

Pediatric mental health complaints are common presentations to the emergency department. Many providers are comfortable managing symptoms of depression, anxiety, suicidality. But what about pediatric patients with severe agitation and aggression? Between 6 and 10% of pediatric mental health ED visits require restraint. Do we even do that? How do we do it? Should we use drugs? Can we use the same medications we’d use in an adult?
This post aims to familiarize readers with simple non-pharmacologic interventions, and to provide guidance on how to choose the right medication for the right pediatric patient, presenting with agitation or aggression to the emergency department.
Non-pharmacological Interventions
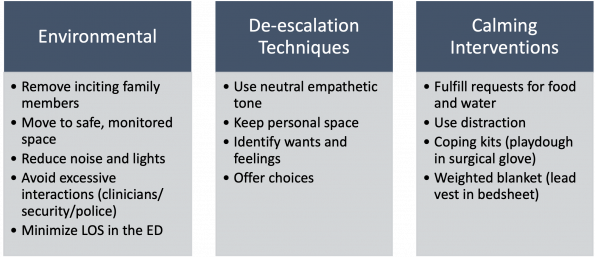
All pediatric patients with acute agitation and aggression should receive multi-modal non-restraining interventions as the baseline therapy, if it is safe to do so. There are three categories summarized in the literature:
Physical Restraint
This section really should appear at the end of the blog post because it is a last resort during the most acute safety threats. Physical restraint of pediatric patients should be undertaken with the highest degree of caution and care. Patients may be brought in by police and it’s important for the medical team to ensure clear communication with police that our goal in the ED is to emphasize environmental and pharmacologic strategies in children to avoid, to the greatest allowable degree, the physical and psychological harm that can be associated with physical restraint of pediatric patients. Primum non nocere. Physical restraint in children (or in adults) should always employ the minimum amount of force necessary and be medically justified. Any force beyond what is necessary is technically assault.
Non-pharmacological take-aways:
- When it is safe, use a combination of environmental modifications, verbal de-escalation, and calming interventions to decrease the need for chemical or physical restraint.
- Longer ED length of stay is associated with increased odds of a code white activation. Please see these patients ASAP.
- Physical restraint is used as a last resort when environmental and pharmacological strategies have failed, are impossible or unsafe.
Medications
When situations escalate, and non-pharmacologic strategies have failed or are not appropriate, it’s time for medications. Physicians should make deliberate selections of sedating medications that are tailored to the patient and the etiology of their agitation. Understanding your patient’s history is crucial because the pathophysiology and susceptibility to adverse drug reactions are different in pediatric patients, compared to adults.
Causes of pediatric agitation are varied and so the mantra “etiology drives decision” should guide providers when choosing which drugs to administer pediatric patients who are dangerously agitated, or at risk of becoming so.
A note about PO medications…
It may surprise some providers, but many of even the most heightened or agitated pediatrics patients will accept an oral medication. If it is offered by a familiar caregiver, and the child is told it will help calm them, very few reject them. Oral dissolving tabs (ODT) are excellent if your hospital has them. Set the expectations of the nurse and parent that the onset time is expected to be slower than IM medications and that IM medications may become necessary if oral medications fail. If the situation allows, oral medications should be first line to injectables in pediatric mental health emergencies.
Etiologies for special consideration…
In general, pediatric patients presenting with intoxication (or withdrawal) or psychosis may be treated with similar medication strategies as adults. This group will be discussed at the end of the section. There are, however, three groups of patients in pediatrics who required special care when administering medication for rapid tranquilization. They are:
- Autism spectrum disorder (ASD)
- Oppositional defiant disorder/behavioural dysregulation and,
- Pediatric delirium/encephalopathy
Autism Spectrum Disorder
Patients with ASD have unique triggers for agitation. When severe, their underlying condition makes their assessment very difficult and, when agitated, sometimes impossible. The most common trigger of agitation in patients with ASD is pain. In non-verbal ASD children, the three most common causes of pain are: 1) dental, 2) constipation, and 3) headache, though clinicians should examine each system diligently for evidence of an unrecognized painful process.
Some practitioners treat with empiric analgesia (acetaminophen/ibuprofen), which is very reasonable, but the role of sedating and calming medications cannot be understated. Safe sedation to both calm the patient safely and to enable a thorough physical exam is essential to making the diagnosis.
There are two important factors to consider when choosing medications:
- Avoid benzodiazepines and diphenhydramine, as young and neuroatypical children are at greatest risk for experiencing paradoxical agitation.
- Offer oral medications before injectables. You may be surprised at how accepting these patients are of oral medications, especially if a family caregiver is administering them. Use oral dissolving tabs (ODT) if your facility has them.
ASD Take-Aways:
- Consider an undiagnosed source of pain in children with ASD presenting with new agitation. You can give empiric analgesia.
- Avoid benzodiazepines and diphenhydramine, as these patients are at risk of paradoxical agitation.
- First line:
- Olanzapine ODT/PO
- Risperidone ODT/PO
- Doses included in table at end of blog post
- If injectable medication is required for safety of a medically necessary exam or procedure:
- Olanzapine IM
Oppositional Defiant Disorder/Behavioural Dysregulation
Patients with ODD or severe behavioural dysregulation often present when parents have tried everything they can think of and ‘don’t know what to do anymore’. When treating patients who may appear to be having a tantrum to end all tantrums, there are few medication choices that are wrong. If a patient is currently taking a medication at home, a good first step is giving an extra dose of their own medication.
If this fails, or is not possible, there are several choices that are all reasonable, and there is no consensus among experts for which medication is best. As with patients who have ASD, oral medications should be offered/attempted prior to injectables, if appropriate. Clinicians may choose from any of antipsychotics, benzodiazepines, or alpha agonists.
When it comes time to use injectables, many practitioners may reach for lorazepam or haloperidol. Both medications work well, but consider adding olanzapine to your list, if it’s not already on there. A study of youth admitted to psychiatry found that olanzapine has a faster onset compared lorazepam. In head-to-head comparisons with haloperidol, olanzapine was 12 minutes faster (11 vs 23 min), with no difference in efficacy. Midazolam was fastest (8 min), and a reasonable choice, but in pediatrics has an increased risk of paradoxical agitation. Olanzapine carries a lower risk of EPS relative to haloperidol, but doesn’t last as long as and may require additional dosing within the first hour of administration. Olanzapine should not be given within an hour of a benzodiazepine in children, due to increased risk of respiratory depression.
ODD Take-Aways:
- Give an extra dose of the patient’s own sedating medication.
- If not available, or ineffective:
- Olanzapine ODT/PO
- Risperidone ODT/PO
- Clonidine PO
- Lorazepam PO/SL
- Doses included in table at end of blog post
- If injectable medication is required, use either but never both, of:
- Olanzapine IM
- Midazolam or lorazepam IM
- See Table 2 at end of blog post for doses
- Do not give olanzapine within 1 hour of a benzodiazepine, as it increases the risk of respiratory depression.
Delirium/Encephalopathy
Delirium is very rare in the pediatric ED and should raise concern for organic CNS infection, autoimmune disease, or medication reaction. The most common medications causing delirium are benzodiazepines, opioids and anti-cholinergics. A complete medical work up must be undertaken and if a patient cannot be thoroughly investigated (often with MRI brain, lumbar puncture, and pediatric neurology consultation) they should be transferred to a pediatric centre.
As with adults, pediatric delirium can present with hypoactive, hyperactive or mixed states. If a patient is severely altered and agitated, the consensus recommendation is to treat with anti-psychotics and to avoid benzodiazepines. Haloperidol has largely been replaced by second generation neuroleptics and, of these, olanzapine, quetiapine and risperidone are the most commonly used medications in pediatric delirium. In a retrospective review of pediatric agitated delirium cases treated with haloperidol, 23% experienced acute dystonia, which the authors conclude made haloperidol therapy ‘fraught with difficulty’. Extra-pyramidal symptoms, like dystonia, are treated effectively in pediatrics as they are in adults, but why make your shift fraught with difficulty if you can avoid it with a lower risk medication?
Pediatric Delirium/Encephalopathy Take-Aways:
- Pediatric delirium requires complete work-up for organic CNS infection, autoimmune or metabolic disease.
- Review history for, and avoid administering, benzodiazepines, anti-cholingerics, and opiates.
- If mild sedaion is required, use:
- Olanzapine ODT/PO
- Risperidone ODT/PO
- Quetiapine PO
- If rapid tranquilization is required, use:
- Olanzapine IM
Psychosis and Intoxication
In general, cases of pediatric (most often adolescent) psychosis and intoxication do not have features that make them particularly unique from adult cases. However, primary psychotic disorders in pediatrics are rare, and so a full neurologic, as well as psychiatric, assessment should be undertaken.
In practice, chemical sedation is often achieved with benzodiazepines and/or neuroleptic medications, most commonly haloperidol. There is consensus recommendations to not give olanzapine with benzodiazepines in this population, and so the old 5 and 2 combination (haloperidol and lorazepam) prevails when rapid tranquilization is urgently needed. This is still the standard of care for pediatric patients, even in undifferentiated intoxication causing aggression. Interestingly, there is emerging evidence for the efficacy and safety of IM ketamine for rapid agitation control in adults. Check out the EMOttawa blog post by Drs. Adam and Rosenberg, for their review of an RCT published in Annals of Emergency Medicine in 2021.
In pediatrics for agitation, ketamine has yet to find it’s way into evidence based practice due to a paucity of research and concerns of psychosis in undifferentiated pediatric patients with mental health complaints.
Medication Doses
| Oral Medications | ||
| Olanzapine ODT/PO
|
Under 12 years
2.5 mg/dose |
12 years and older
5 mg – 10 mg/dose |
| Risperidone ODT/PO
|
Under 12 years
0.5 mg – 1.0 mg/dose |
12 years and older
1 mg – 2 mg/dose |
| Clonidine PO | 0.05 – 0.1 mg/dose | |
| Lorazepam PO/SL | 0.05 – 1.0 mg/kg/dose
MAX 4 mg |
|
| Quetiapine PO | 1.0 – 1.5 mg/kg/dose
MAX 50 mg |
|
| Injectable Medications | ||
| Olanzapine IM
25% – 50% of PO dose |
Under 12 years
2.5 – 5 mg/dose |
12 year and older
5 – 10 mg/dose |
| Haloperidol IM | Under 12 years
1 – 3 mg/dose |
12 years and older
2.5 – 5 mg/dose |
| Midazolam IM | Under 5 years
0.1 mg – 0.15 mg/kg/dose MAX 6 mg |
5 years and older
0.025 – 0.05 mg/kg/dose MAX 10 mg |
References:
- Dorfman DH, Kastner B. The use of restraint for pediatric psychiatric patients in emergency departments. Pediatr Emerg Care. 2004;20(3):151-156. doi:10.1097/01.pec.0000117921.65522.fd
- Dorfman DH, Mehta SD. Restraint use for psychiatric patients in the pediatric emergency department. Pediatr Emerg Care. 2006;22(1):7-12. doi:10.1097/01.pec.0000195758.12447.69
- Gerson R, Malas N, Mroczkowski MM. Crisis in the Emergency Department: The Evaluation and Management of Acute Agitation in Children and Adolescents. Child Adolesc Psychiatr Clin N Am. 2018;27(3):367-386. doi:10.1016/j.chc.2018.02.002
- Gerson R, Malas N, Feuer V, Silver GH, Prasad R, Mroczkowski MM. Best Practices for Evaluation and Treatment of Agitated Children and Adolescents (BETA) in the Emergency Department: Consensus Statement of the American Association for Emergency Psychiatry. West J Emerg Med. 2019;20(2):409-418. doi:10.5811/westjem.2019.1.41344
- Carison A, Babl FE, Hill A, O’Donnell SM. Children and adolescents with severe acute behavioural disturbance in the emergency department. Emerg Med Australas EMA. 2020;32(5):747-755. doi:10.1111/1742-6723.13515
- Mancuso CE, Tanzi MG, Gabay M. Paradoxical reactions to benzodiazepines: literature review and treatment options. Pharmacotherapy. 2004;24(9):1177-1185. doi:10.1592/phco.24.13.1177.38089
- Swart GT, Siman E, Stewart SL. The use of Pro Re Nata or Statim medications for behavioral control: a summary of experience at a tertiary care children’s mental health center. J Child Adolesc Psychopharmacol. 2011;21(1):67-77. doi:10.1089/cap.2010.0010
- Chan EW, Lao KSJ, Lam L, et al. Intramuscular midazolam, olanzapine, or haloperidol for the management of acute agitation: A multi-centre, double-blind, randomised clinical trial. EClinicalMedicine. 2021;32:100751. doi:10.1016/j.eclinm.2021.100751
- Turkel SB, Tavaré CJ. Delirium in children and adolescents. J Neuropsychiatry Clin Neurosci. 2003;15(4):431-435. doi:10.1176/jnp.15.4.431
- Thom RP. Pediatric Delirium. Am J Psychiatry Resid J. 2017;12(2):6-8. doi:10.1176/appi.ajp-rj.2017.120203
- Joyce C, Witcher R, Herrup E, et al. Evaluation of the Safety of Quetiapine in Treating Delirium in Critically Ill Children: A Retrospective Review. J Child Adolesc Psychopharmacol. 2015;25(9):666-670. doi:10.1089/cap.2015.0093
- Ratcliff SL, Meyer WJ, Cuervo LJ, Villarreal C, Thomas CR, Herndon DN. The use of haloperidol and associated complications in the agitated, acutely ill pediatric burn patient. J Burn Care Rehabil. 2004;25(6):472-478. doi:10.1097/01.bcr.0000144540.21272.2c
- Barbic D, Andolfatto G, Grunau B, et al. Rapid Agitation Control With Ketamine in the Emergency Department: A Blinded, Randomized Controlled Trial. Ann Emerg Med. 2021;78(6):788-795. doi:10.1016/j.annemergmed.2021.05.023
Is the lorazepam PO dose correct?