaxis from their PCP.
- We can close the gap to patient care by prescribing prophylactic medications, see dramatic reductions in return ED visits, and alleviate the significant economic and societal implications of this condition.
- We wouldn’t treat an asthma exacerbation in the ED without sending the patient home with puffers – we, therefore, should not be sending home our migraines home without a similar outpatient management plan – let’s expand our scope!
3 simple steps to Prescribing Prophylactics
- Step 1 – Refine your migraine history with 3 key questions to identify your prophylaxis candidates. How many days per month:
- Do you have a migraine?
- Are you headache-free?
- Do you take medication for a headache?
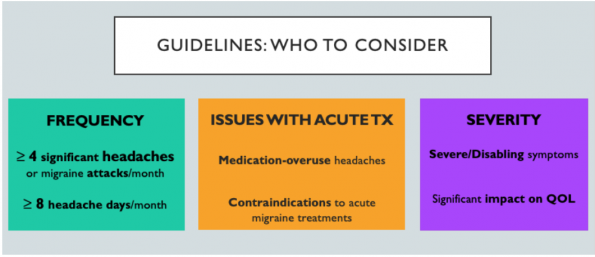
It is recommended that we offer migraine preventatives to the following populations:
-
- Those with frequent headaches
- Those with issues with acute treatment
- Those with severe symptoms
- Step 2 – Select medications and explore options for comorbidity co-treatment
- The top 3 preventative medications with the highest quality data and strongest recommendations from the Canadian Headache Society (CHS) are Metoprolol, Amitriptyline and Topiramate.
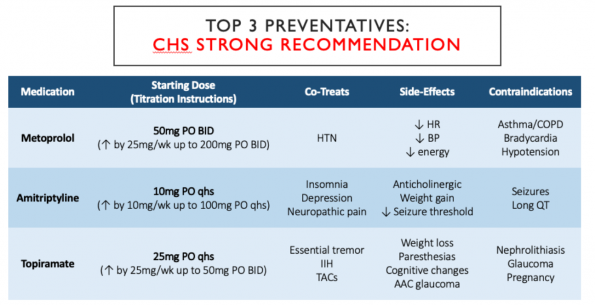
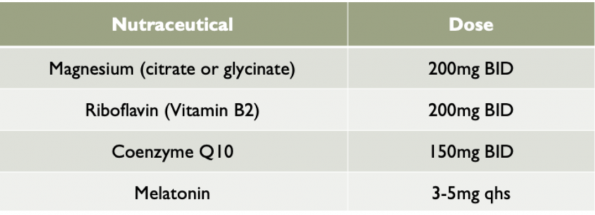
-
- There are also nutraceutical options, that despite not having much evidence to support their use com highly recommended as low risk, are well toleration options for prophylaxis.
- Step 3 – Educate your patient on expectations and medication-overuse
- The goal of prophylactic therapy is the reduction of migraine burden by frequency (>50%) and by the number of headache days by (>50%).
- The medications will need titration by a family physician or neurologist.
- It may take up to 2 months to get to the target dose and to see the full benefit of prophylaxis.
- Recommend use of headache diary.
- Educate on avoiding medication-overuse:
- Limit analgesia use to <10 days/month
- Failure to limit the use of analgesia may lead to progression of migraines from episodic to chronic.
Take-Home points: We can ameliorate the care of patients with migraines with these simple 3 steps – asking the 3 key questions on history to identify candidates, prescribe preventative treatment when appropriate and educate patients on expectations and avoidance of medication-overuse.
Future Directions
Calcitonin Gene-Related Peptide (CGRP) Receptor Antagonists
- CGRPs are neurotransmitters released during a migraine attack and facilitate pain transmission.
- New class of drugs that antagonize the CGRP receptors have been studied for the treatment of acute migraine headaches.
- Proposed benefit – lack of vasoconstriction
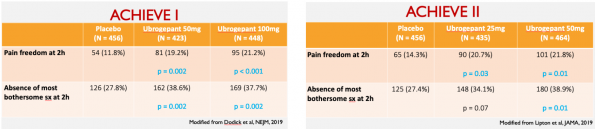
ACHIEVE I and II Trials are two recently published studies evaluating the new CGRP receptor antagonists for aborting migraines.
-
- Both trials are in phase 3, multi centre, double-blinded studies evaluating the efficacy, safety, and tolerability of Ubrogepant compared to placebo, for acute treatment of a single migraine attack.
- ACHIEVE I – compared Ubrogepant doses of 50mg vs 100mg vs placebo.
- ACHIEVE II – compared Ubrogepant doses of 25mg vs 100mg vs placebo.
- Primary efficacy outcomes in both studies were:
- Pain freedom at 2 hrs after medication administration
- Freedom from the most bothersome migraine-associated symptom (nausea, photophobia, or photophobia) at 2 hours after medication administration
- Both trials concluded that Ubrogepant is more effective than placebo in achieving freedom from pain and relief from most bothersome symptom at 2 hours after administration (exception = 25mg dose which was not better than placebo).
-
- Most common side effects: nausea, somnolence and dry mouth.
- Limitations of the study:
- No active comparators in either of these studies.
- Findings based on a single migraine attack.
- Ubrogepant is now FDA approve in the USA.
Ditans
- Ditans are serotonin-1F receptor agonists, and also lack a vasoconstrictive effect when activated.
- Several recent clinical trails have compared the effectiveness of Lasmiditan to placebo (SAMURAI and SPARTAN), and examined adverse effects (GLADIATOR trial).
- Overall conclusions – Lasmiditan is more effective than placebo at relieving acute headache pain at 2 hours, and may be a new, safe, effective option for acute migraine treatment.
- Lasmiditan is now FDA approved in the USA.
Take-Home points: There are new FDA approved abortive medications for acute migraine, CGRP antagonists and Ditans, that are in the early stages of research. They may be a good option for those who have failed or have contraindications to triptans or other abortives.
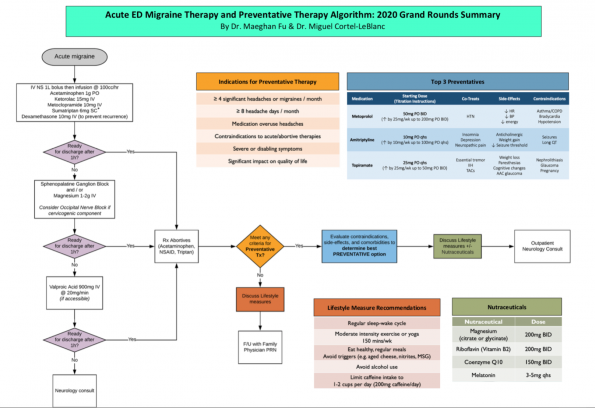
Proposed Algorithm for Migraine Management in the ED
Take-Home Points
- A good history is vital to proper migraine management.
- IV Valproic Acid and Sphenopalatine Ganglion Blocks are good options to consider when treating in the ED, especially in those who may be refractory to our common ED cocktail.
- The evidence does not currently support the use of Ketamine in the ED for acute migraines.
- We should avoid the use of opihoidsin migraine management at all costs.
- The prescription of abortive should be considered in all patients who present with migraines.
- We should strongly consider starting migraine prophylaxis in select migraines, as we can make the huge changes for the patient and the medical system as a whole.
- There are new and exciting advances in migraine management around the corner.
References
- Zhang, W., McLeod, C., Koehoorn, M. The Relationship Between Chronic Conditions and Absenteeism and Associated Costs in Canada. 2016. Scand J Work Environ Health, 1;42(5):413-22.
- Mathers, C. WHO Global Burden of Disease 2004 Update. World Health Organization, Page 33. Table 8. Disability classes for the GBD study, with examples of long-term disease and injury sequelae falling into each class
- Guidelines – Canadian Headache Society. (2019). Retrieved from https://headachesociety.ca/guidelines/
- Edwards, K. R., Norton, J., & Behnke, M. (2001). Comparison of Intravenous Valproate Versus Intramuscular Dihydroergotamine and Metoclopramide for Acute Treatment of Migraine Headache. Headache: The Journal of Head and Face Pain, 41(10), 976–980.
- Tanen, D. A., Miller, S., French, T., & Riffenburgh, R. H. (2003). Intravenous sodium valproate versus prochlorperazine for the emergency department treatment of acute migraine headaches: A prospective, randomized, double-blind trial. Annals of Emergency Medicine, 41(6), 847–853.
- Friedman, B. W., Garber, L., Yoon, A., Solorzano, C., Wollowitz, A., Esses, D., … Gallagher, E. J. (2014). Randomized trial of IV valproate vs metoclopramide vs ketorolac for acute migraine. Neurology, 82(11), 976–983.
- Bakhshayesh, B., Saadat, S. M. S., Rezania, K., Hatamian, H., & Hossieninezhad, M. (2013). A randomized open-label study of sodium valproate vs sumatriptan and metoclopramide for prolonged migraine headache. The American Journal of Emergency Medicine, 31(3), 540–544. doi: 10.1016/j.ajem.2012.10.014
- Mojica, J., Mo, B., & Ng, A. (2017). Sphenopalatine Ganglion Block in the Management of Chronic Headaches. Current Pain and Headache Reports, 21(6).
- Kudrow, L., Kudrow, D. B., & Sandweiss, J. H. (1995). Rapid and Sustained Relief of Migraine Attacks With Intranasal Lidocaine: Preliminary Findings. Headache: The Journal of Head and Face Pain, 35(2), 79–82.
- Maizels, M., Scott, B., Cohen, W., Chen, W. (1996). Intranasal Lidocaine for Treatment of Migraine: A Randomized, Double-blind, Controlled Trial. JAMA, 276(4), 319-321.
- Maizels, M., & Geiger, A. M. (1999). Intranasal Lidocaine for Migraine: A Randomized Trial and Open-Label Follow-up. Headache: The Journal of Head and Face Pain, 39(8), 543–551.
- Schaffer, J. T., Hunter, B. R., Ball, K. M., & Weaver, C. S. (2015). Noninvasive Sphenopalatine Ganglion Block for Acute Headache in the Emergency Department: A Randomized Placebo-Controlled Trial. Annals of Emergency Medicine, 65(5), 503–510.
- Etchison, A., Bos, L., Ray, M., Mcallister, K., Mohammed, M., Park, B., … Heitz, C. (2018). Low-dose Ketamine Does Not Improve Migraine in the Emergency Department: A Randomized Placebo-controlled Trial. Western Journal of Emergency Medicine, 19(6), 952–960.
- Benish, T., Villalobos, D., Love, S., Casmaer, M., Hunter, C. J., Summers, S. M., & April, M. D. (2019). The THINK (Treatment of Headache with Intranasal Ketamine) Trial: A Randomized Controlled Trial Comparing Intranasal Ketamine with Intravenous Metoclopramide. The Journal of Emergency Medicine, 56(3).
- Bigal, M. E., & Lipton, R. B. (2008). Excessive acute migraine medication use and migraine progression. Neurology, 71(22), 1821–1828.
- Friedman, B. W., Kapoor, A., Friedman, M. S., Hochberg, M. L., Rowe, B. H. (2008). The relative efficacy of merperidine for the treatment of acute migraine: A meta-analysis of randomized controlled trials. Ann Emerg Med, 52(6):705-713.
- Tornabene, S. V., Deutsch R., Davis, D. P., Chan, T. C., Vilke, G. M. (2009). Evaluating the use and timing of opioids for the treatment of migraine headaches in the emergency department. J Emerg Med, 36:333–337.
- Ho, T. W., Rodgers, A., Bigal, M. E. (2009). Impact of recent prior opioid use on rizatriptan efficacy. A post hoc pooled analysis. Headache, 49:395-403.
- Colman, I., Rothney, A., Wright, S. C., Zilkalns, B., & Rowe, B. H. (2004). Use of narcotic analgesics in the emergency department treatment of migraine headache. Neurology, 62(10), 1695–1700.
- Tepper, S. J. (2012). Opioids should not be used in migraines. Headache, 52(S1): 30-34.
- Friedman, B. W., Solorzano, C., Esses, D., Xia, S., Hochberg, M., Dua, N., … Gallagher, E. J. (2010). Treating Headache Recurrence After Emergency Department Discharge: A Randomized Controlled Trial of Naproxen Versus Sumatriptan. Annals of Emergency Medicine, 56(1), 7–17.
- Silberstein, S. D., Winner, P. K., & Chmiel, J. J. (2003). Migraine Preventive Medication Reduces Resource Utilization. Headache: The Journal of Head and Face Pain, 43(3), 171–178.
- Shamliyan, T. A., Choi, J.-Y., Ramakrishnan, R., Miller, J. B., Wang, S.-Y., Taylor, F. R., & Kane, R. L. (2013). Preventive Pharmacologic Treatments for Episodic Migraine in Adults. Journal of General Internal Medicine, 28(9), 1225–1237.
- Lipton, R. B., Bigal, M. E., Diamond, M., Freitag, F., Reed, M. L., & Stewart, W. F. (2007). Migraine prevalence, disease burden, and the need for preventive therapy. Neurology, 68(5), 343–349.
- Guidelines – American Headache Society. (2019). Retrieved from https://americanheadachesociety.org/resources/guidelines/
- Guidelines – American Academy of Neurology. (2019). Retrieved from https://www.aan.com/policy-and-guidelines/guidelines/
- Bigal, M. E., Lipton, R. B. (2008). Excessive acute migraine use and migraine progression. Neurology, 71(22):1821-8.
- Dodick, D.W., Lipton, R.B., Ailani, J., Lu, K.L., Finnegan, M.P.H., Trugman, J.M., Szegedi, A. (2019). Ubrogepant for the Treatment of Migraine. The New England Journal of Medicine, 381:2230-41
- Lipton, R.B., Dodick, D.W., Ailani, J., Lu, K., Finnegan M., Szegedi, A., Trugman, J.M. (2019). Effect of Ubrogepant vs placebo on pain and the most bothersome associated symptom in the acute treatment of migraine: The ACHIEVE II Randomized Clinical Trial. JAMA, 322(19):1887-1898
- Kuca, B., Silberstein, S.D., Wietecha, L., Berg, P.H., Dozier, G., Lipton, R.B. (2018). Lasmiditan is an effective acute treatment for migraine: A phase 3 randomized study. Neurology, 91:e2222-e2232
- Goadsby, P.J., Wietecha, L.A., Dennehy, E.B., Kuca, B., Case, M.G., Aurora, S.K., Gaul, C. (2019). Phase 3 randomized, placebo-controlled, double-blind study of lasmiditan for acute treatment of migraine. Brain, 142:1894-1904
- Brandes, J.L., Klise, S., Krege, J.H., Case, M., Khanna, R., Vasudeva, R., Raskin, J., Pearlman, E.M., Kudrow, D. (2019). Interim results of a prospective, randomized, open-label, Phase 3 study of the long-term safety and efficacy of lasmiditan for acute treatment of migraine (the GLADIATOR study). Cephalagia, 39(11):1343-1357.


Thanks to the author for sharing the updates on migraine management. The information given above about headaches is really good and beneficial for everyone who is suffering form migraine.
i read your blog such a very useful information,
Thankyou so much for sharing this accurate information with us.Really appreciate your work.Please keep sharing .
This blog offers valuable insights into migraine management. The author provides updates on current approaches and highlights the importance of individualized treatment plans. It’s a great resource for anyone seeking effective strategies to alleviate and manage migraines.