

In this second post on Primary Care in the ED we are going to focus on the acute management and treatment of depression. In part one we focused on HTN and COPD – read more here.
ED visits for mental health are rising, and many patients use the ED as their first point of contact into the mental health system.¹⁶ Our typical focus for these patients involves safety assessments, particularly around suicide risk — and we can probably do a lot better. More than one in three patients with a mood, anxiety, or substance-use disorder report unmet care needs.¹⁷ We also know that earlier treatment improves the chance of remission and that untreated depression is a risk factor for suicide.Let’s expand our knowledge of depression by reviewing the most up-to-date Canadian depression guidelines (CANMAT).¹⁸
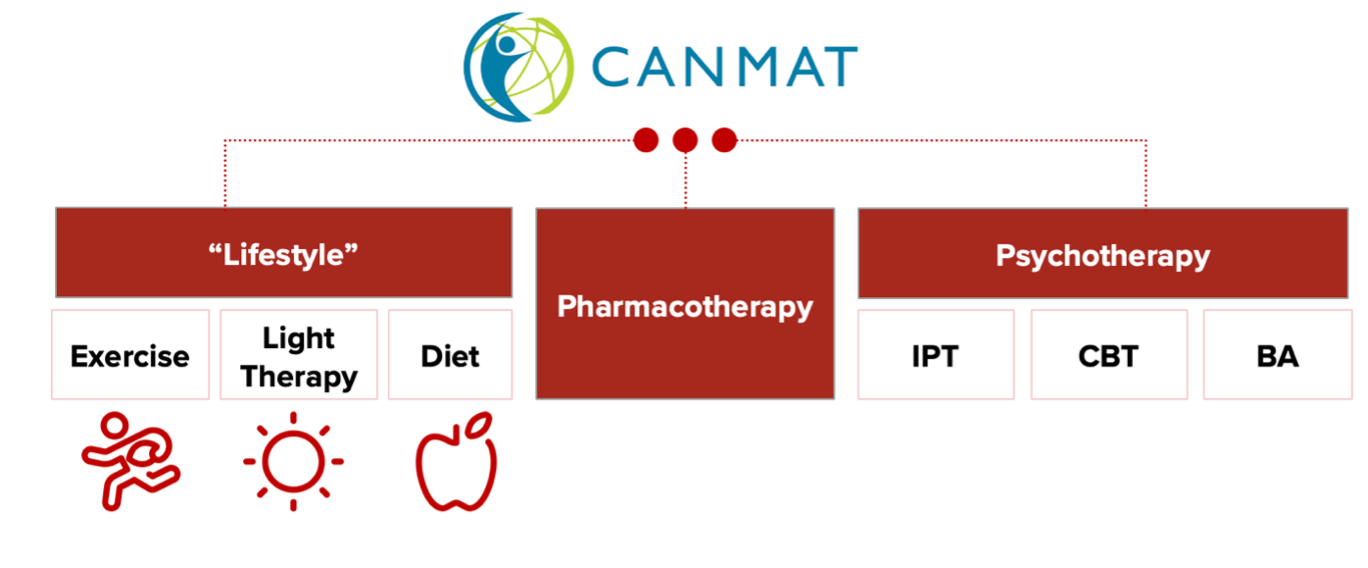
These guidelines provide a comprehensive, multimodal approach to treat all types of depression, but for our purposes we’ll focus on the treatment of mild and moderate depression, looking at exercise as therapy, medication, and psychotherapy.
1. Exercise
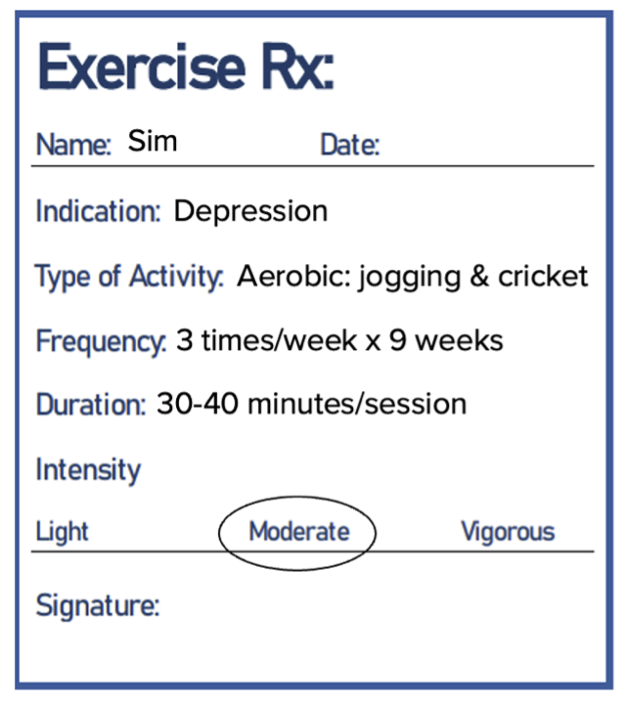
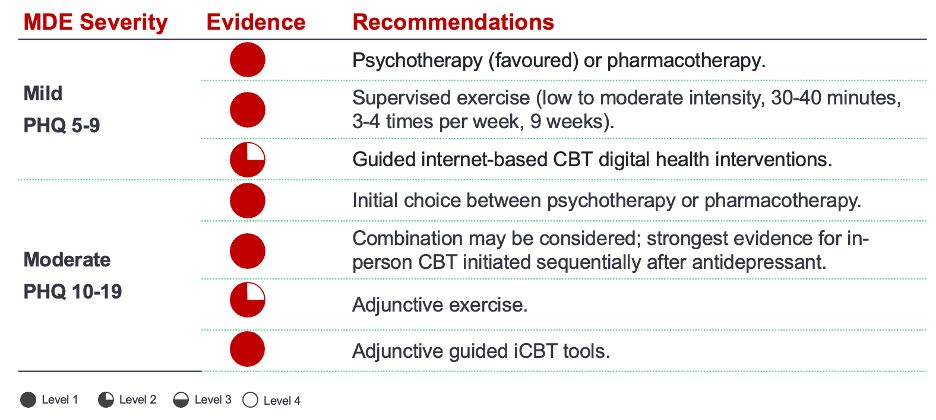
When it comes to lifestyle interventions, one of the most interesting and well-studied approaches in depression is exercise. Supervised exercise (low-to-moderate intensity, for 30–40 minutes at a time, three to four times a week for at least nine weeks) is recommended as a first-line agent in mild depression and as an adjunct in moderate depression.¹⁸
High-quality research continues to demonstrate effectiveness comparable to first-line pharmacotherapy and psychotherapy:
-
2023 meta-analysis: 41 RCTs (2 264 participants) showed that moderate- or vigorous-intensity aerobic or resistance exercise decreased depressive symptoms (NNT = 2), comparable to psychotherapy or pharmacotherapy.¹⁹
-
Systematic review: Seven RCTs (1 020 patients) found exercise significantly reduced suicidal ideation and behaviours.²⁰
-
2024 network analysis: Various exercise modalities were as effective as pharmacotherapy and psychotherapy, with benefits increasing with intensity, though even small amounts (e.g., yoga) were beneficial.²¹
These studies had limitations — most involved supervised programs and participants with mild depression who were motivated to engage. For patients with anhedonia and lack of motivation, adherence is difficult; thus, exercise is recommended as monotherapy only for mild cases, yet adjunctive for all.
Prescribing Exercise:
- Involve patients in shared decision-making.
- Write a prescription specifying activity type, frequency, duration, and intensity — and choose something the patient enjoys.
- Guidelines recommend low-to-moderate intensity for 30–40 minutes, three to four times weekly, for nine weeks.¹⁸
- Any exercise is better than none.²²
Take-home Point #1: Exercise is first-line monotherapy in mild depression and adjunctive second-line for all forms of depression. Any exercise is better than none.
2. Pharmacotherapy (SSRI, SNRI)
SSRIs are first-line for moderate depression and may be considered in mild cases if psychotherapy isn’t readily available. Pharmacotherapy and psychotherapy are equally effective as initial treatments, but the strongest evidence supports a sequential approach — starting with SSRIs and then adding CBT for long-term benefit.
Choosing an antidepressant:
All have similar efficacy; selection depends on comorbidities, prior response, and side-effect profile.
- Previous response → use that one
- Chronic pain or somatization → duloxetine
- Multiple medications → avoid fluoxetine & paroxetine (long-half life)
- Sexual side effects → desvenlafaxine, bupropion
- Cardiac disease → sertraline
- <18 years → fluoxetine
In speaking with some of our local psychiatry experts about choices they commented:
“One thing to note is that initiating cipralex (escitalopram) is very easy from the ED. You give them a prescription of 5 mg daily x 1 week, then increase to 10 mg daily (the lowest effective dose)”
Your post-ED counselling should include follow-up with a primary care provider in approximately 2-3 weeks and review of side effects including:
- Gastrointestinal (n/v/diarrhea/constipation)
- Sedation/fatigue/dizziness
- Anti-cholinergic (orthostasis, dry mouth)
- Insomnia / agitation
- Weight gain
- Sexual dysfunction
- QT prolongation
- Other: mania precipitation, discontinuation syndrome
- Suicidal ideation *
* A Review: Suicidality and Antidepressants
One of the biggest concerns of providers prescribing antidepressants with no follow-up is suicide risk.
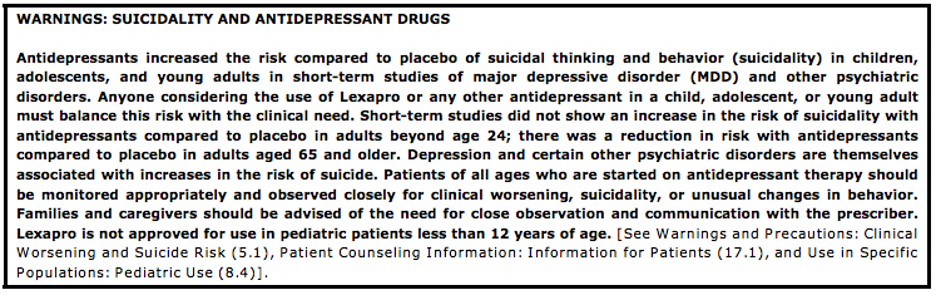
While collectively, the evidence supports the conclusion that antidepressants reduce suicidal thoughts and behaviours, the take-home point is that in the <25 age group, there is a slight increase in overall suicidality as a composite measure – but this is not representative of suicide completions – and should be balanced against the known real risk of untreated depression.
If you’re curious about this, we’ll dive a bit deeper into the evidence and controversy:
In 2004, the United States FDA issued a Black Box warning after placebo-controlled trials showed an increased risk of suicidal thoughts and behaviors in children and adolescents taking antidepressants compared to placebo and in 2007, they expanded the warning to include young adults aged 18-24. Health Canada issued similar warnings.
The data underpinning these recommendations stemmed from 2 studies:
- A 2006 meta-analysis reviewing 4,582 patients across 24 trials assessing the relationship between antidepressant drugs and suicidality in pediatric patients, with an increased relative risk of suicidal ideation relative to control but no completed suicides23.
- A larger meta-analysis of 372 double blind randomized placebo-controlled trials of almost 100,000 patients. Their primary composite outcome was suicidality – defined as suicidal ideation or worse (including completed suicide, suicide attempts, and preparatory acts). They noted no significant differences with all groups combined, but in age-stratified analysis: increased risk among children and adolescent <25, no evidence of increased risk among adults >25, and among adults 65 and older, a clear protective benefit24.
However, it is important to note that the actual event rates and absolute risk were quite low. There were only 8 completed suicides, which again did not differ significantly between any group. And in that <25 group, when you look at the pure event rate for their outcome, the actual absolute risk difference between the groups was less than 1%.
These warnings sparked a tremendous amount of controversy as population health data following these studies and subsequent warnings demonstrated a concurrent drop in depression diagnoses, prescriptions, and a rise in actual suicide25. Many were also quick to point out that these studies and RCT’s were reflective of short-term efficacy – usually in the 4 to 12-week range and not long-term safety25.
So, all in all, while the data shows a trend towards increased relative risk of suicidality in this age group, it reflects short-term risk, it’s a low absolute relative risk, it does not equate to rates of suicidal completion, and should be balanced against the rates of untreated depression in terms of morbidity and mortality with a real risk of suicide. This is in alignment with our local practice experts in child/adolescent and adult psychiatry, who highlight the need to counsel patients and the importance of follow-up, citing that these warnings were meant to encourage discussion and dialogue about suicidality, but not to avoid prescribing.
So… should we be prescribing in the ED?
Ultimately this is going to come down to personal preference and your local practice environment. But with all of this evidence in mind, here is my own personal checklist of who I would consider starting on an antidepressant:
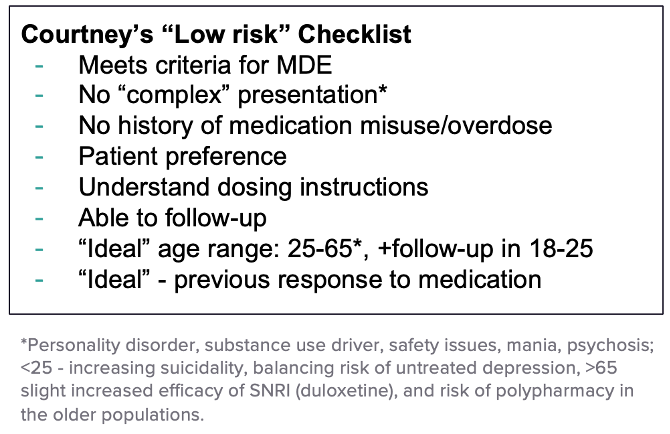
Take home point #2: Escitalopram (Cipralex) 5mg x 1 week, followed by 10mg, is a reasonable choice for many “low risk” individuals, provided they are engaged in treatment, understand dosing, and agree to follow-up.
If you want to learn more details about antidepressants and depression resources, check out the Ottawa Depression Algorithm.
3. Psychotherapy
Finally, our last component of our approach to depression – therapy.
It is considered first line for both mild and moderate depression, as an either/or option, preferred for mild given its lack of side effects and efficacy, and recommended strongly for consideration of combination with pharmacotherapy in moderate depression, given the evidence around combined effects. It also has the most evidence for sustained treatment effects long-term in the 6 to 12-month range.
Types of Therapy
From the ED, we probably aren’t thinking about the different kinds of therapy that might be best for the patients we see. And it’s not a one-size fits all approach.
In the CANMAT guidelines, there is mention of multiple modalities (cognitive behaviour therapy, interpersonal therapy, behavioural activation), that are effective for depression, with a simultaneous recognition that conclusions are limited because it is inherently difficult to study.
I had a discussion with one of our local clinical psychologist Dr. Krause about different types of therapies for depression:
“In general, in clinical practice, cognitive behavioural therapy (CBT) is favoured, and when you look at the evidence and dismantle the therapy components, at least for more severe forms of depression, behavioural activation is what becomes most important. Incorporating the “C” becomes more relevant for patients with comorbid mental health conditions, specifically anxiety, as the cognitive strategies around distorted thought patterns is what is most helpful.”
What is behavioural activation?
In its simplest terms, behavioural activation is doing something that increases pleasure or improves mastery – and they can be small things, like going for a walk, or cleaning your kitchen. It is intended to get patients out of what’s called the “vicious cycle of depression”, which is basically that the more depressed you are, the less you do, and therefore the more depressed you get. And by doing more things, you improve your energy, mood, activity, and become less depressed.
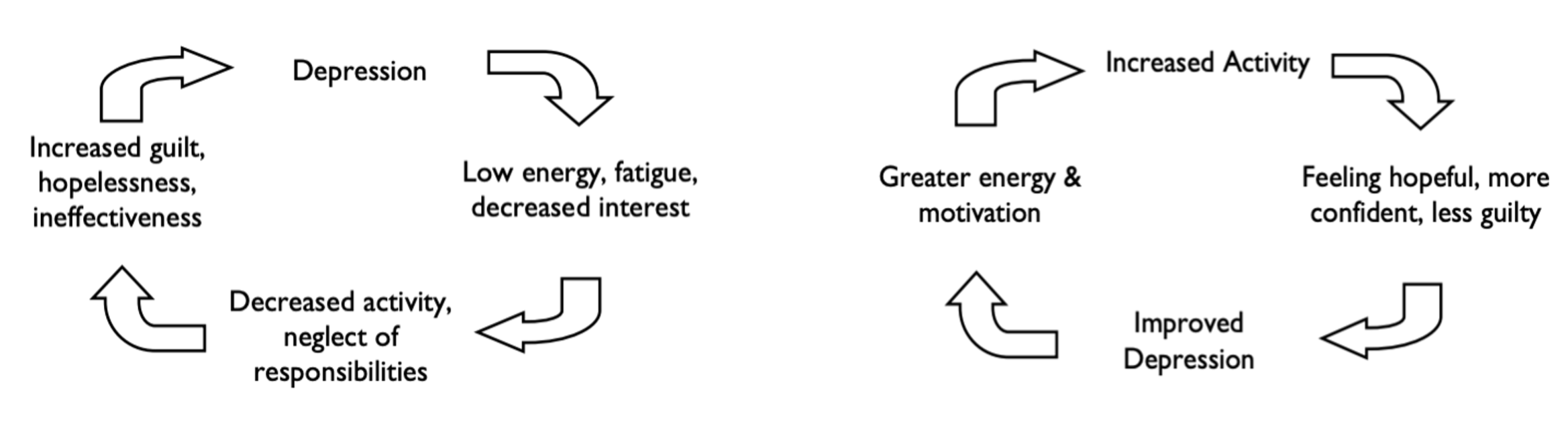
In a therapy format, it uses techniques like goal and activity setting, with having patients predict future enjoyability in an objective way for longitudinal mood tracking. For example, rating how they think they are going to feel before and after a walk with a friend, to call out their internal distortions and see that overtime, doing things makes them feel better.
Dr. Krause, our clinical psychology expert, pointed me towards the Centre for Clinical Interventions resources, which include behavourial activation worksheets, fun activities, and weekly mood schedules you can provide to patients on your next shift26.
Administering Therapy
When it comes to looking for therapists to deliver these modalities – what specific guidance should we give patients? How long do they go for, and what should they look for?
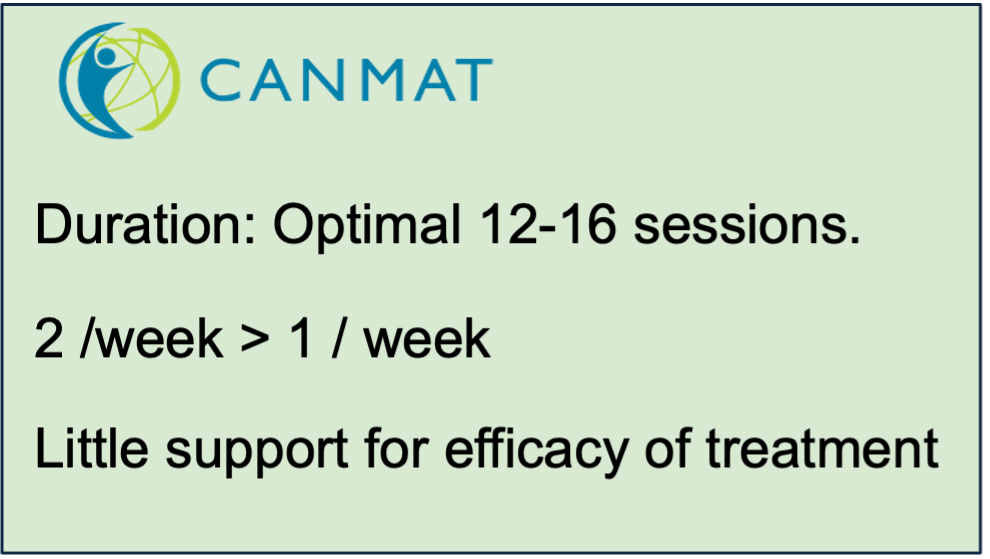
In CANMAT, the optimal timeline for therapy is 12-16 sessions with twice weekly or weekly sessions with the most evidence behind it. We should also be highlighting to patients the importance of at least once per week therapy, at least in the early acute depressive episode phase, as there is little evidence for treatment efficacy with therapy delivered less than once per week18.
In terms of what to look for, our local expert Dr. Krause’s “finding a counsellor tips” includes:
- Prioritizing a focus on behavioural activation.
- Ensuring you are getting structured homework.
- If seeing no improvement in 4-5 weeks, consider a new therapist.
Something that I incorporate on shift with patients who are working with therapists is asking “what kinds of things are you working on, or working towards?” We then talk about having objectives, goals, homework and structure with the overarching goal that therapy should be simultaneously challenging and supportive.
Finding a Therapist and Digital Solutions
And finally, when it comes to finding a therapist, this is going to be a real struggle for many patients and dependent on your local contexts.
Patients may often ask you about digital health technologies, apps or free solutions they can use that might be beneficial given financial barriers. Although not extensive list, below are some guided and non-guided options mentioned in CANMAT that you might consider for patients:
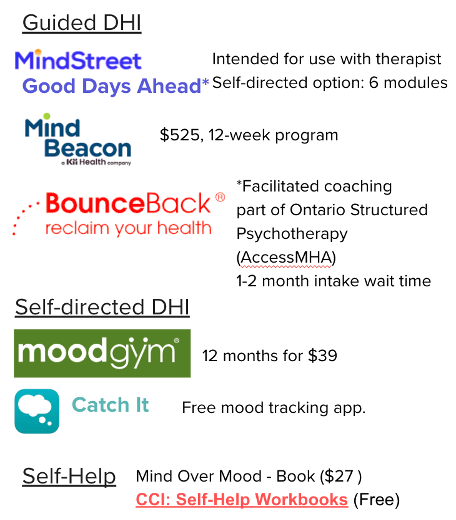
However, it is important to note that digital health tools have best efficacy only for mild cases, in patients who are motivated, with the most evidence for guided (i.e. someone coaching you through it), particularly for internet-based CBT over unguided (i.e. self-directed tools.). For this reason, these tools should be considered only as monotherapy in cases of mild depression with patient preference27.
Take Home Points
- Not all therapy is the same.
- An important component of therapy for depression is behavioural activation.
- Guided>unguided digital health interventions for mild depression
References
- Duong D, Vogel National survey highlights worsening primary care access. CMAJ. 2023 Apr 24;195(16):E592–E593. Available from: https://www.cmaj.ca/content/195/16/E592
- Ontario College of Family Physicians. New survey shows full‑blown crisis in family medicine [Internet]. May 30, 2023 [cited 2025 Jan 24]. Available from: https://ontariofamilyphysicians.ca/news/new-survey-shows-full-blown-crisis-in-family-medicine/
- Statistics Canada. (2019). Primary health care providers, 2017. Health Reports, 30(2), 3–11. Retrieved January 24, 2025, from https://www150.statcan.gc.ca/n1/pub/82-003-x/2019002/article/00001-eng.htm
- Tobe, S., Harvey, P., Mabaya, G., & Summers, D. (2024). A NEW QUALITY STANDARD FOR HYPERTENSION: GUIDING EVIDENCE-BASED, HIGH-QUALITY CARE IN ONTARIO. Canadian Journal of Cardiology, 40(10), S132.
- Weaver CG, Clement F, Campbell N et al. Health Care Costs Attributable to Hypertension: a Canadian Population-Based Cohort Study. Hypertension. 2015;66:00-00. DOI: 10.1161/HYPERTENSIONAHA.115.05702.
- Masood S, Austin PC, Atzema CL. A population-based analysis of outcomes in patients with a primary diagnosis of hypertension in the emergency department. Annals of emergency medicine. 2016 Sep 1;68(3):258-67.
- Hypertension Canada. (2024). Hypertension: Introducing a new standard for high-quality care in Ontario. Retrieved January 24, 2025, from https://hypertension.ca/news/hypertension-introducing-a-new-standard-for-high-quality-care-in-ontario/#:~:text=Patient%20outcomes%20for%20hypertension%20can,home%20and%20community%20care%20settings
- Michaud, A., Lamarre-Cliche, M., Vadeboncoeur, A., & Cloutier, L. (2020). Screening for hypertension in adults during emergency department consultation: a systematic review. European Journal of Emergency Medicine, 27(3), 178-185
- Dieterle, T., Schuurmans, M. M., Strobel, W., Battegay, E. J., & Martina, B. (2005). Moderate-to-severe blood pressure elevation at ED entry: hypertension or normotension?. The American journal of emergency medicine, 23(4), 474-479.
- Wolf, S. J., Lo, B., Shih, R. D., Smith, M. D., & Fesmire, F. M. (2013). Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Annals of emergency medicine, 62(1), 59-68.
- Todd, B. R., Xing, Y., Zhao, L., Nguyen, A., Swor, R., Eberhardt, L., & Bahl, A. (2024). Antihypertensive prescription is associated with improved 30‐day outcomes for discharged hypertensive emergency department patients. Journal of the American College of Emergency Physicians Open, 5(2), e13138.
- Oras, P., Häbel, H., Skoglund, P. H., & Svensson, P. (2020). Elevated blood pressure in the emergency department: a risk factor for incident cardiovascular disease. Hypertension, 75(1), 229-236.
- McAlister, F. A., Youngson, E., & Rowe, B. H. (2021). Elevated blood pressures are common in the emergency department but are they important? A retrospective cohort study of 30,278 adults. Annals of Emergency Medicine, 77(4), 425-432.
- Brody, A., Rahman, T., Reed, B., Millis, S., Ference, B., Flack, J. M., & Levy, P. D. (2015). Safety and efficacy of antihypertensive prescription at emergency department discharge. Academic Emergency Medicine, 22(5), 632-635.
- Goupil, R., Tsuyuki, R. T., Santesso, N., Terenzi, K. A., Habert, J., Cheng, G., … & Hundemer, G. L. (2025). Hypertension Canada guideline for the diagnosis and treatment of hypertension in adults in primary care. CMAJ, 197(20), E549-E564.
- Ontario Health. (2021). Summary report. https://www.ontariohealth.ca/sites/ontariohealth/files/2021-02/Summary.pdf
- 1 in 3 unmet care needs – Statistics Canada. (2023). Who are the gig workers in Canada? Retrieved January 24, 2025, from https://www150.statcan.gc.ca/n1/pub/11-627-m/11-627-m2023053-eng.htm
- Lam, RW, Kennedy, SH, Adams, C., Bahji, A., Beaulieu, S., Bhat, V., … & Milev, RV (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults. The Canadian Journal of Psychiatry , 07067437241245384.
- Heissel, A., Heinen, D., Brokmeier, L. L., Skarabis, N., Kangas, M., Vancampfort, D., … & Schuch, F. (2023). Exercise as medicine for depressive symptoms? A systematic review and meta-analysis with meta-regression. British journal of sports medicine, 57(16), 1049-1057.
- Fabiano, N., Gupta, A., Fiedorowicz, J. G., Firth, J., Stubbs, B., Vancampfort, D., … & Solmi, M. (2023). The effect of exercise on suicidal ideation and behaviors: A systematic review and meta-analysis of randomized controlled trials. Journal of affective disorders, 330, 355-366.
- Noetel, M., Sanders, T., Gallardo-Gómez, D., Taylor, P., del Pozo Cruz, B., Van Den Hoek, D., … & Lonsdale, C. (2024). Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. bmj, 384.
- Zhou, C., Puder, D., & Fabiano, N. (2024). How to prescribe physical activity for depression. Sports Psychiatry: Journal of Sports and Exercise Psychiatry.
- Hammad, T. A., Laughren, T., & Racoosin, J. (2006). Suicidality in pediatric patients treated with antidepressant drugs. Archives of general psychiatry, 63(3), 332-339.
- Stone, M., Laughren, T., Jones, M. L., Levenson, M., Holland, P. C., Hughes, A. ….. & Rochester, G. (2009). Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration. Bmj, 339.
- Friedman, R. A. (2014). Antidepressants’ black-box warning—10 years later. New England Journal of Medicine, 371(18), 1666-1668.
- Centre for Clinical Interventions. Looking After Yourself: Self‑help resources for mental health problems [Internet]. Perth (Australia): CCI; 2024 Jan 16 [cited 2025 Jun 24]. Available from: https://www.cci.health.wa.gov.au/resources/looking-after-yourself
- Lam, RW, Kennedy, SH, Adams, C., Bahji, A., Beaulieu, S., Bhat, V., … & Milev, RV (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults. The Canadian Journal of Psychiatry , 07067437241245384.
- Blazer, A. J., & Stanbrook, M. B. (2023). How can Canada’s health systems improve care for people with chronic obstructive pulmonary disease?. CMAJ, 195(35), E1182-E1183.
- Bourbeau, J., Bhutani, M., Hernandez, P., Aaron, S. D., Beauchesne, M. F., Kermelly, S. B., … & Marciniuk, D. D. (2023). 2023 Canadian Thoracic Society guideline on pharmacotherapy in patients with stable COPD. Chest.
- Papaioannou AI, Hillas G, Loukides S, Vassilakopoulos T. Mortality prevention as the centre of COPD management. ERJ Open Res. 2024 Jun 17;10(3):00850-2023. doi: 10.1183/23120541.00850-2023. PMID: 38887682; PMCID: PMC11181087.
- Coutinho, A. D., Lokhandwala, T., Boggs, R. L., Dalal, A. A., Landsman-Blumberg, P. B., Priest, J., & Stempel, D. A. (2016). Prompt initiation of maintenance treatment following a COPD exacerbation: outcomes in a large insured population. International Journal of Chronic Obstructive Pulmonary Disease, 1223-1231.
- Diab, N., Gershon, A. S., Sin, D. D., Tan, W. C., Bourbeau, J., Boulet, L. P., & Aaron, S. D. (2018). Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. American journal of respiratory and critical care medicine, 198(9), 1130-1139.
- University of Ottawa. (n.d.). Confronting the crisis: DFMS comprehensive strategy lays out a path to primary care for all. Retrieved January 24, 2025, from https://www.uottawa.ca/en/news-all/confronting-crisis-dfms-comprehensive-strategy-lays-out-path-primary-care-all
Thank you! That was a very relevant and nice topic to read!
Really enjoyed this piece. It does a great job highlighting how often depression surfaces in the ED and why follow up care truly matters. The emphasis on practical treatment options and continuity really stood out.
It’s a good reminder that strong, accessible primary care, including personalized and preventive approaches, can help patients get support earlier and potentially avoid crisis level visits. Thanks for shedding light on such an important topic!