

- There are 35,000 out-of-hospital cardiac arrests (OHCA) annually in Canada6.
- Patient survival in OHCA increases dramatically with resuscitation; bystander CPR, use of AEDs and activation of EMS.
- Signifiant gains have been made with education at both the community and prehospital care level. Despite this, less than 40% of patients with OHCA receive CPR and only 25% have an AED applied by a lay person.
- Of the patients who survive OHCA, more than 90% will not survive to discharge from hospital.
Resuscitation Guidelines
-
- The International Liaison Committee on Resuscitation (or ILCOR) was formed in 1992 as an international council.
- There are multiple representatives from various national councils, such as the Heart and Stroke Foundation of Canada, American Heart Association and the European Resuscitation Council that sit on the ILCOR council.
- The goal of ILCOR is to disseminate and implement evidence surrounding resuscitation and first aid by using consensus summaries of scientific data. Its most recent publication was in 20207.

ILCOR.org
- We are unlikely to see frequent major changes to guidelines moving forward in newly published recommendations.
- Guidelines to resuscitation medicine had previously been updated intermittently, traditionally every 5 years.
- In 2015, ILCOR began a continuous evidence evaluation process, leading to the creation of continuous recommendations.
- The Heart & Stroke Foundation of Canada and the American Heart Association work together to develop North American Guidelines.
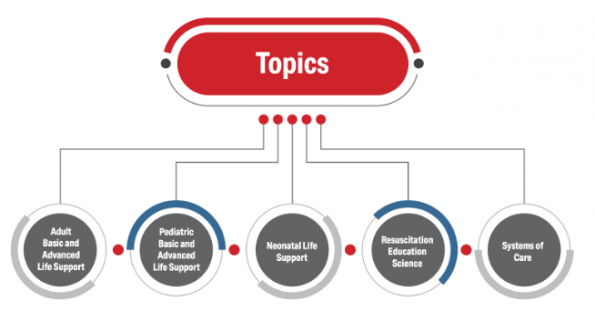
- The 2020 ILCOR/AHA guidelines cover 5 core topics. They provide recommendations for providers and instructors.
- These guidelines cover BLS and ALS for adults and pediatric patients, neonatal life support, resuscitation education and systems of care12.
2020 AHA Guidelines
This post will focus on some of the more controversial guidelines in the new adult ACLS guidelines, published by ILCOR in 2020.
- Dual Sequential Defibrillation (DSD) in shock refractory VF
- PoCUS as a prognostic tool in non-shockable cardiac arrests
- Epinephrine in cardiac arrests
-
-
We will aim to provide insight into some of the current and emerging literature on the above topics, to help contextualize the recommendations and practice moving forward.
Dual Sequential Defibrillation in Shock Refractory VF Resuscitation
2020 AHA guidelines: “The usefulness of double sequential defibrillation (DSD) for refractory shockable rhythm has NOT been established” (Class 2b)12
2020 ILCOR guidelines: “We suggest AGAINST routine use of dual sequential defibrillation (DSD) strategy in comparison with a standard defibrillation strategy for cardiac arrest with a shockable rhythm.” (weak recommendation, very low-certainty evidence)7
-
- The above recommendations are based on a 2020 ILCOR systematic review which found no evidence to support double sequential defibrillation, mostly based on the low quality evidence that is currently available7.
- Patients with shockable rhythms have a much higher change of survival in comparison to patients with a PEA or asystolic arrest.
- 10% of patients with shockable rhythms develop shock refractory VF. 10% of these patients will survive, in comparison to 30% survival in shock responsive patients.
- Multiple definitions of shock refractory VF exist. A commonly accepted definition is that shock refractory VF is ventricular fibrillation that is resistant to at least 3 doses of epinephrine, 300mg of amiodarone and 3 defibrillation attempts without spontaneous circulation (ROSC) after > 10 min of CPR.
- Unfortunately there are no clear guidelines or ACLS algorithms that have been published on how to best manage shock refractory VF.
- Dr. Lindsay Cheskes, covered this extensively in an excellent BLOG POST and discussed therapies for shock refractory VF that go beyond ACLS guidelines. Dr. Lindsay Cheskes specifically recommends holding administration of additional doses of epinephrine, trialing esmolol, in addition to using dual sequential defibrillation.

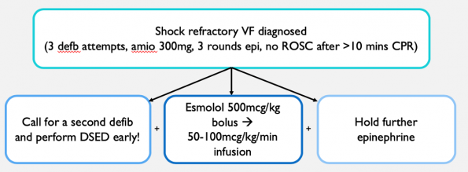
Dr. Cheskes’ Algorithm for Shock Refractory VF
-
- What is DSD? It is a method of delivering two shocks in sequence from 2 different defibrillators.
- There are various theories behind DSD:
- Delivering 2 shock increases the total energy delivered to the myocardium.
- Using two sets of pads provides additional energy vectors.
- The first shock delivered may lower the defibrillation threshold, thus potentially increasing the success rate from the second shock delivered in sequence.
- Pads are typically placed in one of two different orientations in DSD: (1) both pairs of pads are placed anterolaterally (image to the left) or (2) one set of pads placed anteroposteriorly and the second anterolaterally (image to the right).
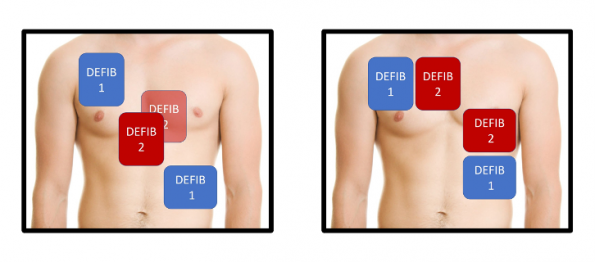
Pad placement for DSD. Image from Dr. Mark Ramzy (@MRamzyDO) from EMCrit: https://emcrit.org/emcrit/double-defibrillation/
Observational Study
Only until recently, evidence available around the use of dual sequential defibrillation was observational. The best evidence available regarding the use of DSD was a study published by Cheskes et al (2019)4. This was a retrospective observational study of 252 OHCA patients with refractory VF in 4 Canadian paramedic services. In this trial, they compared outcomes between two types of defibrillation: (1) standard defibrillation and (2) dual sequential defibrillation. They looked to compare the rates of VF termination and VF termination to ROSC with both defibrillation strategies.
Results: When comparing standard and dual sequential defibrillation, they found that overall they were EQUALLY successful in TERMINATING shock refractory VF by either obtaining ROSC (21.4% vs. 17.6%; RR 0.8; 95% CI: 0.4-1.6) or converting to PEA or asystole (78.1% vs 76.5%; RR 1.0; 95% CI 0.8-1.2). In earlier defibrillation attempts (shock attempts 4-8), DSD was much more successful in obtaining ROSC when compared to the standard defibrillation group (15.7% vs 5.4%; RR 2.9, 95% CI 1.4-5.9). With increasing defibrillation attempts, this benefit was lost and standard defibrillation was just as effective as DSD. Although this was purely observational and did not assess patient centred outcomes such as neurologic recovery, they did identify that DSD is likely most beneficial when performed early in the resuscitation.
DOSE-VF Trial
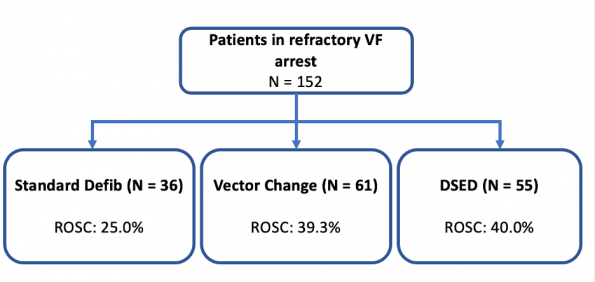
Recently, a new RCT named the DOSE-VF trial (Cheskes et al. 2020) was started3. Although this study is currently in progress, they published the results from the pilot of this RCT in 2020. The goal for this pilot was to assess the feasibility and safety of the study protocol. It is a pre-hospital, multi-center cluster RCT comparing standard defibrillation (SD), dual sequential external defibrillation (DSD) and vector change external defibrillation (VC) in patients with OCHA presenting in shock refractory VF. The primary outcome measure of this study will be survival to discharge. Even though this pilot was meant to look at the feasibility of the trial, it provided a glimpse into some of the preliminary data surrounding the various treatment arms.
Overall, we can appreciate a trend that VC and DSD have higher rates of obtaining ROSC when compared to standard defibrillation. DSD and VC were able to obtain ROSC in 40.0% and 39.3% of patients in contrast to standard defibrillation (which had a rate of 25.0%). Note, that this preliminary data should be interpreted with caution as it was a pilot study – therefore, it is not powered to look at patient centre outcomes.
Bottom Line
Dual sequential defibrillation is likely safe. Based on the evidence currently available, it is probably more effective than standard defibrillation and is most effective when performed early in shock refractory VF. In resource poor settings where DSD may not be feasible, changing the pad placement/vectors (VC) may be just as effective as DSD.
PoCUS as a Prognostic Tool in Non-shockable Cardiac Arrest
2020 AHA Guideline: “We suggest AGAINST the use of PoCUS for prognostication during CPR” (Class 3: No Benefit)12.
REASON Study
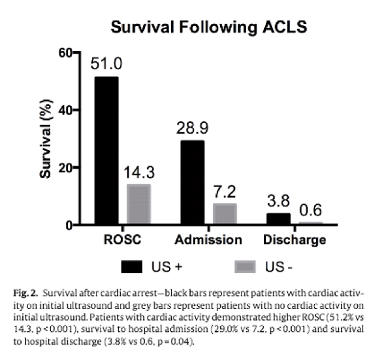
The REASON Study (Gaspari et al. 2016) was a non-randomized, prospective, non-blinded, convenience sample of 798 ED patients with non traumatic PEA or asystolic cardiac arrests5. The primary outcome was survival to admission and secondary outcomes included survival to hospital discharge and ROSC. Patients needed to have received at least 1 round of ACLS drugs. The initial PoCUS was performed and repeated during pulse checks using parasternal or substernal views.
They found a statistically significant difference for all 3 outcomes: ROSC, survival to admission and survival to discharge. Overall, patients who had cardiac activity on POCUS had a 51% chance of achieving ROSC, versus 14.3% if there was no cardiac activity. Only 3.8% of patients who had cardiac activity survived to hospital discharge. If there was no cardiac activity seen on PoCUS, only 0.6% of patients survived to hospital discharge.
Based on the rest of their results, the authors concluded that cardiac activity on ultrasound was the variable most associated with survival following cardiac arrest. Surprisingly, it was even more reliable than the presence of bystander CPR in predicting these outcomes.
SHoC-ED Study
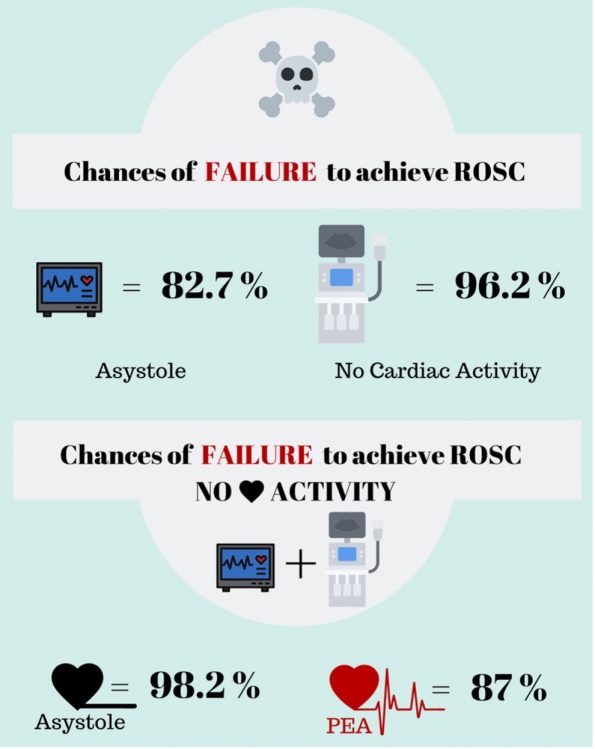
This study (Beckett et. al, 2019) was an observational study published in CJEM2. The authors assessed the prognostic value of PoCUS in comparison to rhythm analysis. They also looked to see if combining PoCUS and ECG rhythm findings together better predicted poor outcomes in cardiac arrest. This was a health records review of 180 cases of patients with OHCA with non-shockable rhythms. Their primary outcomes included ROSC, survival to hospital admission and survival to hospital discharge.
When using ECG alone, patients in asystole had an 82.7% chance of not achieving ROSC. PoCUS when used alone performed better with a sensitivity of 96.2% for failure to achieve ROSC. PoCUS performed better than ECG rhythm in all 3 outcomes of the study. When the patient’s rhythm was asystole and there was no cardiac activity on PoCUS, these patients had a 98.2% chance of NOT achieving ROSC. Of these patients, only 0.8% survived to discharge.
Sensitivity of initial ECG rhythm, initial PoCUS findings overall, and PoCUS findings in patients with ECG asystole, and PEA, for the prediction of no ROSC. (Lalande et al. 2019)
Bottom Line
PoCUS is much better at predicting death than survival in patients with non-shockable cardiac arrests. The chance of survival to discharge for patients in asystole with absence of cardiac activity on PoCUS is less than 1% whereas the chance of obtaining ROSC is 50% in those with cardiac activity. This information should be used as a tool to further risk stratify cardiac arrest patients in addition to other prognostic variables.
Epinephrine in Cardiac Arrest Resuscitation
2020 ILCOR guideline: “We RECOMMEND administration of epinephrine during CPR.” (strong recommendation, low to moderate certainty of evidence)7
-
- It is universally accepted that epinephrine increases the likelihood of ROSC in cardiac arrests.
- There is an emerging philosophical discussion within the medical community around whether epinephrine may be harming patients by increasing their likelihood of having poor neurologic recovery.
PACA Trial
This trial (Jacobs et al., 2011) was conducted in Australia and New Zealand8. It was a double-blind randomized placebo-controlled trial of epinephrine in 534 adults with OHCA. They compared epinephrine to placebo. Their primary outcome was survival to hospital discharge and secondary outcomes included ROSC and neurologic outcomes.
Unsurprisingly, they found a significant increase in ROSC with epinephrine versus placebo (23.5% vs 8.4%). Unfortunately, this study ended early due to ethical concerns and ultimately was underpowered to asses patient-centred outcomes such as neurologic recovery.
PARAMEDIC2 Trial

The PARAMEDIC2 Trial (Perkins et al. 2018)
This was a multi-centre, randomized, double-blind, placebo controlled trial of 8014 patients with OHCA in the UK14. They compared IV epinephrine to saline boluses. Their primary outcome was survival t 30 days. There were multiple secondary outcomes, most notably survival to hospital discharge and favorable neurologic recovery.
Unsurprisingly they found a significant increase in the rate of ROSC in the epinephrine group in comparison tot he placebo (36.3% vs 11.7%). In the epinephrine group, 31.0% of survivors had a poor neurologic outcome, compared to 17.8% in the placebo group. Overall, in this study the authors found that the use of epinephrine increased the rates of ROSC but came at the cost of more ICU days, severe neurologic disabilities, and no difference in survival with favorable neurologic outcome compared to placebo.
PACA and PARAMEDIC-2 Meta-analysis
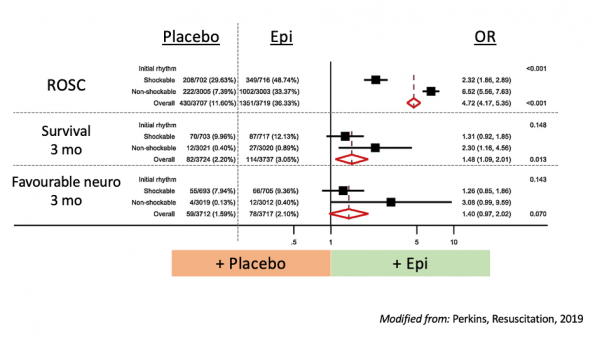
A meta-analysis was performed with the goal of assessing the effect of the initial arrest rhythm on the outcomes of the PARAMEDIC2 and PACA trials (Perkins et al., 2019).
When assessing ROSC, as expected, they found a combined OR of 4.7 favouring epinephrine. Patients with shockable rhythms had a much lower OR of obtained ROSC in comparison to those with non-shockable rhythms. A similar trend could be seen for survival and favorable neurologic outcomes at 3 months, although most of the results were not found to be statistically significant. Overall, what we can conclude is that relative to placebo, the effects of epinephrine on ROSC appear to be greater for patients with a non-shockable rhythm. There are similar patterns for long term survival and favourable neurologic recovery, but the difference in effect is less significant.
-
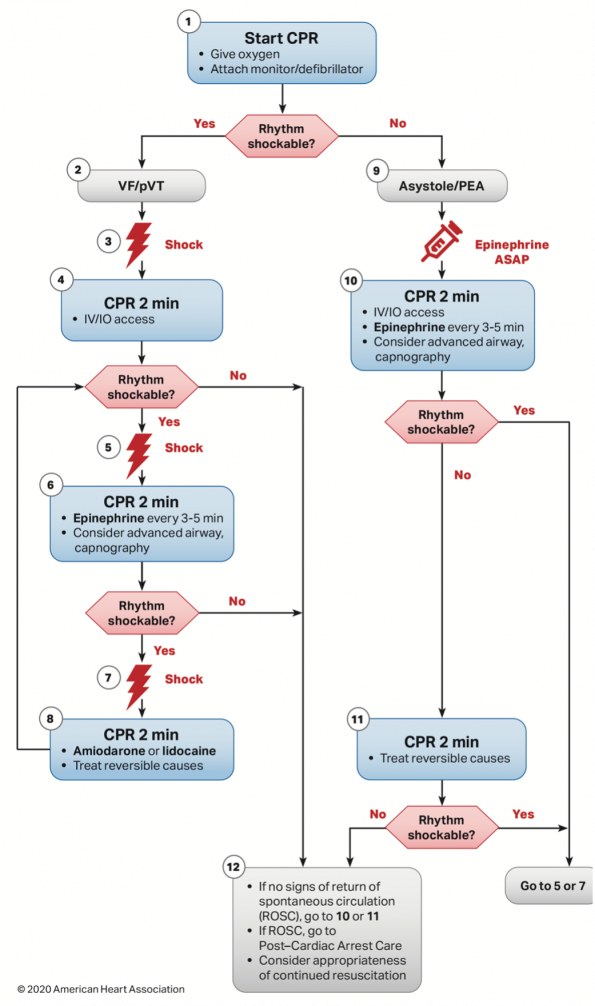
- Based on meta-analyses, ILCOR released the following guideline: “For non-shockable rhythms (pulseless electrical activity/asystole), we recommend administration of epinephrine as soon as feasible during CPR” (strong recommendation, very-low certainty of evidence)7.
- To reflect this recommendation, a new algorithm for cardiac arrests was released to emphasize the importance of administering epinephrine early in cardiac arrests with non-shockable rhythms.
Bottom Line:
Epinephrine in cardiac arrests should be used with caution. Although it overall increases survival, it also significantly increases poor neurologic recovery. Patient with non-shockable rhythms likely benefit most from epinephrine, which should be administered as early as possible in this subgroup.
Take Home Points
In summary, review of the current literature surrounding three aspects of the new ILCOR 2020 Guidelines, has led us to draw the following conclusions:
(1) Dual Sequential Defibrillation (DSD): According to ILCOR, DSD is not recommended due to poor evidence on the subject. However, preliminary data from the DOSE-VF trial demonstrates that DSD is likely safe, and possibly more effective than standard defibrillation when used early in shock refractory VF.
(2) PoCUS during Cardiac Arrest: Although not recommended for use by ILCOR guidelines for prognostication during CPR, evidence suggests that POCUS is quite reliable in predicting likelihood of death. It could play a role as an additional data point to assist risk stratification during cardiac arrest.
(3) Epinephrine use in PEA/Asystole: Early epinephrine use is most beneficial in the non-shockable subgroup. Overall excessive use of epinephrine should be done with caution, as poor neurological outcomes may be encountered.
References
- Beck L, Ostermayer D, Ponce J, Srinivasan S, Wang H. Effectiveness of prehospital dual sequential defibrillation for refractory ventricular fibrillation and ventricular tachycardia cardiac arrest. Prehospital emergency care. 2019.
- Beckett N, Atkinson P, Fraser J, Banerjee A, French J, Talbot J-A, Stoica G, Lewis D. Do combined ultrasound and electrocardiogram-rhythm findings predicts survival in emergency department cardiac arrest patients? The Second Sonography in Hypotension and Cardiac Arrest in the Emergency Department (SHoC-ED2) Study. CJEM. 2019
- Cheskes S, Dorian P, Feldman M, et al. DOuble Sequential External Defibrillation for Refractory Ventricular Fibrillation: The DOSE VF Pilot Randomized Controlled Trial. Resuscitation. 2020
- Cheskes, S., Wudwud, A., Turner, L., McLeod, S., Summers, J., Morrison, L. J., & Verbeek, P. R. (2019). The impact of double sequential external defibrillation on termination of refractory ventricular fibrillation during out-of-hospital cardiac arrest. Resuscitation, 139, 275-281.
- Gaspari R, Weeke A, Adhikari S, Noble V, Nomura J, Theodoro D, et al. Emergency department point-of-care ultrasound in out-of-hospital and in-ED cardiac arrest. Resuscitation. 2016.
- Highlights of the 2020 American Heart Association Guidelines for CPR and ECC. Heart & Stroke Foundation of Canada Edition. 2020.
- International Liaison Committee on Resuscitation. 2020 International consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Resuscitation. 2020.
- Jacobs I, Finn J, Jelinek G, Oxer H, Thompson P. Effect of adrenaline on survival in out-of-hospital cardiac arrest: a randomised double-blind placebo-controlled trial. Resuscitation. 2011.
- Kedan I, Ciozda W, Palatinus J, Palatinus H, Kimchi A. Prognostic value of point-of-care ultrasound during cardiac arrest: a systematic review. Cardiovascular Ultrasound. 2020.
- Kim H, Suh J, Choi J, Cho Y. Can serial focused echocardiographic evaluation in life support (FEEL) predict resuscitation outcome or termination or resuscitation (TOR) A pilot study. Resuscitation. 2016.
- Lanlande E, Woo M. POCUS predicts prognosis in cardiac arrest. CJEM. 2019.
- Merchant R, Topjian A, Panchal A, et. Part 1: executive summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020
- Morgenstern J, “Epinephrine in out of hospital cardiac arrest: a review of all the evidence”, First10EM blog, November 6, 2018. Available from: https://first10em.com/epinephrine/
- Perkins G, Ji C, Deakin C, Quinn T, Nolan J, Scomparin C, Regan S, Long J, Slowther A, Pocock H, Black J, Moore F, Fothergill R, Rees N, O’Shea L, Docherty M, Gunson I, Han K, Charlton K, Finn J, Petrou S, Stallard N, Gates S, Lall R. A randomized trial of epinephrine in out-of-hospital cardiac arrest. 2018.
- Perkins G, Kenna C, Ji C, Deaking C, Nolan J, Quinn T, Fothergill R, Gunson I, Pocock H, Rees N, Charlton K, Finn J, Gates S, Lall R. The effects of adrenaline in out of hospital cardiac arrest eith shockable and non-shockable rhythms: Findings from the PACA and PARAMEDIC-2 randomised controlled trials. Resuscitation. 2019.
- Ross E, Redman T, Harper S, Mapp J, Wampler D, Miramontes D. Dual defibrillation in out-of-hospital cardiac arrest: A retrospective cohort analysis. Resuscitation. 2016.

