
As an emergency medicine physician, whether you are working in the resuscitation bay or in urgent care, ENT complaints are common and will be encountered in both areas. The goal of this post is to provide you with a practical framework and highlight tips and tricks for managing both common and life-threatening ENT emergencies.
By the end of this post, the goal is to walk away with a practical approach to the following complaints:
- Epistaxis
- Post-tonsillectomy bleeding
- Acute and chronic rhinosinusitis and their complications
- Peritonsillar abscesses
- Epiglottitis
Throughout the post, look for the following symbols:
- 🦪 – Clinical Pearl
- 📖 – Evidence Update
- 👩⚕️ – Expert Opinion
1. Epistaxis
Epistaxis is a common problem with most cases being uncomplicated, but some can present with severe or even life-threatening bleeding. Most cases seen in the ED will be anterior epistaxis with 90% of cases originating from Kiesselbach’s plexus.
The most common cause of epistaxis is minor mucosal trauma or irritation. Common predisposing factors for epistaxis that we should be screening for include:
- Dry/low humidity seasons
- Anticoagulation/anti-platelet medications
- Bleeding disorders
- Nasal cancers
- Liver disease/significant alcohol use
Although epistaxis is something we see all the time and likely know the basics of management, in talking to experts and reviewing recent evidence, there are some areas that we could improve upon. So let’s walk through an approach.
Sick or not sick?
- Once you have done a brief history and exam, our priority is to determine stability.
- If they are unstable, this is our wheelhouse! Resuscitate and address your
- If they are UNSTABLE:
- Address ABCs
- Blood transfusion for hemorrhagic shock
- Expedited standard epistaxis management (see below)
- Involve ENT earlier if unstable
- Consider:
- Anticoagulation reversal
- IV TXA
- Anti-emetics
- Remember that blood is emetogenic, so give this early to prevent a more soiled airway down the line!
For the stable patient, you will have more time to manage the epistaxis by following this step-by-step approach. Figure 1:
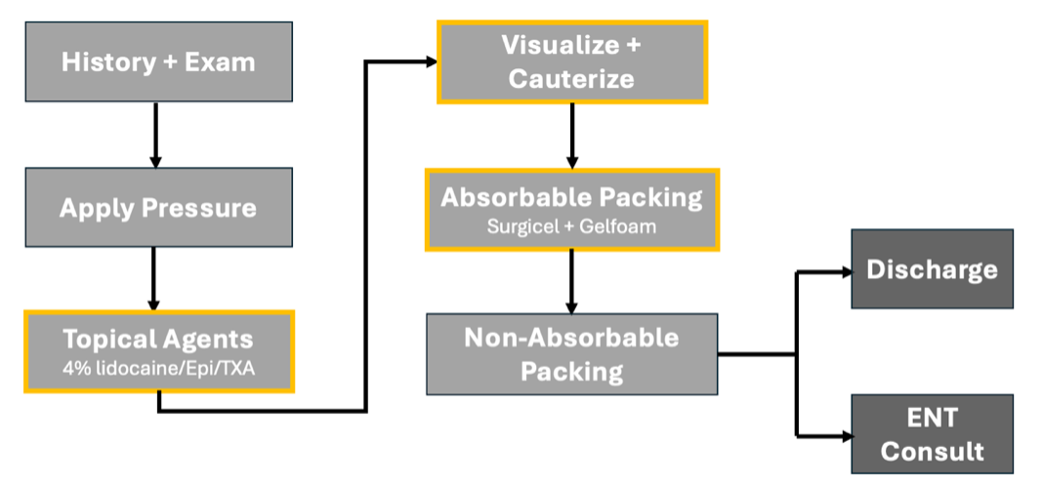
Step 1: Apply pressure
- Remember to always don your PPE with a face shield and gown.
- Ask the patient to blow out the clots and then apply pressure to the soft part of the nose, lean forward and keep holding consistent pressure and do NOT let go or they will have to start over.
🦪 Spray a nasal decongestant into the bleeding nose PRIOR to placing nasal clamp/applying pressure. Consider doing this at triage to optimize the chances of success without the need for packing down the line.
Step 2: Topical Agents
- Ask the patient to blow out the clots and try to visualize where the bleeding is coming from. If ongoing bleeding, it’s time to apply topical agents for decongestion and vasoconstriction to help with hemostasis.
- But what topical agents should you use?
📖

Accepting the limitations of some these positive studies, TXA has been shown to be a safe medication with some benefit. Seeing this through a patient centered lens, to avoid the discomfort of packing and potential need for repeat ED visits for packing removal, with a well-tolerated and safe medication, I would recommend adding TXA to your topical mix.
So here is what I propose as your ideal epistaxis topical solution:
TOPICAL AGENT MIX
- Epinephrine (1:1,000 or 1mg/mL) *
- 4% lidocaine
- TXA
- *Screen for cardiac history, if present use a decongestant like xylometazoline instead of epi
👩⚕️ In talking to our ENT colleagues, they find that epinephrine is the most effective vasoconstrictor in achieving hemostasis and what they typically reach for as first line. They use 1 in 1,000 or 1mg/mL epinephrine concentration. However, if your patient has a significant cardiac history, reach for xylometazoline or a decongestant as your vasoconstrictor of choice.
To prep for potential packing and need for cauterization, use 4% lidocaine. This higher concentration will allow for better analgesia and prevent over-dilution of your mixture. Finally, with the current evidence and good safety profile of TXA I would add TXA to that mix.Once you have made your mixture, make sure the patient blows out the clots and then prepare your cotton pledgets.
🦪 Stretch out your cotton pledget into a long cigar shape, dip them in your solution and insert them into the nose using your forceps like how you would insert packing. This will allow it to reach farther back in the nose
Apply your clamps and wait a minimum of 15 minutes. Don’t rush this step. These medications need time to work. Pick up another patient and return in 15-20 minutes.
Step 3: Visualize and Cauterize
- This step is probably an area where we could improve upon. Visualizing where the bleed is coming from key to help reassure you that it is not a posterior bleed and optimize your chances of successful cauterization.
- So, pause here and make sure these tips and tricks are in your epistaxis toolkit.
🦪
- Lighting is key
- Use the ENT head light or use your own head lamp if available
- Follow the bleed with the Frazier suction
- Use the nasal speculum to increase your area of visualization and follow the bleed back to its point of origin with the Frazier suction.
- Cauterize AROUND the bleed first
- Use silver nitrate to cauterize around the bleeding vessel, making your way slowly to the site of bleeding itself. Make sure you are using enough pressure for the silver nitrate to take effect – look for a slight bend in the silver nitrate stick.
Step 4: Absorbable packing
- If ongoing oozing/mild bleeding despite your attempts at visualization and cautery, consider absorbable packing. Although this may already be incorporated into some of our practices, I think it should become mainstay in our epistaxis algorithm.
- For absorbable packing, our ENT team typically uses a combination of gel foam and Surgicel.
- Practical Tip: Cut a piece of gelfoam to your desired size and wrap it in surgical, like a small cigar, and stick it to the area of bleeding.
- This is particularly helpful in the patients who are continually oozy rather than jumping to use non-absorbable packing.
- Although expensive, this technique offers several advantages including:
- Better patient comfort
- No need for repeat ED visit
- Avoids the chance of rebleeding with pack removal
Step 5: Non-absorbable packing
- You may be asking yourself when you get to this point – which non absorbable packing should I reach for: a balloon device like the Rapid Rhino or Epistat or a Merocel.
- And the answer is, it probably doesn’t make that big of a difference
📖 Rapid Rhino ≈ Merocel for rebleeding BUT Rapid Rhino better tolerated
A few quick practical Do’s and Don’ts of non-absorbable packing, specifically with Merocel insertion.
- DO’S
- Use oil-based lubricants
- Have your patient sit upright with their head against the back of the stretcher
- Push the tip of the patient’s nose upwards
- Follow the floor of the nose and try to aim medially
- This will allow you to follow the septum and avoid going directly into the turbinates which will cause discomfort and pain.
- Go FAST! This is uncomfortable and will be less tolerated if you go slowly.
- Irrigate the Merocel with a decongestant to provide further vasoconstriction
- DON’T’S
- Do NOT use water-based lubricants
- This will cause your Merocel to start inflating and will make it challenging to insert and advance far enough to stop the bleed.
- Do NOT use water-based lubricants
If you are still not able to get control with unilateral packing, I would proceed to bilateral anterior packing.
- 👩⚕️Consult ENT if:
- Uncontrolled or severe bleeding
Bleeding in ENT post-operative patients
Bilateral packing (center specific)
- Uncontrolled or severe bleeding
Step 6: Discharge
- For most patients, advise them to return for packing removal in 48hrs.
- If they are on anticoagulants, ENT typically leaves packing in for 72hrs.
- For patients on blood thinners, holding their anticoagulation will need to be done on a patient-by-patient basis, taking into account the severity of the bleed, the reason for anticoagulation, and the risks associated with holding it.
So what about antibiotics?
- The traditional teaching was that prophylactic antibiotics are necessary to prevent toxic shock syndrome. Although rare, there have case reports with anterior nasal packing and caries a risk of mortality even in healthy patients. However, as we know, antibiotics can have adverse effects themselves.
- Overall, the studies looking at this question are based on small retrospective, observation studies and there is a lack of convincing high-quality evidence to support the use of universal antibiotics for packing and few clinically significant infections were recorded.
- In the most recent 2020 Epistaxis Guidelines published by the American Academy of Otolaryngology and Head and Neck surgery, they state that given the lack of convincing evidence, the risks and benefits of antibiotic use should be evaluated on a patient by patient basis.
- In talking to ENT experts, their practice is to still give antibiotics to anyone with packing given this potential risk and often prescribe cephalexin while the packing remains in situ.
To distill this down, this is what I suggest:
- Screen for risk factors that may make someone more prone to have infectious complications (ex. immunocompromised, on chemotherapies, severe diabetes)
- If these exist, consider providing antibiotic prophylaxis.
- If no risk factors and the patient is otherwise healthy, engage in shared decision making with patient.
- I would generally opt to forgo antibiotics with clear instructions on what to watch for and the importance of returning for packing removal.
🦪 Finally, some pearls from our ENT colleagues that they recommend to their patients.
- Highlight the importance of home humidifiers to counteract the low moisture environment, especially in the winter months.
- Use nasal lubricants, which may include:
- Petroleum jelly (ex. Vaseline) – Use a small dallop on their finger, place just inside their nose to warm it up and gently sniff in to apply lubrication to the rest of the nose
- Nasal spray lubricants: Water based lubricants (ex. Secaris) or Oil base lubricant (ex. Nozoil – a sesame oil based product).
Key Take Home Points
- “Ideal” topical solution = 4% lidocaine + epi/xylometazoline + TXA
- Visualization and Frazier suction is KEY
- Add absorbable packing to your practice
- No need for return visits
- Better patient comfort
2. Post-Tonsillectomy Bleeds
Tonsillectomies are common operations in both children and adults with the vast majority having uncomplicated courses. Post-tonsillectomy bleeds are categorized into 2 main groups based on the timing of their presentation:
- Primary: <24hrs post-op
- Typically related to intra-operative factors/surgical techniques and underlying coagulopathies.
- Secondary: >24hrs post-op (Usually 5-7 days, up to 14 days)
- Thought to be due to the sloughing of the tonsillar bed eschar as it naturally separates from the underlying tissue resulting in the exposure of small surface vessels that are prone to bleeding after minor local trauma.
- These can present with minor oozing but can be insidious and escalate quickly.
Minor bleeding is a common complication post-operatively and although major bleeding only occurs in about 3-5% of patients it can be severe and life threatening. Mortality is quoted to be 1 per 56,000 cases in Ontario, with 1/3 of deaths related to bleeding.
Even when a patient presents with a minor bleed, it is not uncommon to have multiple episodes of bleeding with 30% of cases having a second bleeding event.
🦪Minor bleeding is often a warning sign of severe life-threatening hemorrhage
So let’s review the common presentations so that if you were to be faced with a catastrophic bleed you are equipped with the tools to save their life. Management can be practically divided into 3 main concepts:
- Direct pressure and application of topical therapies.
- Nebulized medications
- Close monitoring and call for help early
In talking to ENT specialists, in addition to our typical resuscitative measures, for your severe bleeds the thing we can do while we wait for ENT for operative management is to apply direct pressure with epi-soaked gauze. This is the management step that they highlight is the best initial step we can do in the ED that can save the patient’s life.
They use 1:1,000 epinephrine-soaked gauze and Magill or ringed forceps to apply direct pressure to the bleeding tonsillar bed. Apply pressure laterally to help with hemostasis.
- If time permits, spray first with topical lidocaine and if the patient is cooperative sometimes you can allow them to apply pressure themselves.
🦪 Direct pressure + Epi-soaked gauze = LIFE SAVING
There is limited evidence assessing IV TXA for post-tonsillectomy hemorrhage, however, extrapolating data from prior studies for acute bleeds, we know that TXA has been shown to be more efficacious when given early. Using this and in talking to experts, for severe bleeding, I would give a dose of TXA as long as there are no contra-indications.
In terms of nebulized medications, they offer a potential non-invasive treatment option, which can be particularly useful in pediatric patients when accessing the oropharynx can be a challenge.
A Systematic review and meta-analysis by Alghamdi et al assessed the rate of repeat OR to control bleeding in patients who received nebulized TXA vs no TXA. They found that there were significantly lower rates of repeat OR required in the TXA arm and concluded that nebulized TXA was a safe and a promising treatment for post-tonsillectomy bleeds
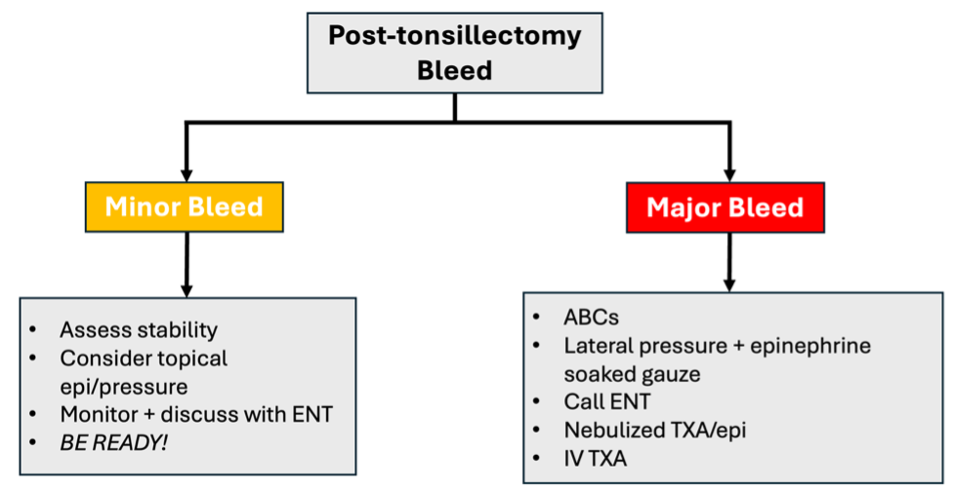
Summary
Minor Bleeds:
- If ongoing bleeding, consider topical epinephrine and direct pressure
- Given the risk of a subsequent bleeds, it is important to monitor these patients. Call ENT to discuss the need for monitoring and disposition planning.
- While monitoring, be prepared to intervene if a secondary bleed occurs.
Major Bleeds:
- Address your ABCs, grab your epi-soaked gauze, give a dose of IV TXA and call for help.
- If the patient is uncooperative or you are unable to access the posterior oropharynx consider using nebulized TXA or epinephrine to temporize.
Acute and Chronic Rhinosinusitis
Rhinosinusitis refers to the symptomatic inflammation of the paranasal sinuses and nasal cavity. It can be categorized into acute (symptoms <4 weeks) and chronic (symptoms >12 weeks). Acute rhinosinusitis (ARS) is something that we will see frequently in the ED. Risk factors to develop ARS include older age, smoking, changes in atmospheric pressure like flying or scuba diving, swimming, allergies, or immunodeficiency.
ARS Causes:
- Viral
- Most cases we see are due to a viral illness presenting with similar symptoms to a viral URTI with a peak in severity around days 3-6 and partial or complete resolution by day 7-10 with conservative management.
- Bacterial
- Only ~0.5-2% of cases will be bacterial
- Most common bacteria: Strep pneumonia, Haemophilus influenzae and Moraxella catarrhalis.
- Allergic
- Non-allergic
- Mechanical obstruction
- Impaired mucociliary clearance (ex. CF)
For ARS, we will focus mainly on the management and diagnosis of acute bacterial rhinosinusitis (ABRS). We should think about ABRS when symptoms are present for 7-10 days or more without evidence of improvement with a typical biphasic or double worsening pattern after initial viral symptoms. ABRS is a clinical diagnosis, and imaging should not be obtained unless there is a clinical concern for complications.
Diagnosis of ABRS:
- 2 “PODS” symptoms, 1 of which must be O or D.
“PODS”
- P = facial pain/pressure/fullness
- O = nasal obstruction
- D = purulent nasal discharge
- S = smell – hyposmia or anosmia
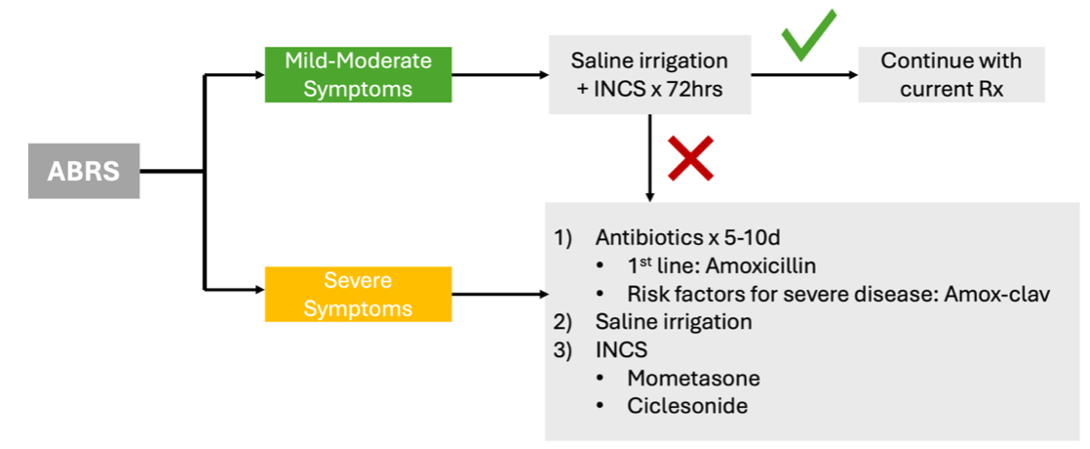
Management of ABRS:
- Many patients will have a self-limited disease that resolves with time and rarely develop complications even without antibiotics.
- In the 2018 Cochrane review on antibiotics for acute rhinosinusitis (https://pubmed.ncbi.nlm.nih.gov/30198548/), they found that the NNT for an additional beneficial outcome was 19 and the NNT for an additional harmful outcome was 8. They concluded that the potential benefit of antibiotics was marginal, and we need to consider their use in the context of risks associated with antibiotics and patient factors.
Because of the challenges with follow up in the ED, what I would recommend is engaging in shared decision making with the patient based on their co-morbidities and severity of symptoms. If mild symptoms, use a watch and wait approach with a delayed start of antibiotics after 72hrs of conservative management with saline irrigation and intra-nasal corticosteroids. If severe symptoms on presentation or if conservative management fails after 72hrs, proceed with antibiotic treatment (Figure 3).
ABRS+ CRS Complications:
Although most cases will be uncomplicated, it is our job to screen for any complications in the ED. You should have a high suspicion for a complication in a patient who is presenting with high persistent fever despite treatment, persistent severe headache or signs of any of these concerning disease processes.
- Orbital Cellulitis
- One of the most common complications
- Screen for: Vision changes, pain with extra-ocular movements, proptosis
- If suspected, obtain a CT scan to assess for subperiosteal abscess
- CNS complications:
- These can include meningitis, osteomyelitis with underlying subperiosteal abscess (Pott’s puffy tumour), and intracranial abscesses.
- Screen for: Severe headache, altered mental status, findings of raised ICP
- Septic cavernous sinus thrombosis
- Screen for:
- Cranial nerve palsies (specifically CN3, 4 and 6 and the ophthalmic and maxillary division of the trigeminal nerve)
- Headache, diplopia, periorbital edema, fever.
- Screen for:
Chronic Rhinosinusitis:
Although this is often a presentation commonly see in primary care, given the current state of our healthcare system, we can likely expect to see more of these in the ED. My hope is to provide you with some quick tips and tricks for identifying chronic rhinosinusitis and empower you to initiate treatment on their initial visit.
CRS Diagnosis:
- >12 weeks of symptoms
- 2 “CPODS” symptoms + signs of inflammation
- C = congestion
- P = facial pain/pressure/fullness
- O = nasal obstruction
- D = purulent anterior/posterior drainage
- S = smell – hyposmia or anosmia
- Subtypes
- With nasal polyps (CRSwNP)
- Without nasal polyps (CRSsNP)
CRS without nasal polyps makes up the majority of cases (60-65%) and presents more commonly with facial pain/pressure while CRS with nasal polyps have predominant hyposmia. Management depends on the subtype, so it is important to try and do a nasal exam on these patients.
CRS can largely be diagnosed and started on treatments based on clinical exam and history alone. In talking to our local ENT experts, in the absence of suspected complications, a CT is not indicated. CTs are generally used for surgical planning and can be ordered once surgery is being considered.
CRS Management:
In discussion with our ENT colleagues, we propose the following management:
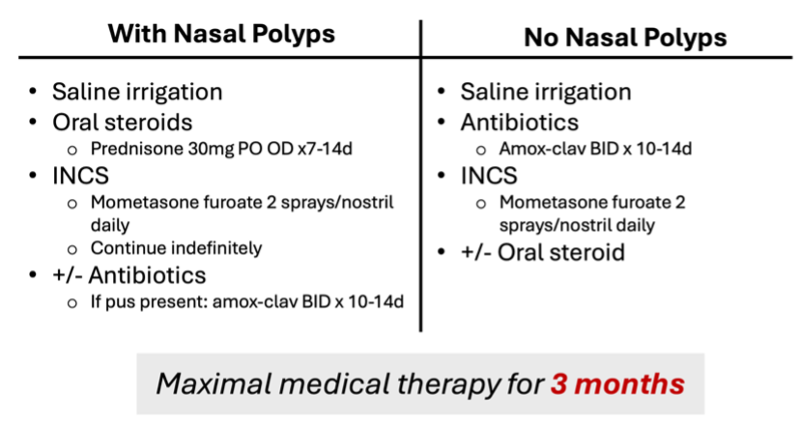
Note: For CRS without nasal polyps, oral steroids are not necessary or routinely recommended as first line but could be considered if there is significant inflammation.
It is important to remember that this is a chronic disease. These patients need to be on maximal medical therapy for 3 months prior to consideration of surgery or other treatment modalities. If a patient has failed 3 months of maximal medical therapy, this is the point where an ENT specialist would assess them to determine the next steps.
- 🦪 For ABRS – use a “watch and wait” approach for antibiotics prescriptions for mild-moderate symptoms
- For CRS:
- Examine for nasal polyps
- Initiate maximal medical therapy in the ED
- Set expectations + importance of compliance – need 3 months of treatment prior to specialist/surgical assessment and improvement is slow and gradual
Peritonsillar Abscess (PTA)
- PTAs are most frequently seen in adolescents and young adults and are typically polymicrobial with Group A strep, staph and respiratory anaerobes as common infectious culprits.
- Differentiating peritonsillar cellulitis and PTAs can be challenging on physical exam and is likely one of the main reasons for diagnostic uncertainty.
- Peritonsillar cellulitis or a phlegmon = inflammatory reaction of the peritonsillar space, but without a discrete pus collection.
- Why do we care?
- If left untreated, PTAs can result in complications including retropharyngeal abscesses, Lemierre’s, descending mediastinitis and even airway obstruction.
- Early diagnosis and management are critical in preventing these complications
PTA Overview:
- Most commonly occur in the superior pole of the tonsil, followed by the mid and inferior poles.
- Classic symptoms:
- Severe sore throat (often one-sided)
- Fever
- Voice changes
- Referred otalgia
- Drooling
- Physical Exam Findings:
- Unilateral peritonsillar and soft palate swelling
- Bilateral PTAs are rare, but not impossible
- Uvular deviation
- Cervical adenopathy.
- Trismus
- 2/3 of patients with PTAs develop trismus due to the irritation and spasm and of the internal pterygoid muscle. This can sometimes help you differentiate a PTA from pharyngitis.
- 2/3 of patients with PTAs develop trismus due to the irritation and spasm and of the internal pterygoid muscle. This can sometimes help you differentiate a PTA from pharyngitis.
- Unilateral peritonsillar and soft palate swelling
- 🦪 Assess neck range of motion
- Should be NORMAL in an uncomplicated PTA.
- If decreased, have a high suspicion for deep neck space, particularly if restricted with neck EXTENSION
- In patients with retropharyngeal abscesses, there is typically pain and limitation with neck extension (compared to flexion classically with meningitis)
PTA Diagnosis:
- So how good are we at diagnosing PTAs in the emergency department?
- Physical exam alone: Sensitivity 75-78%, Specificity 50%
- CT: Sensitivity ~100%
- Cons: Radiation exposure, increased ED length of stay, $$$
- Needle aspiration: False negative rate ~10-24%
To increase our confidence in diagnosing PTAs in the ED, consider using ultrasound as your 1st line diagnostic modality.
Advantages of US:
- Accessible + Fast
- No radiation
- Guide management
- Determine PTA size
- Assist in landmarking for drainage
- Improves ED LOS
There are 2 main US approaches:
- Intra-oral approach using the endocavitary probe
- Sensitivity: 90-100%
- Remember to topicalize the posterior oropharynx prior to US
- Advantages:
- Better orientation and landmarking for needle aspiration/I&D
- Allow for measurement of depth of internal carotid
- Cons: Limited by patient comfort and level of trismus
- Transcutaneous/transcervical approach using the linear probe
- Sensitivity: 80-91%
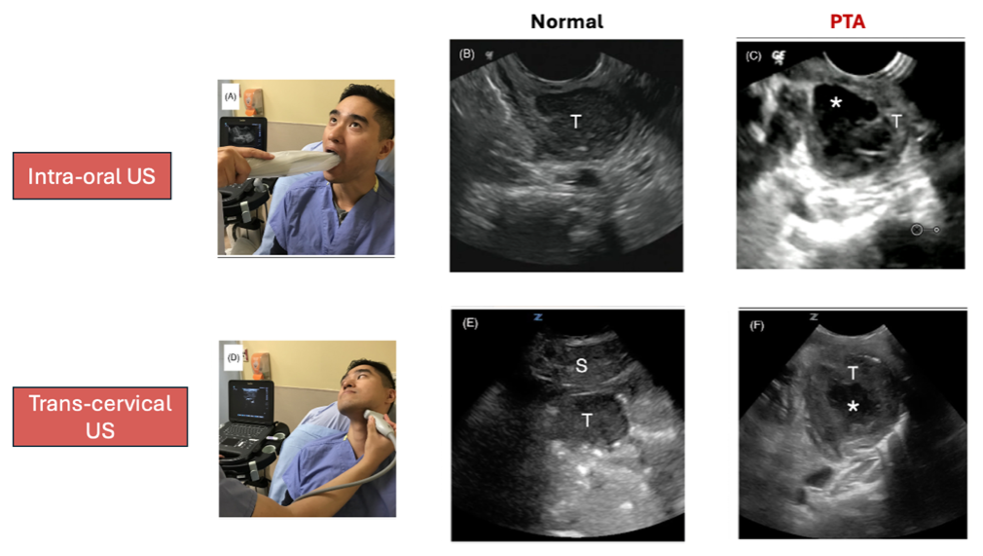
Image source: https://caep.ca/wp-content/uploads/2025/04/Academic-Emergency-Medicine-2023-Kim-Test-characteristics-of-ultrasound-for-the-diagnosis-of-peritonsillar-abscess-A.pdf
PTA Management:
Medical Management:
- IV fluids if dehydrated
- Analgesia (IV Ketorolac)
- Antibiotics:
- Choice of antibiotics depends on a few factors including severity of illness and whether they can tolerate PO
- Examples of IV options: Amox-clav or ampicillin, penicillin/ceftriaxone + metronidazole, clindamycin
- Steroids (Dexamethasone 10mg IV)
Surgical Management:
- After doing a PoCUS, if the abscess is small and <1cm in a patient who has not yet been started on antibiotics, you can do shared decision making regarding the need for PTA drainage.
- If you are opting for medical management alone in these select cases, follow up and re-evaluation are critical.
- In a patient with a large abscess or someone who has already failed outpatient antibiotics, we should proceed with draining the PTA.
- Even with surgical management, the recurrence rate of PTAs has been quoted up to 10-15%.
Needle aspiration vs. I&D?
- In 2016, Chang et al published a Cochrane review assessing needle aspiration vs. I&D for PTAs (https://pubmed.ncbi.nlm.nih.gov/28009937/). They concluded that there is no high-quality evidence to allow for a firm conclusion to be drawn. However, very low-quality evidence suggests that I&D may be associated with a lower chance of recurrence, but needle aspiration is generally less painful.
- Our ENT colleagues here typically start with needle aspiration and will transition to I&D if significant pus is obtained.
- This is a reasonable strategy for us to use in the ED as it allows you to locate the abscess pocket and ensure you are incising the correct area. However, this largely depends on your own comfort with the procedure and the size of the abscess.
👩⚕️ In talking to our ENT colleagues, they find that epinephrine is the most effective vasoconstrictor in achieving hemostasis and what they typically reach for as first line. They use 1 in 1,000 or 1mg/mL epinephrine concentration. However, if your patient has a significant cardiac history, reach for xylometazoline or a decongestant as your vasoconstrictor of choice.
Tips and Tricks:
See links below for a step by step video on how to drain a PTA:
https://coreem.net/procedures/drainage-of-a-peritonsillar-abscess/
https://www.emrap.org/hd/playlist/entPL/chapter/ptaneedle/ptaneedle
To highlight a few tips and tricks to optimize your chances of a successful drainage:
- Find the peritonsillar space
- Once anesthetized you can palpate the tonsil for the area of maximal fluctuance or use the suction to identify the margin of the tonsil
- Use caution/avoid if uncooperative patient or severe trismus
- 1st attempt = superior pole
- Start at the superior pole and avoid the inferior pole given the highest risk and proximity to the carotid artery
- Visualization
- Use a headlamp
- For additional light and to create space in the oropharynx consider using:
- Laryngoscope blade with light on
- Disposable vaginal speculum with light (remove the top piece and use the bottom piece with the light)
- Safety precautions
- Use PoCUS to determine the depth of the carotid
- Cut off the needle cap or cover the distal end of the scalpel blade so that only 1cm is exposed to prevent any accidental damage to deeper structures (see pictures below)

Epiglottitis
Epiglottitis is taught as a primarily pediatric presentation commonly associated with Haemophilus influenza type B. We classically think of it in the unvaccinated pediatric patient, ages 2-6, who presents with fever, stridor, drooling, respiratory distress, and tripoding. Anatomically, given the natural narrow pediatric airways, even minimal obstruction due to epiglottic inflammation can cause acute airway obstruction and severe illness.
Following the implementation of the haemophlius influenza type B vaccine, the presentations and epidemiology of epiglottitis has shifted. In the post-vaccine era, the incidence of pediatric epiglottitis has significantly decreased, with epiglottitis now being a predominantly adult disease.
There has also been a shift in the causative organisms, with most cases being polymicrobial. Predominant organisms now tend to be streptococcus and staph species, and some cases of haemophilus. In your immunocompromised patients, you should think of potential fungal and gram-negative organisms and screen for MRSA risk factors.
Although the focus of rest of our discussion about epiglottitis will be around infectious causes, it is important to recognize that non-infectious causes do exist.
Non-Infectious Causes:
- Radiation
- Trauma
- Foreign body ingestion
- Thermal/caustic injury
- Auto-immune
Although they can present with symptoms of acute airway obstruction, adults rarely present with the classic features we see in pediatrics but rather a more progressive and subacute onset of symptoms.
Common Symptoms in Adults:
- Progressively sore throat with predominant odynophagia and dysphagia
- Voice changes/pain with talking
- Drooling
Stridor and respiratory distress occur in a minority of presentations, but if present, are associated with the need for airway management. Particularly if these patients present with a rapid onset of symptoms, it is an ominous sign and you should have a higher concern for severe disease.
- 🦪 Physical Exam PEARLS:
- Normal oropharynx or pain out of proportion to exam
- 90% of adult epiglottitis will have a NORMAL oropharynx exam
- Pain to palpation of the larynx/hyoid
- Normal oropharynx or pain out of proportion to exam
Given that epiglottitis is a low prevalence disease associated with potential high morbidity and even mortality, with minimal historical and examination findings to go off of, it can pose a diagnostic dilemma and result in delays to diagnosis. If you don’t think about it, you will miss it.
Diagnostic Modalities:
- Lateral neck x-rays (Ex. Thumb sign, loss of vallecula, epiglottis width)
- Pros:
- Portable/don’t need to move patient to unmonitored area
- Patient can remain sitting upright
- Cons:
- Poor sensitivity and specificity
- High false negative rate (some studies quote up to ~32%)
- Conclusion: Can be a useful data point if positive, but should not be used to rule out epiglottitis with high clinical suspicion
- Pros:
- CT:
- Pros:
- Higher sensitivity (88-100%) + specificity (96%)
- Can help assess for alternative diagnoses
- Cons:
- High risk transportation/out of monitored area
- Lying down can precipitate airway obstruction
- Conclusion: CT should not be used in patients with high-risk features and airway concerns prior to establishment of a definitive airway
- Pros:
- Nasopharyngeal scope
- Pros:
- Direct visualization of epiglottitis
- Can help determine severity of swelling
- Cons:
- Can worsen respiratory distress/obstruction if patient begins to panic/hyperventilate
- ENT often avoids tropicalizing for NP scope given concerns that topicalization can give sense of worsening airway obstruction
- Conclusion: ONLY perform if the patient is stable with no respiratory complaints or stridor. Do NOT perform in anyone with stridor or respiratory distress given potential worsening after scope. When in doubt, call ENT.
- Pros:
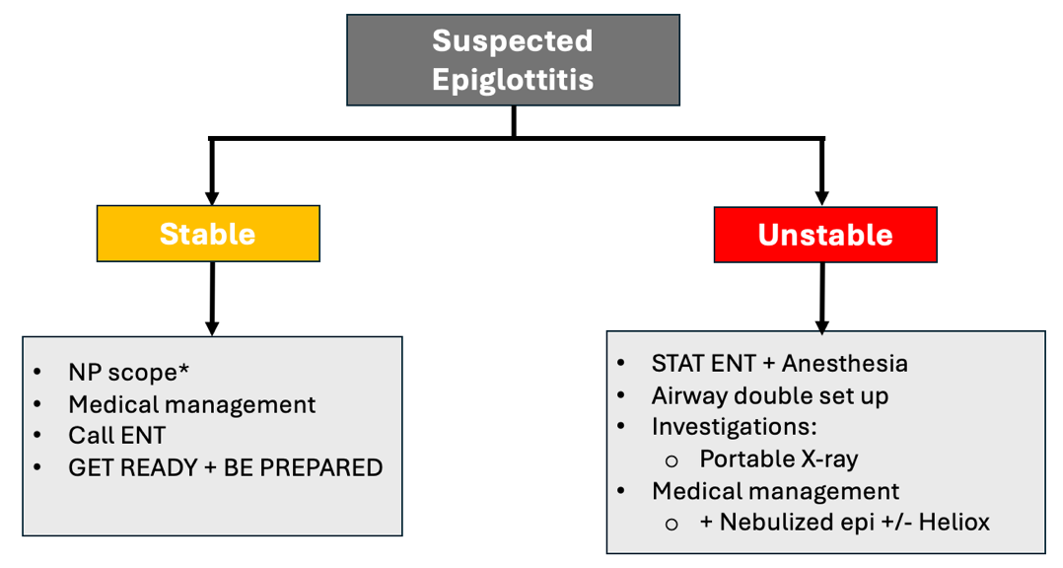
Epiglottitis Management (Figure 4):
- Step 1: Stable or unstable?
- Recognize that all these patients have the risk to deteriorate
- In this algorithm, “stable” refers to the patient with no stridor or respiratory symptoms and looks well. These are the cases you could consider doing an NP scope if comfortable. However, given the potential dynamic process, perform this in a monitored area and be prepared.
- If unstable: Priority = airway management
- Our goal is to get them quickly and safely to the OR for airway intervention with ENT and anesthesia
- Call for help early and be prepared. Have your double set up and surgical airway equipment ready!
- General Medical Management:
- Supportive therapy (IV fluids, analgesia) + elevate head of the bed
- IV antibiotics (Ceftriaxone 2g IV)
- +/- Vanco if MRSA risk factors/severe sepsis
- If immunocompromised, consider covering for gram-negatives and pseudomonas (ex. Pip-tazo or cefipime)
- IV steroids (ex. Dexamethasone 10mg IV)
- Controversial with minimal high-quality evidence to support or refute its use. However, given acute nature and theoretical benefit of reducing airway edema, our ENT colleagues do recommend giving a dose
- Add-Ons for the unstable patients:
- Initiate the above medical management
- Consider lateral neck xray if patient/time permits
- Start nebulized epinephrine and heliox
- This may buy you some time until ENT arrives
- Take Home: BE PREPARED
- These can deteriorate quickly, even if they arrive looking stable.
- Call for help early and have your double set up ready
References
1. Akkan, S., Çorbacıoğlu, S. K., Aytar, H., Emektar, E., Dağar, S., & Çevik, Y. (2019). Evaluating effectiveness of nasal compression with tranexamic acid compared with simple nasal compression and Merocel packing: A randomized controlled trial. Annals of Emergency Medicine, 74(1), 72-78.
2. Alghamdi, A. S., Hazzazi, G. S., Shaheen, M. H., Bosaeed, K. M., Kutubkhana, R. H., Alharbi, R. A., Abu-Zaid, A., & Felemban, R. A. (2024). Nebulized tranexamic acid for treatment of post-tonsillectomy bleeding: A systematic review and meta-analysis. European Archives of Oto-Rhino-Laryngology.
3. Battaglia, A., Burchette, R., Hussman, J., Silver, M. A., Martin, P., & Bernstein, P. (2018). Comparison of medical therapy alone to medical therapy with surgical treatment of peritonsillar abscess. Otolaryngology–Head and Neck Surgery, 158(2), 280-286.
4. Baugh, R. F., Archer, S. M., Mitchell, R. B., Rosenfeld, R. M., Amin, R., Burns, J. J., Darrow, D. H., Giordano, T., Litman, R. S., Li, K. K., Mannix, M. E., Schwartz, R. H., Setzen, G., Wald, E. R., Wall, E., Sandberg, G., & Patel, M. M. (2011). Clinical practice guideline: Tonsillectomy in children. Otolaryngology–Head and Neck Surgery, 144(1S), S1–S30.
5. Berger, G., Landau, T., Berger, S., Finkelstein, Y., Bernheim, J., & Ophir, D. (2003). The rising incidence of adult acute epiglottitis and epiglottic abscess. American Journal of Otolaryngology, 24(6), 374–383.
6. Bridwell, R. E., Koyfman, A., & Long, B. (2022). High risk and low prevalence diseases: Adult epiglottitis. American Journal of Emergency Medicine, 57, 14–20.
7. Bryczkowski, C., Haussner, W., Rometti, M., Wei, G., Morrison, D., Geria, R., & McCoy, J. V. (2022). Impact of bedside ultrasound on emergency department length of stay and admission in patients with a suspected peritonsillar abscess. Cureus, 14(12), e32207.
8. Butler, F. M., & Hernandez, D. R. (2025). Acute rhinosinusitis: Rapid evidence review. American Family Physician, 111(1), 47–53.
9. Chan, D. K., & Parikh, S. R. (2014). Perioperative ketorolac increases post-tonsillectomy hemorrhage in adults but not children. The Laryngoscope, 124(8), 1789–1793.
10. Chang, B. A., Thamboo, A., Burton, M. J., Diamond, C., & Nunez, D. A. (2016). Needle aspiration versus incision and drainage for the treatment of peritonsillar abscess. Cochrane Database of Systematic Reviews, 2016(12)..
11. Chau, J. K. M., Seikaly, H. R., Harris, J. R., Villa-Roel, C., Brick, C., & Rowe, B. H. (2013). Corticosteroids in peritonsillar abscess treatment: A blinded placebo-controlled clinical trial. The Laryngoscope, 124(1), 97-103.
12. Chiang, C. Y., Lin, J. S., Tsai, T. Y., Tu, Y. K., & Tsai, M. J. (2023). Comparative effectiveness of various noninvasive local treatments in patients with epistaxis: A systematic review and network meta-analysis. Academic Emergency Medicine, 30(10), 1047–1058.
13. Chiang, C. Y., Lin, J. S., Tsai, T. Y., Tu, Y. K., & Tsai, M. J. (2023). Comparative effectiveness of various noninvasive local treatments in patients with epistaxis: A systematic review and network meta-analysis. Academic Emergency Medicine, 30(10), 1047–1058. https://doi.org/10.1111/acem.14680​:contentReference[oaicite:2]{index=2}
14. Chow, A. W., Benninger, M. S., Brook, I., Brozek, J. L., Goldstein, E. J. C., Hicks, L. A., Pankey, G. A., Seleznick, M., Volturo, G., Wald, E. R., & File, T. M. (2012). IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clinical Infectious Diseases, 54(8), e72–e112.
15. Cohn, B. (2015). Are prophylactic antibiotics necessary for anterior nasal packing in epistaxis? Annals of Emergency Medicine, 65(1), 109-111.
16. de Cassan, S., Thompson, M. J., Perera, R., Glasziou, P. P., Del Mar, C. B., Heneghan, C. J., & Hayward, G. (2020). Corticosteroids as standalone or add-on treatment for sore throat. Cochrane Database of Systematic Reviews, 2020(5)
17. Desrosiers, M., Evans, G. A., Keith, P. K., Wright, E. D., Kaplan, A., Bouchard, J., Ciavarella, A., Doyle, P. W., Javer, A. R., Leith, E. S., Mukherji, A., Schellenberg, R. R., Small, P., & Witterick, I. J. (2011). Canadian clinical practice guidelines for acute and chronic rhinosinusitis. Allergy, Asthma & Clinical Immunology, 7(2).
18. Epstein, V. A., & Kern, R. C. (2008). Invasive fungal sinusitis and complications of rhinosinusitis. Otolaryngologic Clinics of North America, 41(3), 497–524.
19. Fan, Z., Qiao, T., Shi, S., Zhang, A., Liu, J., Wang, Y., & Liu, C. (2025). Epidemiology, presentation, management, and outcomes of patients with acute epiglottitis: A 10-year retrospective study based on a tertiary hospital in northern China. European Archives of Oto-Rhino-Laryngology, 282(333–340).
20. Fokkens, W. J., Lund, V. J., Hopkins, C., Hellings, P. W., Kern, R., Reitsma, S., … & Wang, D. Y. (2020). European position paper on rhinosinusitis and nasal polyps 2020. Rhinology, 29(Supplement), 1–464.
21. Fokkens, W. J., Lund, V. J., Mullol, J., Bachert, C., Alobid, I., Baroody, F., Cohen, N., Cervin, A., Douglas, R., Gevaert, P., Georgalas, C., Goossens, H., Harvey, R., Hellings, P., Hopkins, C., Jones, N., Joos, G., Kalogjera, L., Kern, B., … Wormald, P. J. (2012). European position paper on rhinosinusitis and nasal polyps 2012. Rhinology, 50(1), 1–12.
22. Forner, D., Curry, D. E., Hancock, K., MacKay, C., Taylor, S. M., Corsten, M., Trites, J. R., & Rigby, M. H. (2020). Medical intervention alone vs surgical drainage for treatment of peritonsillar abscess: A systematic review and meta-analysis. Otolaryngology–Head and Neck Surgery, 163(5), 915-922.
23. Fujiwara, T., Miyata, T., Tokumasu, H., Gemba, H., & Fukuoka, T. (2017). Diagnostic accuracy of radiographs for detecting supraglottitis: A systematic review and meta‐analysis. Acute Medicine & Surgery, 4(3), 190–197.
24. Furukawa, M., Hashimoto, K., Kitani, Y., & Yoshida, M. (2022). Point-of-care ultrasound in the head and neck region. Journal of Medical Ultrasonics, 49(4), 593–600.
25. Galioto, N. J. (2017). Peritonsillar abscess. American Family Physician, 95(8), 501-506.
26. Gifford, T. O., & Orlandi, R. R. (2008). Epistaxis. Otolaryngologic Clinics of North America, 41(3), 525–536.
27. Glynn, F., & Fenton, J. E. (2008). Diagnosis and management of supraglottitis (epiglottitis). Current Infectious Disease Reports, 10(3), 200–204.
28. Gottlieb, M., & Long, B. (2023). Managing epistaxis. Annals of Emergency Medicine, 81(2), 234-240.
29. Gottlieb, M., Long, B., & Koyfman, A. (2018). Clinical mimics: An emergency medicine-focused review of streptococcal pharyngitis mimics. The Journal of Emergency Medicine, 54(5), 619-629.
30. Guardiani, E., Bliss, M., & Harley, E. (2010). Supraglottitis in the era following widespread immunization against Haemophilus influenzae type B: Evolving principles in diagnosis and management. The Laryngoscope, 120(11), 2183–2188.
31. Hanna, J., Brauer, P. R., Berson, E., & Mehra, S. (2019). Adult epiglottitis: Trends and predictors of mortality in over 30 thousand cases from 2007 to 2014. The Laryngoscope, 129(5), 1107–1112.
32. Hardman, J. C., & Nankivell, P. (2014). Do corticosteroids improve outcomes in peritonsillar abscess? The Laryngoscope, 124(9), 1945-1950.
33. Harounian, J. A., Schaefer, E., Schubart, J., & Carr, M. M. (2016). Pediatric adenotonsillectomy and postoperative hemorrhage: Demographic and geographic variation in the US. International Journal of Pediatric Otorhinolaryngology, 87, 50–54.
34. Hori, H., Fukuchi, T., & Sugawara, H. (2021). Point-of-care ultrasound for prompt diagnosis and treatment monitoring of acute epiglottitis. Journal of General and Family Medicine, 22(1), 51–52.
35. Hosseini, M., Jahangiri, R., Faramarzi, A., Asmarian, N., Sajedianfard, S., Kherad, M., Soltaniesmaeili, A., & Babaei, A. (2022). Intranasal topical application of tranexamic acid in atraumatic anterior epistaxis: A double-blind randomized clinical trial. Annals of Emergency Medicine, 80(3), 182-188.
36. Hu, L., Gordon, S. A., Swaminathan, A., Wu, T., Lebowitz, R., & Lieberman, S. (2021). Utilization of prophylactic antibiotics after nasal packing for epistaxis. The Journal of Emergency Medicine, 60(2), 144–149.
37. Hur, K., Zhou, S., & Kysh, L. (2017). Adjunct steroids in the treatment of peritonsillar abscess: A systematic review. The Laryngoscope, 128(1), 72-77.
38. Iqbal, I. Z., Jones, G. H., Dawe, N., Mamais, C., Smith, M. E., Williams, R. J., Kuhn, I., & Carrie, S. (2017). Intranasal packs and haemostatic agents for the management of adult epistaxis: Systematic review. The Journal of Laryngology & Otology, 131(12), 1065–1092.
39. Iqbal, I. Z., Jones, G. H., Dawe, N., Mamais, C., Smith, M. E., Williams, R. J., Kuhn, I., & Carrie, S. (2017). Intranasal packs and haemostatic agents for the management of adult epistaxis: Systematic review. The Journal of Laryngology & Otology, 131(12), 1065–1092.
40. Janapala, R. N., Tran, Q. K., Patel, J., Mehta, E., & Pourmand, A. (2022). Efficacy of topical tranexamic acid in epistaxis: A systematic review and meta-analysis. American Journal of Emergency Medicine, 51, 169-175.
41. Joseph, J., Martinez-Devesa, P., Bellorini, J., & Burton, M. J. (2018). Tranexamic acid for patients with nasal haemorrhage (epistaxis). Cochrane Database of Systematic Reviews, 2018(12), CD004328.
42. Kaplan, A. (2014). Canadian guidelines for acute bacterial rhinosinusitis: Clinical summary. Canadian Family Physician, 60, 227–232.
43. Keating, M. K., Phillips, J. C., & Phillips, J. (2023). Chronic rhinosinusitis. American Family Physician, 108(4), 370–377. Retrieved from
44. Kim, D. J., Burton, J. E., Hammad, A., Sabhaney, V., Freder, J., Bone, J. N., & Ahn, J. S. (2023). Test characteristics of ultrasound for the diagnosis of peritonsillar abscess: A systematic review and meta-analysis. Academic Emergency Medicine, 30(10), 859–869.
45. Kimura, Y., Jo, T., Inoue, N., Suzukawa, M., Tanaka, G., Kage, H., Kumazawa, R., Matsui, H., Fushimi, K., Yasunaga, H., & Matsui, H. (2023). Association between systemic corticosteroid use and mortality in patients with epiglottitis. The Laryngoscope, 133(2), 344–349.
46. Ko, D. R., Chung, Y. E., Park, I., Lee, H.-J., Park, J. W., You, J. S., Chung, T. N., Park, Y. S., Chung, S. P., & Kim, S. (2012). Use of bedside sonography for diagnosing acute epiglottitis in the emergency department. Journal of Ultrasound in Medicine, 31(1), 19–22.
47. Kohen, B., Perez, M., McKay, J., Zamora, R., & Xu, C. (2023). The use of point-of-care ultrasound in the diagnosis of peritonsillar abscess. POCUS Journal, 8(2), 116-120.
48. Kuan, E. C., Tajudeen, B. A., Bhandarkar, N. D., St. John, M. A., Palmer, J. N., & Adappa, N. D. (2018). Is topical epinephrine safe for hemostasis in endoscopic sinus surgery? The Laryngoscope, 128(11), 2484–2491.
49. Lange, J. L., Peeden, E. H., & Stringer, S. P. (2017). Are prophylactic systemic antibiotics necessary with nasal packing? A systematic review. American Journal of Rhinology & Allergy, 31(4), 240-247.
50. Lee, S. H., Yun, S. J., Kim, D. H., Jo, H. H., & Ryu, S. (2017). Do we need a change in ED diagnostic strategy for adult acute epiglottitis? American Journal of Emergency Medicine, 35(10), 1519–1524.
51. Lee, Y. J., Jeong, Y. M., Lee, H. S., & Hwang, S. H. (2016). The efficacy of corticosteroids in the treatment of peritonsillar abscess: A meta-analysis. Clinical and Experimental Otorhinolaryngology, 9(2), 89-97.
52. Lemiengre, M. B., van Driel, M. L., Merenstein, D., Liira, H., Mäkelä, M., & De Sutter, A. I. M. (2018). Antibiotics for acute rhinosinusitis in adults. Cochrane Database of Systematic Reviews, 2018(9), CD006089.
53. Lin, J. L., Ramirez, M. R., & Smith, N. L. (2016). Epiglottitis: It hasn’t gone away. Anesthesiology, 124(6), 1404-1410.
54. Liu, J. H., Anderson, K. E., Willging, J. P., Myer, C. M. III, Shott, S. R., Bratcher, G. O., & Cotton, R. T. (2001). Posttonsillectomy hemorrhage: What is it and what should be recorded? Archives of Otolaryngology–Head & Neck Surgery, 127(10), 1271-1275.
55. Long, B., & Gottlieb, M. (2023). Managing peritonsillar abscess. Annals of Emergency Medicine, 82(1), 101-107.
56. Long, B., Langille, M., Rosenberg, H., & Atkinson, P. (2024). Just the facts: Evaluation and management of epistaxis. Canadian Journal of Emergency Medicine.
57. Makhdom, R. (2023). Ultrasound in tonsillitis – Submandibular approach. Emergency Medicine Simulation Journal.
58. Mitchell, R. B., Archer, S. M., Ishman, S. L., Rosenfeld, R. M., Coles, S., Finestone, S. A., Friedman, N. R., Giordano, T., Hildrew, D. M., Kim, T. W., Lloyd, R. M., Parikh, S. R., Shulman, S. T., Walner, D. L., Walsh, S. A., & Nnacheta, L. C. (2019). Clinical practice guideline: Tonsillectomy in children (update). Otolaryngology–Head and Neck Surgery, 160(1S), S1–S42.
59. Munroe, K. M., Sowerby, L. J., & Chin, C. J. (2020). Is topical tranexamic acid effective in treating epistaxis? Journal of Otolaryngology – Head & Neck Surgery, 49(1), 50.
60. Murano, T., Brucato-Duncan, D., Ramdin, C., & Keller, S. (2019). Prophylactic systemic antibiotics for anterior epistaxis treated with nasal packing in the ED. American Journal of Emergency Medicine, 37(5), 726-729.
61. Newton, E., Lasso, A., Petrcich, W., & Kilty, S. J. (2016). An outcomes analysis of anterior epistaxis management in the emergency department. Journal of Otolaryngology – Head and Neck Surgery, 45(24).
62. Orlandi, R. R., Kingdom, T. T., Smith, T. L., Bleier, B., DeConde, A., Luong, A. U., Poetker, D. M., Soler, Z. M., Welch, K. C., Wise, S. K., Adappa, N., Alt, J. A., Anselmo-Lima, W. T., Bachert, C., Baroody, F. M., Batra, P. S., Bernal-Sprekelsen, M., Beswick, D., Bhattacharyya, N., … Wormald, P. J. (2021). International consensus statement on allergy and rhinology: Rhinosinusitis 2021. International Forum of Allergy & Rhinology, 11, 213–739.
63. Powell, J., & Wilson, J. A. (2012). An evidence-based review of peritonsillar abscess. Clinical Otolaryngology, 37(2), 136-145.
64. Reuben, A., Appelboam, A., Stevens, K. N., Vickery, J., Ewings, P., Ingram, W., Jeffery, A. N., Body, R., Hilton, M., Coppell, J., Wainman, B., & Barton, A. (2021). The use of tranexamic acid to reduce the need for nasal packing in epistaxis (NoPAC): Randomized controlled trial. Annals of Emergency Medicine, 77(6), 631-640.
65. Rosenfeld, R. M., Andes, D., Bhattacharyya, N., Cheung, D., Eisenberg, S., Ganiats, T. G., Gelzer, A., Hamilos, D., Haydon, R. C., Hudgins, P. A., Jones, S., Krouse, H. J., Lee, L. H., Mahoney, M. C., Marple, B. F., Mitchell, J. P., Nathan, R., Shiffman, R. N., Smith, T. L., & Witsell, D. L. (2016). Clinical practice guideline: Adult sinusitis. Otolaryngology–Head and Neck Surgery, 137(S1), S1–S31.
66. Rosenfeld, R. M., Piccirillo, J. F., Chandrasekhar, S. S., Brook, I., Kumar, K. A., Kramper, M., & Orlandi, R. R. (2015). Clinical practice guideline (update): Adult sinusitis. Otolaryngology–Head and Neck Surgery, 152(4), 598–609.
67. Rosenfeld, R. M., Piccirillo, J. F., Chandrasekhar, S. S., Brook, I., Kumar, K. A., Kramper, M., Orlandi, R. R., Palmer, J. N., Patel, Z. M., Peters, A., Walsh, S. A., & Corrigan, M. D. (2015). Clinical practice guideline (update): Adult sinusitis. Otolaryngology–Head and Neck Surgery, 152(2S), S1–S39.
68. Sadeghirad, B., Siemieniuk, R. A. C., Brignardello-Petersen, R., Papola, D., Lytvyn, L., Vandvik, P. O., Merglen, A., Guyatt, G. H., & Agoritsas, T. (2017). Corticosteroids for treatment of sore throat: Systematic review and meta-analysis of randomised trials. BMJ, 358, j3887.
69. Schumaker, H. M., Doris, P. E., & Birnbaum, G. (1984). Radiographic parameters in adult epiglottitis. Annals of Emergency Medicine, 13(8), 588–590.
70. Schwarz, W., Ruttan, T., & Bundick, K. (2019). Nebulized tranexamic acid use for pediatric secondary post-tonsillectomy hemorrhage. Annals of Emergency Medicine, 73, 269–271.
71. Secko, M., & Sivitz, A. (2015). Think ultrasound first for peritonsillar swelling. American Journal of Emergency Medicine, 33(4), 569–572.
72. Shaikh, N., Kais, A., Dewey, J., & Jaffal, H. (2024). Effect of perioperative ketorolac on postoperative bleeding after pediatric tonsillectomy. International Journal of Pediatric Otorhinolaryngology, 180, 111953.
73. Sideris, A., Holmes, T. R., Cumming, B., & Havas, T. (2019). A systematic review and meta‐analysis of predictors of airway intervention in adult epiglottitis. The Laryngoscope, 130(2), 465–473.
74. Siu, J. M., Propst, E. J., & Wolter, N. E. (2024). Post-tonsillectomy hemorrhage in children. Canadian Medical Association Journal, 196(41), E1374.
75. Sobol, S. E., & Zapata, S. (2008). Epiglottitis and croup. Otolaryngologic Clinics of North America, 41(3), 551–566.
76. Spencer, R., Newby, M., Hickman, W., Williams, N., & Kellermeyer, B. (2022). Efficacy of tranexamic acid (TXA) for post-tonsillectomy hemorrhage. American Journal of Otolaryngology–Head and Neck Medicine and Surgery, 43, 103582.
77. Spires, J. R., Owens, J. J., Woodson, G. E., & Miller, R. H. (1987). Treatment of peritonsillar abscess: A prospective study of aspiration vs incision and drainage. Archives of Otolaryngology–Head & Neck Surgery, 113(9), 984-986.
78. Tran, Q. K., Barnett, J., O’Connell, F., D’Anza, B., & Pourmand, A. (2021). Nasal packing in the emergency department: A practical review for emergency providers. Open Access Emergency Medicine, 13, 527-533.
79. Tran, Q. K., Rehan, M. A., Haase, D. J., Matta, A., & Pourmand, A. (2020). Prophylactic antibiotics for anterior nasal packing in emergency department: A systematic review and meta-analysis of clinically significant infections. American Journal of Emergency Medicine, 38, 983-989.
80. Tunkel, D. E., Anne, S., Payne, S. C., Ishman, S. L., Rosenfeld, R. M., Abramson, P. J., Benoit, M. M., Bercovitz, R. S., Brown, M. D., Chernobilsky, B., Feldstein, D. A., Hackell, J. M., Holbrook, E. H., Holdsworth, S. M., Lin, K. W., Lind, M. M., Poetker, D. M., Riley, C. A., Schneider, J. S., … Monjur, T. M. (2020). Clinical practice guideline: Nosebleed (epistaxis). Otolaryngology–Head and Neck Surgery, 162(1S), S1–S38.
81. Tunkel, D. E., Anne, S., Payne, S. C., Ishman, S. L., Rosenfeld, R. M., Abramson, P. J., Benoit, M. M., Bercovitz, R. S., Brown, M. D., Chernobilsky, B., Feldstein, D. A., Hackell, J. M., Holbrook, E. H., Holdsworth, S. M., Lin, K. W., Lind, M. M., Poetker, D. M., Riley, C. A., Schneider, J. S., … Monjur, T. M. (2020). Clinical practice guideline: Nosebleed (epistaxis) executive summary. Otolaryngology–Head and Neck Surgery, 162(1), 8–25.
82. Tunkel, D. E., Anne, S., Payne, S. C., Ishman, S. L., Rosenfeld, R. M., Abramson, P. J., Benoit, M. M., Bercovitz, R. S., Brown, M. D., Chernobilsky, B., Feldstein, D. A., Hackell, J. M., Holbrook, E. H., Holdsworth, S. M., Lin, K. W., Lind, M. M., Poetker, D. M., Riley, C. A., Schneider, J. S., … Monjur, T. M. (2020). Clinical practice guideline: Nosebleed (epistaxis). Otolaryngology–Head and Neck Surgery, 162(1S), S1–S38.
83. Hung, T. Y., Li, S., Chen, P. S., Wu, L., Yang, Y. J., Tseng, L. M., Chien, K. C. (2011). Bedside ultrasonography as a safe and effective tool to diagnose acute epiglottitis. American Journal of Emergency Medicine, 29(3), 359.e1–359.e3.
84. Urban, M. J., Masliah, J., Heyd, C., Patel, T. R., & Nielsen, T. (2021). Peritonsillar abscess size as a predictor of medical therapy success. Annals of Otology, Rhinology & Laryngology, 131(2), 211-218.
85. Zahed, R., Moharamzadeh, P., Alizadeh Arasi, S., Ghasemi, A., & Saeedi, M. (2013). A new and rapid method for epistaxis treatment using injectable form of tranexamic acid topically: A randomized controlled trial. American Journal of Emergency Medicine, 31(9), 1389–1392.
86. Zahed, R., Mousavi Jazayeri, M. H., Naderi, A., Naderpour, Z., & Saeedi, M. (2017). Topical tranexamic acid compared with anterior nasal packing for treatment of epistaxis in patients taking antiplatelet drugs: Randomized controlled trial. Academic Emergency Medicine, 24(3), 360–366.
Online Resources:
1. Acute sinusitis and rhinosinusitis in adults: Clinical manifestations and diagnosis. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/acute-sinusitis-and-rhinosinusitis-in-adults-clinical-manifestations-and-diagnosis
2. Approach to the adult with epistaxis. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/approach-to-the-adult-with-epistaxis
3. Chronic rhinosinusitis with nasal polyposis: Management and prognosis. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/chronic-rhinosinusitis-with-nasal-polyposis-management-and-prognosis
4. Chronic rhinosinusitis without nasal polyposis: Management and prognosis. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/chronic-rhinosinusitis-without-nasal-polyposis-management-and-prognosis
5. Chronic rhinosinusitis: Clinical manifestations, pathophysiology, and diagnosis. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/chronic-rhinosinusitis-clinical-manifestations-pathophysiology-and-diagnosis
6. Epiglottitis (supraglottitis): Clinical features and diagnosis. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/epiglottitis-supraglottitis-clinical-features-and-diagnosis
7. Epiglottitis (supraglottitis): Management. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/epiglottitis-supraglottitis-management
8. Peritonsillar cellulitis and abscess. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/peritonsillar-cellulitis-and-abscess
9. Uncomplicated acute sinusitis and rhinosinusitis in adults: Treatment. UpToDate. Retrieved February 12, 2025, from https://www.uptodate.com/contents/uncomplicated-acute-sinusitis-and-rhinosinusitis-in-adults-treatment
