

Previously in Part One, we reviewed the pathophysiology and pre-hospital management of patients who experienced non-fatal and fatal drownings. Now, in Part Two, let’s take a deeper dive into the resuscitation of these patients in the Emergency Department as well as general management for these patients.
- Drowning Resuscitation
- Prognostication
- Secondary Drowning and the Well-Appearing Patient
- Wilderness Medicine Survival Strategies

Drowning Resuscitation
We won’t review standard ACLS care as it applies to the arrested patient. Instead, below are core nuances you should know when managing your next drowning resuscitation patient.
Airway
Expect it to be soiled given the aspiration that occurs while drowning and that vomiting is documented in up to 86% of drowning victims requiring CPR.[1] This compounds the degree of respiratory difficulty and likelihood of ARDS. If intubating, consider using a SALAD (Suction Assisted Laryngoscopy and Airway Decontamination) technique.[2]
NG/OG Decompression Post-Intubation
When you’ve secured the airway, and if you’re not running an active code, all these drowning patients need an orogastric or nasogastric tube placed post-intubation. Drowning victims swallow more water than they aspirate, and gastric distention from positive-pressure ventilation is common.[1]
Breathing
Follow an ARDS protocol and prime your RT to expect this. In brief, this involves increasing PEEP to achieve adequate oxygenation, and using a low TV ventilation strategy.[3]
Cervical Collars
C-collar are rarely indicated for the drowning patients. The largest study to date examined 2,244 submersion victims and found only 11 (0.5%) to have c-spine injuries.[4] All 11 patients had obvious signs of injury and a mechanism consistent with spinal trauma. That is, a history of diving, MVC or fall from height. If your patient does not fall into one of these categories, a c-collar is likely not indicated and clinical judgment can be used on a case-by-case basis.
Hypothermia
In drowning, hypothermia isn’t an “if” but a “when” question. The temperature of thermally neutral water, at which heat loss balances heat production is 34° C.[5] Comparatively, the temperature of an average indoor lane pool is 26–28° C. Conduction science demonstrates that a person immersed in cold water loses heat 25 times as fast as someone exposed to cold air. All these patients should have a core-temperature obtained and, if hypothermic, rewarmed as per your local institutional protocol.
Electrolyte Abnormalities
There often aren’t any abnormalities in electrolytes. Initial thoughts came from case report of patients drowning in the dead sea. However, canine studies in the 1960s showed you needed an abundance of water to cause any significant electrolyte abnormality.[6] One study instilled up to 44 ml/kg into the trachea of intubated canine. Electrolyte abnormalities and hemodilution occurred only with volumes > 11 ml/kg, which is far more than the average drowning victim aspirates.
Antibiotics
Antibiotics are NOT indicated and shouldn’t be given unless the patient drowns in heavily contaminated water (a.k.a. sewage) – not rivers, lakes, oceans, or even hot tubs.[7] If non-fatal drowning victims go on to develop a pneumonia, its often-rarer organisms including pseudomonas, aeromonas, and atypical fungal infections. This occurs days later, typically day 3-4 in the ventilator dependent patient, and is best addressed by your intensivist colleagues.
Ineffective Therapies
Artificial surfactant, used to replace the washed-out surfactant that occurs during drowning has been trialed in animal models without success.[8] Similarly, pulmonary vasodilators like nitric oxide, steroids, diuresis, and barbiturate coma have all been found ineffective.[9] Ultimately, these interventions are not indicated for general resuscitation of drowning patients.
Prognostication
Perhaps you’ve seen reports of the miraculous recoveries that some drowning victims can have. If you haven’t, here’s a Times Magazine article on a 14-year-old boy who survived 42-minutes underwater.
Many questions come to mind. What are the factors that allowed him to survive? Was if it’s his age? What if it was the water temperature?
Well, a 2020 ILCOR systematic review examined prognostic factors in search-and-rescue operations that could be associated with positive patient outcomes including: ROSC, survival to hospital discharge, survival with good neurologic outcome.[10] The six factors studied were:
- Age
- EMS response time
- Water salinity
- Submersion duration
- Water temperature
- Witnessed status
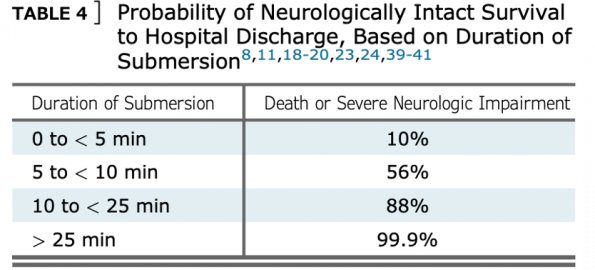
They found that only submersion duration had reliable evidence as a prognostic indicator for making management decisions. They advised against using all other factors based on very-low certainty evidence, noting they “excluded exceptional and rare case reports that [identified] good outcomes after prolonged submersion in icy cold water.”
Termination of resuscitation (TOR) is one of the most challenging aspects of our job, and published general guidelines exist to support decision making. Regarding submersion duration, see the below table from a 2021 CHEST Systematic Review.[11]
The Well-Appearing Drowning Patient
|
I recently cared for an 8-year-old boy brought by mother after swallowing hot-tub water. He wasn’t submerged more than 10-seconds, never vomited, but had an intermittent dry-cough. He had normal vitals and a clear chest on physical exam. The mother noted concerns from a friend’s friend on secondary drowning and risk of nocturnal death. Take a moment to think through your management. Do you obtain a chest x-ray? Observe for a standardized period? Discharge home with reassurance? And does secondary drowning exist? |
 |
A recent scoping review identified five articles on ED observation for the well-appearing drowning patient including criteria to safely predict discharge.[12] They found a 6-hour observation period (from time of event) was sufficient if the following three criteria were met:
- Normal mentation
- Normal age-adjusted vital signs
- Never required supplemental O2
Chest x-ray has not been reliably found to correlate with clinical outcomes and should only be considered for an abnormal lung examination or oxygen saturation.[13]
Secondary Drowning
Let’s agree to stop using this term. It’s outdated and creates unnecessary anxiety.
Consider the following study of 41,279 drowning patients in Rio De Janeiro, Brazil.[14]
In rescued patients with a cough but normal lung exam, there was 0% mortality. Not one single death! Only as symptom severity increased was mortality documented. For example, abnormal pulmonary auscultation with pulmonary field rales averaged 0.6% mortality, and pulmonary edema without hypotension averaged 3.2% mortality.
If the patient in-front of you is well-appearing 6-hours out from the drowning event, with normal vitals and a clear chest, you should confidently reassure them. They will not drown in their sleep! This is a terrifying myth that we should work to dispel.
Wilderness Medicine Survival Strategies
Let’s conclude with survival strategies to three water-based emergencies that can save a life. That of being trapped in a vehicle sinking in water, lost in the ocean, and falling through ice.
Automobile Submersion
Consider the following: Your car has just fallen into the river. Do you:
-
- Attempt to exit the vehicle immediately while it’s still above the surface? OR
- Allow your vehicle to sink to the bottom to maintain orientation and, only when it’s fully submerged, attempt to escape?
The correct answer is to attempt escape immediately during the initial flotation phase.[15] The cabin of the car is filled with air and the car is not expected to sink right away. It will remain above the surface for 30-seconds to upwards of 2-minutes. During this time, remove your seatbelt, open the window, and get out. If you can’t open a window, remove your car’s headrest, and use the metal posts under the headrest to break your side-door window. The front windshield is reinforced glass, so the door windows are best to break, and know that they are weakest at their corners.
A great mnemonic to remember from the Wilderness Medicine guidelines is SWOC.[16]
Seatbelts off;
Windows open;
Out immediately;
Children first.
Lost in the Ocean
Note that this applies to any scenario where you’re stuck out in open water.
The key points are to focus on your breathing, and if you’re going to act, act right away.[16]
After immersion in cold water, you have a very limited period before fatigue and incapacitation render self-rescue impossible, as gross motor skills will quickly decline.
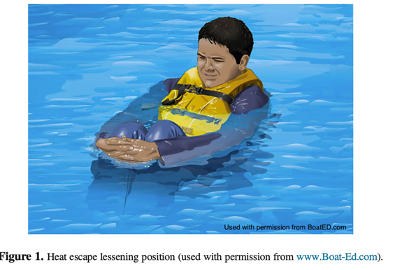
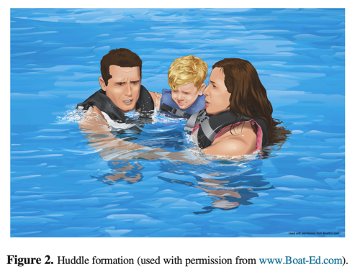
If you’re going to attempt swimming to safety, do this early on. Otherwise, focus on conserving your heat using the Heat Escape Lessening Position (HELP). Laboratory studies have shown the HELP position to decrease heat loss, through focusing on minimizing losses from the axilla, groin, and to a lesser extent the neck. If you’re with other victims, consider using a huddle formation.
Fallen through Ice
Exposure to freezing water triggers a cold shock reflex, with hyperventilation and a potential disorienting effect making self-rescue attempts difficult.[16] Here are the basic steps and considerations for someone who has fallen through the ice:
- First control your breathing by taking slow, deep breaths.
- Be aware that anyone around you is at an increased risk of falling through the ice.
- Call for help immediately, others can seek a rope or a long piece of clothing to help with rescue.
- Resist the urge to climb out on the side you fell through as that’s where the ice if often weakest.
- Kick forward with your legs from the water, with wide arms to increasing surface area attempting a flat torso onto the ice.
- Once out, increase your surface area and minimize focal points of pressure by crawling.
- Seek professional help and hypothermia treatment.
Here is a great video by ABC news on how to do this.
Summary
Overall, the key take-home points for management of a fatal or non-fatal drowning patient in the emergency department includes the following:
- Management in the resuscitation bay:
- Anticipate a difficult and soiled airway, use a SALAD approach
- Employ ARDS ventilation settings
- Prompt OG or NG tube decompression
- Obtain a core temperature and initiate hypothermia rewarming early
- C-spine injuries are rare (0.5%), collar only if obvious signs and mechanism
- No antibiotics are indicated unless drowned in sewage
- Submersion duration is the only factor with reliable evidence for prognostication.
- Safely discharge the well appearing drowning patient home 6-hours post event if meets all three of:
- Normal mentation.
- Normal age adjusted vitals.
- Never required O2.
References
[1] J. J. L. M. Bierens, P. Lunetta, M. Tipton, and D. S. Warner, “Physiology Of Drowning: A Review,” Physiology, vol. 31, no. 2, pp. 147–166, Mar. 2016, doi: 10.1152/physiol.00002.2015.
[2] C. W. Root et al., “Suction Assisted Laryngoscopy and Airway Decontamination (SALAD): A technique for improved emergency airway management,” Resusc. Plus, vol. 1–2, p. 100005, Mar. 2020, doi: 10.1016/j.resplu.2020.100005.
[3] O. Thom, K. Roberts, S. Devine, P. A. Leggat, and R. C. Franklin, “Treatment of the lung injury of drowning: a systematic review,” Crit. Care, vol. 25, no. 1, p. 253, Dec. 2021, doi: 10.1186/s13054-021-03687-2.
[4] R. S. Watson, P. Cummings, L. Quan, S. Bratton, and N. S. Weiss, “Cervical Spine Injuries among Submersion Victims:,” J. Trauma Inj. Infect. Crit. Care, vol. 51, no. 4, pp. 658–662, Oct. 2001, doi: 10.1097/00005373-200110000-00006.
[5] P. Sramek, M. Simeckova, L. Jansky, J. Savllkova, and S. Vybiral, “Human physiological responses to immersion into water of different temperatures,” Eur. J. Appl. Physiol., vol. 81, no. 5, pp. 436–442, Feb. 2000, doi: 10.1007/s004210050065.
[6] R. M. Bennett, “Drowning and Near-Drowning Etiology and Pathophysiology,” Am. J. Nurs., vol. 76, no. 6, p. 919, Jun. 1976, doi: 10.2307/3423913.
[7] J. P. Orlowski and D. Szpilman, “DROWNING,” Pediatr. Clin. North Am., vol. 48, no. 3, pp. 627–646, Jun. 2001, doi: 10.1016/S0031-3955(05)70331-X.
[8] A. L. Anker, T. Santora, and W. Spivey, “Artificial Surfactant Administration in an Animal Model of Near Drowning,” Acad. Emerg. Med., vol. 2, no. 3, pp. 204–210, Mar. 1995, doi: 10.1111/j.1553-2712.1995.tb03200.x.
[9] D. Chandy and D. Richards, “Drowning (submersion injuries).” UpToDate, Feb. 2023. [Online]. Available: https://www.uptodate.com/contents/drowning-submersion-injuries
[10] “Drowning Consensus on Science with Treatment Recommendations [Internet] Brussels, Belgium: International Liaison Committee on Resuscitation (ILCOR) Advanced Life Support Task Force,” 2020, [Online]. Available: https://costr.ilcor.org/document/drowning-tfsr-costr
[11] D. Szpilman and P. J. Morgan, “Management for the Drowning Patient,” Chest, vol. 159, no. 4, pp. 1473–1483, Apr. 2021, doi: 10.1016/j.chest.2020.10.007.
[12] J. Bierens et al., “Resuscitation and emergency care in drowning: A scoping review,” Resuscitation, vol. 162, pp. 205–217, May 2021, doi: 10.1016/j.resuscitation.2021.01.033.
[13] J. D. McCall and B. T. Sternard, Drowning. StatPearls Publishing, Treasure Island (FL), 2022. [Online]. Available: http://europepmc.org/abstract/MED/28613583
[14] D. Szpilman, “Near-Drowning and Drowning Classification,” Chest, vol. 112, no. 3, pp. 660–665, Sep. 1997, doi: 10.1378/chest.112.3.660.
[15] G. G. Giesbrecht and G. K. McDonald, “My Car Is Sinking: Automobile Submersion, Lessons in Vehicle Escape,” Aviat. Space Environ. Med., vol. 81, no. 8, pp. 779–784, Aug. 2010, doi: 10.3357/ASEM.2769.2010.
[16] A. C. Schmidt, J. R. Sempsrott, S. C. Hawkins, A. S. Arastu, T. A. Cushing, and P. S. Auerbach, “Wilderness Medical Society Clinical Practice Guidelines for the Treatment and Prevention of Drowning: 2019 Update,” Wilderness Environ. Med., vol. 30, no. 4, pp. S70–S86, Dec. 2019, doi: 10.1016/j.wem.2019.06.007.


Trackbacks/Pingbacks