

In part 1 of this 2-part series, we discussed diagnosis and initial management of alcohol withdrawal. In part 2, we discuss the role of the benzodiazepines on discharge, how to use gabapentin, naltrexone, and communication strategies to optimize discharge to help your patient meet their goals. For quick reference, here is an algorithm for providers, and handout for patients.
Are benzodiazepines necessary?
After appropriate benzodiazepine loading dose and/or symptom-triggered therapy, an ongoing benzodiazepine taper is generally unnecessary for seizure prevention.
Although seizure prevention was not the primary outcome, in many studies, further doses of diazepam were generally not needed once the target CIWA score was reached.1–3 Early case series and RCTs found no seizures after diazepam loading.1,2 Pharmacokinetically this is due to the long half-life of diazepam compared to the window in which seizure risk is highest (see Part 1).
Unsupervised benzodiazepines may be dangerous due to its additive effect with alcohol – resulting in the risk of over-sedation and respiratory arrest in overdose.
The benzodiazepine taper is thus rarely indicated. A short course may be considered in the extremely high risk patient with poor follow-up (for seizure/delirium), or if shorter half-life drugs are required (i.e. lorazepam). If so, counsel the patient to stop if they start drinking, consider a supervised setting (i.e., detox or a family member), or write daily dispense on the prescription to limit the risk of overdose.
Gabapentin > Benzodiazepines
Several small randomized control trials support the use of gabapentin for treatment of withdrawal symptoms.4,5 It provides similar decrease in the CIWA-Ar score over time with better outcomes for sleep, craving, and sedation. However, it does NOT reliably prevent seizures – and thus should only be used after seizure prophylaxis with benzodiazepines, or in the patient at very low risk of severe withdrawal.
Compared to benzodiazepines there may also be decreased relapse – gabapentin is even considered by the American Psychiatric Association as second line for the treatment of the underlying alcohol use disorder as an anti-craving agent.6,7 It is also lower risk for abuse or overdose – there is no interaction with alcohol.8
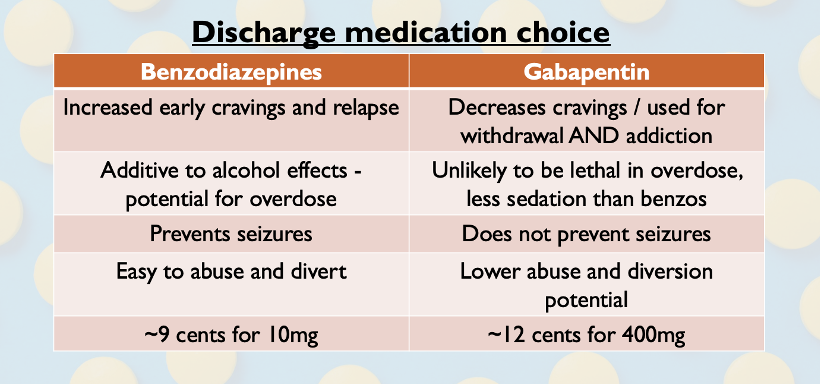 Consider Gabapentin 400mg TID x 7 days instead of discharging your patient with ongoing benzodiazepines. Gabapentin is contraindicated in renal failure.
Consider Gabapentin 400mg TID x 7 days instead of discharging your patient with ongoing benzodiazepines. Gabapentin is contraindicated in renal failure.
Naltrexone in the ED
Naltrexone or acamprosate have an incredibly robust body of evidence for the treatment of the underlying alcohol use disorder as an anti-craving agent. This can be started in the emergency department.
Naltrexone is an opioid receptor antagonist that decreases cravings and the high from alcohol. It is the first-line medication for the treatment of alcohol use disorder. In a meta-analysis of 53 RCTs and 9140 patients, the NNT was 20 for abstinence and 12 to prevent a return to heavy drinking.9 Contraindications are opioid use, liver failure or acute hepatitis with LFTs 3x the upper limit of normal.10
Naltrexone can be started from the ED at 25mg po daily x 4 days then 50mg po daily until follow-up. A follow-up is mandatory to repeat liver enzymes (within 2-4 weeks), monitor progress and mood. This should be started in anyone trying to quit who will not see the addictions physician right away – i.e., during weekends, holidays, clinic closures, or in those going to detox for some time. You can listen to one patient’s perspective here:
Naltrexone costs ~$2.81 per 50mg pill if out of pocket, but is covered by a limited use code for Ontario government drug insurance (ODB or ODSP) under LU 532. It requires the patient to have alcohol use disorder, be willing to cut down, and engage in non-pharmacologic management.
Acamprosate (LU531) is the other first-line medication for alcohol use disorder; preferred when patients have liver enzyme elevation, but it is currently not available in Canada due to manufacturing issues.
Screening, Brief Intervention, Referral to Treatment
SBIRT (Screening, Brief Intervention, Referral to Treatment) is the communication strategy of choice for brief encounters in addictions medicine.
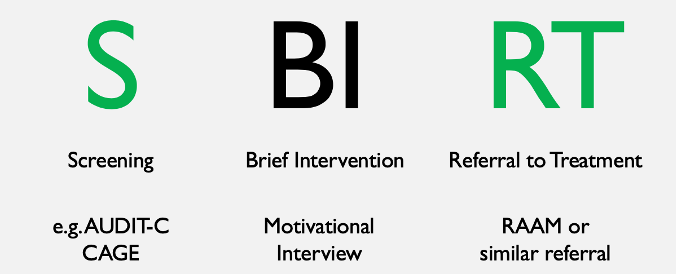
Screening can use formal scores like AUDIT-C or the CAGE questionnaire, but the prevalence of alcohol use disorder in those requiring observation for intoxication is likely high. Those who screen positive can then undergo a brief intervention.
Brief Intervention is a highly empathic interviewing strategy in which the goal is to help the patient draw connections between alcohol use and negative consequences, helping them to connect decreases in alcohol use with achieving their goals. The general approach can be remembered by the mnemonic RULE:
- Resist the righting reflex – patients in the early stages of change will push back and argue against a paternalistic model of communication
- Understand your patient’s motivation – “What do you want your alcohol use to look like? What do you enjoy about using alcohol? What do you enjoy less?”
- Listen with empathy
- Empower the patient – give the patient options that are in line with the patient’s own goals
SBIRT in primary care has a NNT of 8 in preventing risky drinking at the 1 year mark, with a 1:4 ratio in cost to cost savings.11,12 SBIRT in the emergency department has not shown clinically significant decreases in consumption, but there is evidence for a decrease in alcohol-related injury. Likely, some subgroups of patients will respond to an SBIRT approach in the ED and it is the most evidence-based, patient-centered strategy widely utilized.
Treatment in Ottawa
For a referral to treatment, there are three main mechanisms in Ottawa – the rapid access addictions medicine (RAAM) clinics, the Ottawa Withdrawal Management Centre (‘detox’), and Service Access to Recovery Centre, and family doctors. There are similar RAAM clinics easily accessible across the province.
- RAAM clinics were developed to be low barrier walk-in access to physicians and practitioners with addictions medicine training. They generally will initiate treatment with pharmacotherapy and counselling, stabilize, and refer back to the family doctor, or on to longer term resources.
- Detoxification centers are for temporary residential or outpatient symptom control of withdrawal. In Ottawa, the Ottawa Withdrawal Management Centre generally does not have access to medication unless prescribed by an outside physician.
- Service Access to Recovery is an Ottawa/Champlain Local Health Integrative Network (LHIN)-specific centralized intake service to triage and refer patients to local resources. It is the primary method of accessing any residential-type treatment. Other LHINs around Ontario may have similar intake systems.
- For a deeper description of Ottawa specific resources, see the patient handout.
Key Points
- Outpatient benzodiazepines are rarely indicated. If high-risk withdrawal is well-treated in the ED with a loading dose and/or symptom-guided therapy as discussed in Part 1, the risks of oversedation and early relapse outweigh the lack of benefit.
- Gabapentin is a reasonable adjunct after benzodiazepines in the ED. It is efficacious in symptom control and potential benefits with less sedation and relapse than ongoing benzodiazepines. It does not prevent seizures reliably and thus should not be used as monotherapy in patients at high risk of seizure.
- Naltrexone is first-line for treatment of the alcohol use disorder and can be safely initiated in the ED
- The screening, Brief Intervention, and Referral to Treatment (SBIRT) approach may help engage patients and lead to better participation in treatment
- Rapid access addiction medicine clinics are available across Ontario and provide an easy portal of entry for addictions treatment
References
- Sellers EM, Naranjo CA, Harrison M, Devenyi P, Roach C, Sykora K. Diazepam loading: Simplified treatment of alcohol withdrawal. Clin Pharmacol Ther. 1983;34(6):822-826. doi:10.1038/clpt.1983.256
- Devenyi P, Harrison ML. Prevention of alcohol withdrawal seizures with oral diazepam loading. Can Med Assoc J. 1985;132(7):798-800. doi:10.1016/s0022-5347(17)47360-5
- Saitz R. Individualized Treatment for Alcohol Withdrawal. Jama. 1994;272(7):519. doi:10.1001/jama.1994.03520070039035
- Anton RF, Latham P, Voronin K, et al. Efficacy of Gabapentin for the Treatment of Alcohol Use Disorder in Patients With Alcohol Withdrawal Symptoms: A Randomized Clinical Trial. JAMA Intern Med. March 2020. doi:10.1001/jamainternmed.2020.0249
- Myrick H, Malcolm R, Randall PK, et al. A double-blind trial of gabapentin versus lorazepam in the treatment of alcohol withdrawal. Alcohol Clin Exp Res. 2009;33(9):1582-1588. doi:10.1111/j.1530-0277.2009.00986.x
- Writing Group Victor Reus GI, Laura Fochtmann CJ, Bukstein O, et al. THE AMERICAN PSYCHIATRIC ASSOCIATION PRACTICE GUIDELINE FOR THE Pharmacological Treatment of Patients With Alcohol Use Disorder Systematic Review Group Steering Committee on Practice Guidelines APA Assembly Liaisons Chair of Area Liaisons. 2018. https://psychiatryonline.org/doi/pdf/10.1176/appi.books.9781615371969.
- Mason BJ, Quello S, Goodell V, Shadan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence a randomized clinical trial. JAMA Intern Med. 2014;174(1):70-77. doi:10.1001/jamainternmed.2013.11950
- Leung JG, Hall-Flavin D, Nelson S, Schmidt KA, Schak KM. Role of gabapentin in the management of alcohol withdrawal and dependence. Ann Pharmacother. 2015;49(8):897-906. doi:10.1177/1060028015585849
- Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for Adults With Alcohol Use Disorders in Outpatient Settings: A Systematic Review and Meta-analysis. JAMA. 2014;311(18):1889-1900. doi:10.1001/jama.2014.3628
- METAPHI. Protocols for alcohol- and opioid-related presentations. 2019;(June). https://www.metaphi.ca/assets/documents/provider tools/ED_Protocols.pdf.
- Fleming MF, Mundt MP, French MT, Manwell LB, Stauffacher EA, Barry KL. Brief Physician Advice for Problem Drinkers: Long-Term Efficacy and Benefit-Cost Analysis. Alcohol Clin Exp Res. 2002;26(1):36-43. doi:10.1111/j.1530-0277.2002.tb02429.x
- Schmidt CS, Schulte B, Seo H-N, et al. Meta-analysis on the effectiveness of alcohol screening with brief interventions for patients in emergency care settings. Addiction. 2016;111(5):783-794. doi:10.1111/add.13263

