

Abnormal uterine bleeding is a common and often disruptive presentation in the Emergency Department, and it can range from a benign nuisance to a sign of significant pathology. This post aims to equip ED clinicians with a practical, patient-centered approach to evaluating and managing AUB in pre-menopausal patients.
Please note that this blog post may use various terms such as person who menstruates, patient, or woman. While most patients with abnormal uterine bleeding are cisgendered women, any person with a uterus can present to the ED with this issue and it is important to include all patients in the conversation of this topic.
By the end of this post, the goal is to achieve a practical approach to Abnormal Uterine Bleeding in the ED including:
- Definition
- Etiology
- Clinical Approach
- Investigations
- Management
Defining AUB
Abnormal Uterine Bleeding (AUB)
“variation from the normal menstrual cycle, and includes changes in regularity and frequency of menses, in duration of flow or in amount of blood loss”
The main guidelines discussed will be the SOGC Clinical Practice Guidelines on Abnormal Uterine Bleeding in Pre-Menopausal Women.
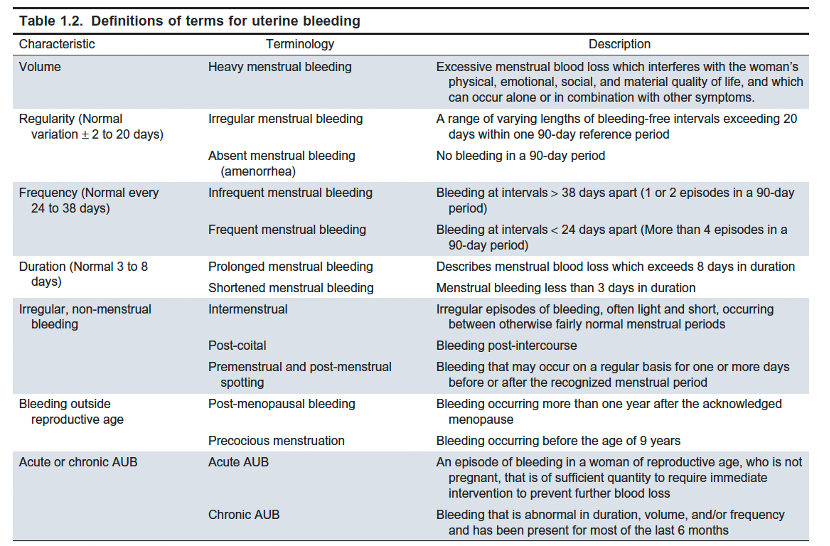
Their first recommendation is that we should consider the “Adoption of standardized international terminology for abnormal uterine bleeding” [1]. The FIGO menstrual disorders working group [1] involved international clinicians and established new definitions that were simple, descriptive, and understood by both physicians and patients.
They suggested that words like menorrhagia, metrorrhagia, hypermenorrhea and dysfunctional uterine bleeding, be abandoned and rather fall under the umbrella term AUB.
Singh S, Best C, Dunn S, Leyland N, Wolfman WL. No. 292-Abnormal Uterine Bleeding in Pre-Menopausal Women. Journal of Obstetrics and Gynaecology Canada. 2018 May 1;40(5):e391–415. https://pubmed.ncbi.nlm.nih.gov/29731212/
Heavy Menstrual Bleeding (HMB)
“excessive menstrual blood loss which interferes with the woman’s physical, social, emotional, and/or material quality of life [that] can occur alone or in combination with other symptoms.”
As with other newer definitions, a more holistic approach is encompassed into these definitions instead of quantifying a certain number of mL of blood or number of soaked pads.
While this definition with a focus on quality of life is helpful, it may still clinically beneficial to attempt to quantify bleeding. We traditionally characterized HMB as more than 80mL of bleeding. With modern menstrual products, it can be surprisingly easy to reach that number. A study assessing different menstrual products by DeLoughery et al showed that saturation of 2 heavy pads (100mL) or 3 heavy tampons over the course of a whole menstrual cycle constituted HMB [2]. This study showed such a variability between products that our traditional questions of “how often do you change your pads/tampon” may not be as telling as we thought.

https://www.canada.ca/en/women-gender-equality/funding/equality-action/menstrual-equity.html
Period poverty is present in Canada with 1 in 6 Canadians who menstruate are unable to consistently afford menstrual products. Therefore, the tool we use to assess HMB may not even be applicable in this patient [3]. This can lead to increased rates of underdiagnosis and undertreatment in those who are most vulnerable. It becomes a cycle affecting those who are most socioeconomically disadvantaged when undertreatment leads to missed school or work, further limiting economic and education opportunities.

https://www.canada.ca/en/women-gender-equality/funding/equality-action/menstrual-equity.html
The 2021 proposed definition by an international von Willebrand disease working group can be helpful as it points out various symptoms, signs and scores that could be in keeping with heavy menstrual bleeding. [4]
Menstrual bleeding meeting any of the following criteria:
- Lasting ≥8 days
- Consistently soaks through 1 or more sanitary protections every 2 hours on multiple days
- Requires use of >1 sanitary protection item at a time
- Requires changing sanitary protection during the night
- Associated with repeat passing of blood clots
- Pictorial Blood Assessment Chart (PBAC) score >100
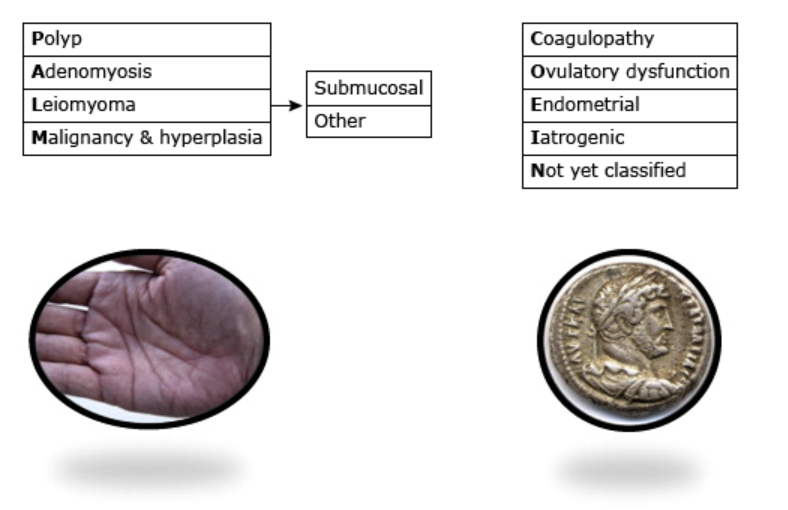
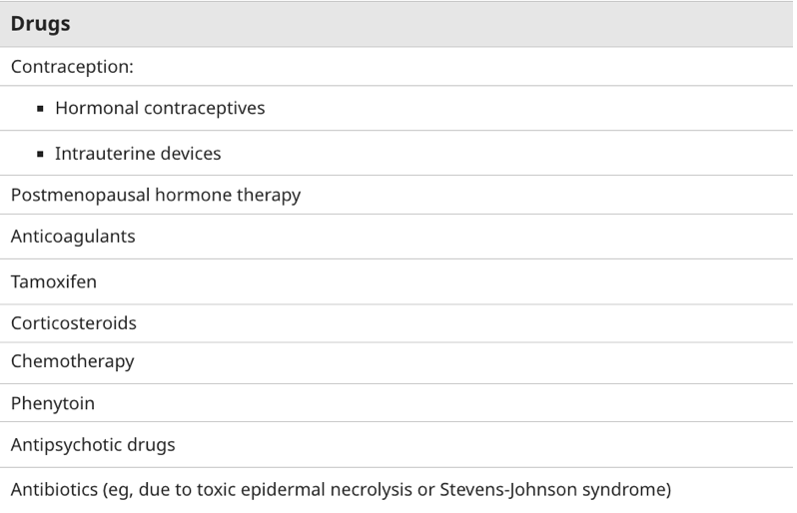
The FIGO classification for AUB can be divided into Structural and Non-structural causes. https://sso.uptodate.com/contents/abnormal-uterine-bleeding-in-nonpregnant-reproductive-age-patients-terminology-evaluation-and-approach-to-diagnosis?search=abnormal%20uterine%20bleeding&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 Structural: PALM (Polyp, Adenomyosis, Leiomyoma, Malignancy) Non-structural: COEIN (Coagulopathy, Ovulatory dysfunction, Endometrial, Iatrogenic, Not yet classified) It is important to look patient’s medication list as multiple medications can be the cause of AUB. This can include anticoagulants, corticosteroids and multiple psychiatric medications. https://sso.uptodate.com/contents/abnormal-uterine-bleeding-in-nonpregnant-reproductive-age-patients-terminology-evaluation-and-approach-to-diagnosis?search=abnormal%20uterine%20bleeding&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1Etiology
History Physical ExamClinical Approach
Investigations
Imaging
Unless bleeding is heavy and ongoing or associated with pain concerning for emergent diagnoses such as ectopic pregnancy, ovarian torsion etc., imaging is not typically necessary in the ED.
Laboratory Investigations
The SOGC recommends universally obtaining a CBC and excluding pregnancy.
The SOGC reports that there is “minimal evidence for ordering ferritin in the absence of anemia or microcytosis”[1]. That being said, ordering ferritin studies after a CBC returns may prolong the length of stay in your patients. With patients waiting a year or longer at times to see a women’s health trained family physician or gynecologist, I recommend ferritin up front in all patients presenting with heavy menstrual bleeding.
This recommendation was informed by an excellent 2025 CMAJ review [6]. It’s a comprehensive synthesis of the current evidence on iron deficiency, drawing from RCTs, observational studies, and both systematic and scoping reviews.
There are 2 key points to highlight:
- Iron deficiency, even without anemia, is clinically significant.
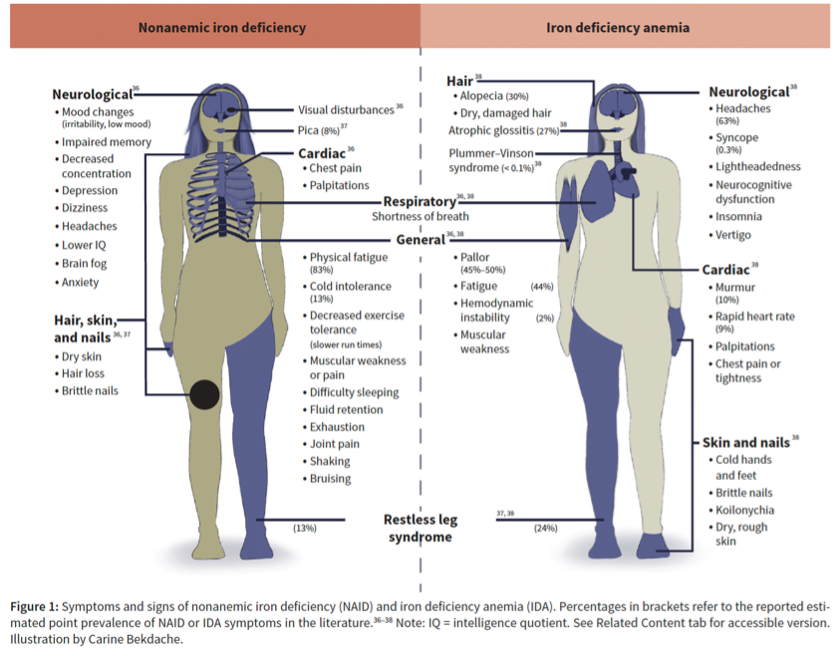
Iron is rate-limiting for red cell production, but it also plays a crucial role in myoglobin, cytochrome P450, and central nervous system function. This figure illustrates the wide spectrum of symptoms, many of which are subtle and often underrecognized. Non-anemic iron deficiency (NAID) is associated with chronic fatigue, impaired cognition, reduced work performance, and overall poorer quality of life.
- The patients at greatest risk are those with abnormal uterine bleeding (AUB) and those who are pregnant.
In a 2022 Ontario screening study, 38% of non-pregnant premenopausal females had NAID and 13% had IDA. Rates were even higher in pregnancy, with over half being iron deficient [6].
Sholzberg M, Hillis C, Crowther M, Selby R. Diagnosis and management of iron deficiency in females. CMAJ. 2025 Jul 2;197(24):E680–7. https://www.cmaj.ca/content/197/24/E680
The burden is particularly striking in patients with AUB. Iron deficiency is found to be 4–7 times more common in Black females compared to White females which may be in part due to higher rates of AUB in this population, reflecting yet another health inequity—iron deficiency is underrecognized, undertreated, stigmatized, and disproportionately affects individuals of Colour [6].
Thrombosis Canada’s 2025 guidelines agreed with this recommendation, stating: “All women who report symptoms of HMB or ID should have CBC and ferritin level assessed and treatment with oral or intravenous iron should be administered if there is iron deficiency with or without anemia”[14]
There’s some variation in the literature about other routine testing, but the consensus is:
- TSH does not need to be ordered in patients with regular but heavy menses and no other thyroid symptoms. If there is irregular or prolonged bleeding—or based on clinical suspicion—it’s reasonable to order, but there are no firm guidelines.
- Coagulation studies do not need to be done routinely unless there are red flags for a bleeding disorder: family history, AUB with heavy bleeding since menarche, or bleeding from other sites. Normal coagulations do not exclude bleeding disorders so these patients should still be referred if there is high suspicion
- Hormone studies (serum gonadotropins, estradiol, progesterone levels) should not be ordered in the ED.
Singh S, Best C, Dunn S, Leyland N, Wolfman WL. No. 292-Abnormal Uterine Bleeding in Pre-Menopausal Women. Journal of Obstetrics and Gynaecology Canada. 2018 May 1;40(5):e391–415. https://pubmed.ncbi.nlm.nih.gov/29731212/
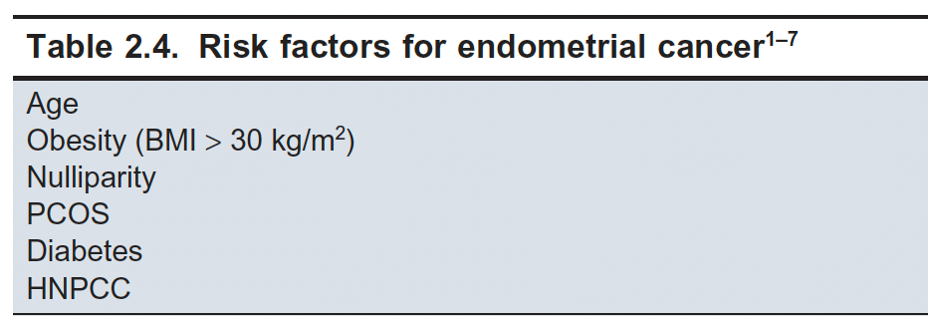
An important point to be aware of is that there is a misconception that a biopsy/further investigations are only needed in post-menopausal patients with vaginal bleeding. In reality, 5-30% of cases of endometrial cancer are diagnosed in pre-menopausal patients [1]. An endometrial biopsy should be considered in patients over 40 years old with risk factors for endometrial cancer according to Canadian guidelines.
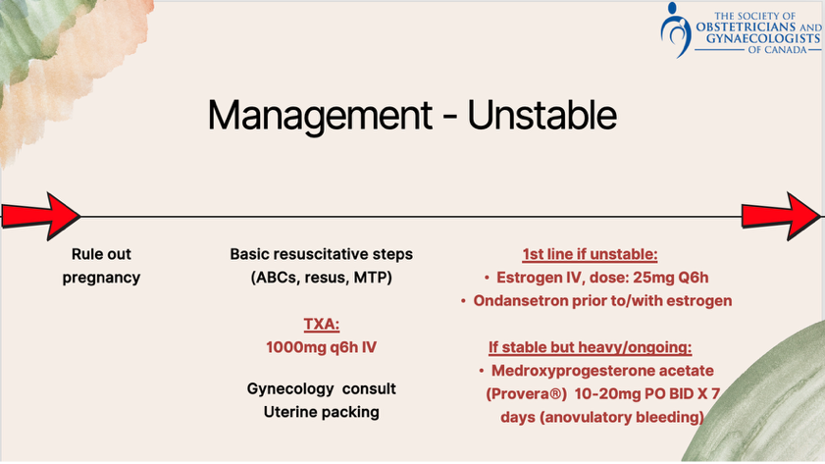
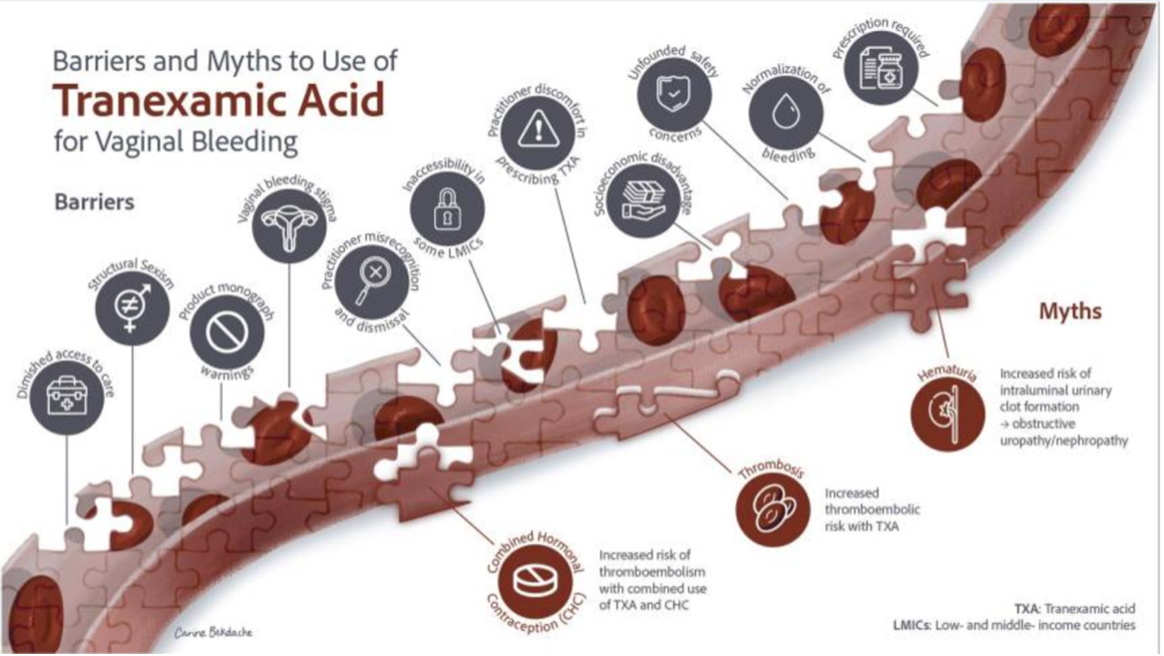
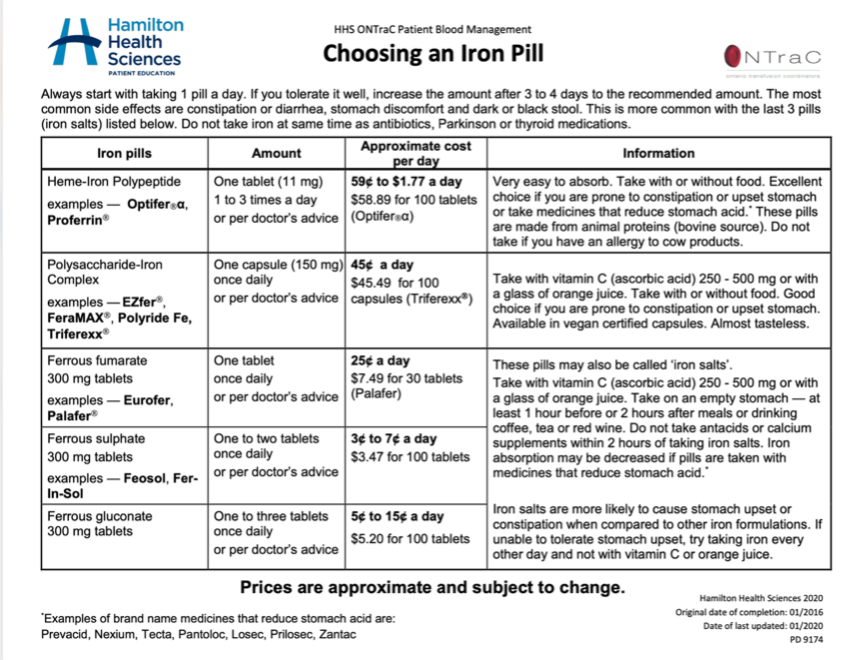
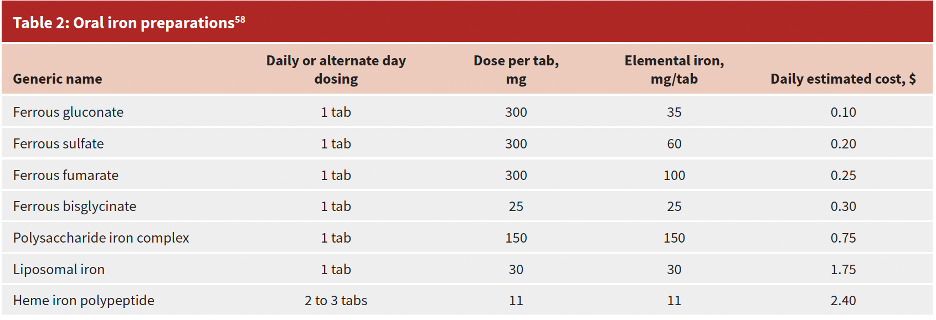
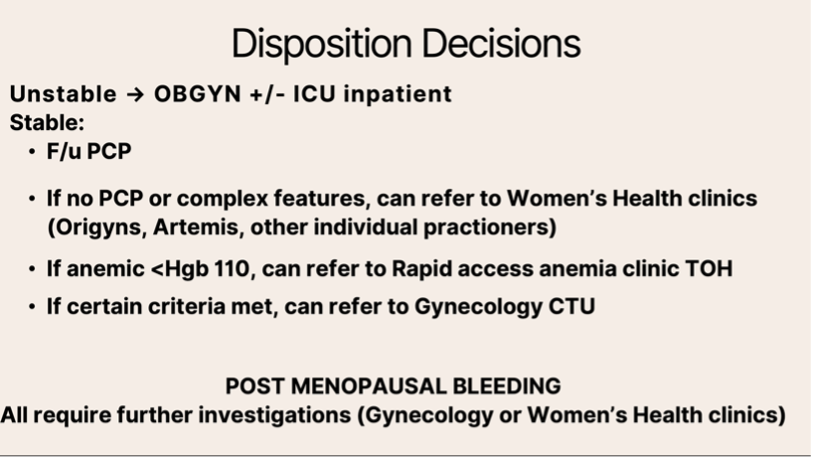
While unstable vaginal bleeding is not the focus of this blogpost, the general approach recommended would be as follows: Unstable: Stable but heavy/ongoing bleeding: It is essential to rule out pregnancy associated bleeding and then proceed with early resuscitative steps that are similar to other unstable bleeding cases. TXA can also be used, with variable dosage recommendations. The SOGC recommends 1000mg IV or PO Q6h. True unstable vaginal bleeding is quite rare in the non-pregnant individual however the first line treatment would be high dose IV estrogen, in discussion with Gynecology. It should be administered after an antiemetic if possible as estrogen causes high rates of nausea and vomiting. Typical contraindications to estrogen apply. If a patient is generally stable however having ongoing heavy bleeding that is thought to be anovulatory in nature (ex. PCOS), an alternative to estrogen is medroxyprogesterone. Stable: Non-hormonal Treatment Options NSAIDS Often our first-line treatment. They work by inhibiting cyclo-oxygenase activity, reducing prostaglandin synthesis, and promoting uterine vasoconstriction. A systematic review and meta-analysis of 17 RCTs by Lethaby et al. found that NSAIDs reduced menstrual blood loss by 30–50% compared to placebo, without an increase in adverse effects [7]. NSAIDS have the added benefit of improving dysmenorrhea which is not the case for treatments like TXA. NSAIDs should ideally be started the night before menses and continued throughout menstruation. They have been studied at regular dosing (not PRN) and at high doses for the indication of HMB. Most studies have looked at naproxen and mefenamic acid, though ibuprofen and ASA are also effective. My recommendation would be to use naproxen since it is the most studied for this indication and is also covered by ODB (Ontario Drug Benefit). I typically prescribe 500 mg BID, which costs about $0.25 per tablet—so roughly $3–4 per menstrual cycle. The usual contraindications for NSAIDS apply such as allergy, renal failure, peptic ulcer disease and more. One additional caution here in this context: avoid NSAIDs in patients with known or suspected bleeding disorders. Heavy menstrual bleeding may be a prominent symptom for many people with an underlying bleeding disorder, and these are often missed. While the ED may not be where these conditions are diagnosed, it is just a reminder to take a careful history. TXA Used for both stable and unstable patients with heavy menstrual bleeding, in either PO or IV form. Sholzberg M, Hillis C, Crowther M, Selby R. Diagnosis and management of iron deficiency in females. CMAJ. 2025 Jul 2;197(24):E680–7. https://www.cmaj.ca/content/197/24/E680 A comprehensive review by Vandermeulen et al. evaluated TXA in heavy menstrual bleeding and barriers to its use [9]. This Canadian review presented strong evidence from multiple systematic reviews and meta-analyses of RCTs, consistently showing TXA’s effectiveness [10,11]. Oral TXA reduces menstrual blood loss by 40–50% when taken TID during the heaviest days of the cycle [9]. What is especially compelling in the review by Vandermeulen et al. is the emphasis on systemic barriers to TXA use. These barriers are not rooted in evidence, but in structural and societal inequities, often relating to stigma around vaginal bleeding, and the normalization of HMB and IDA [9]. The most common concern raised about TXA is the fear of thromboembolic events. But despite this theoretical risk, large meta-analyses have shown no increase in arterial or venous thrombosis [12, 13]. Regarding patients with a history of VTE or those who are anticoagulated, Thrombosis Canada has updated their guidelines on the management of HMB in 2025 and it addresses this directly: “Clinicians are often hesitant to use TXA in patients on anticoagulation due to a perceived risk of inducing thrombosis. Randomized trials in high-risk populations, including postpartum, trauma, and perioperative settings, have not demonstrated an increased incidence of thrombotic events with TXA use. Although prospective studies evaluating TXA for the management of HMB in anticoagulated patients are lacking, thrombosis expert consensus support its temporary use in patients with HMB. Antifibrinolytics should generally be avoided at the beginning of VTE treatment, typically the first month, to allow for adequate fibrinolysis of the index thrombus [14]”. And our local experts agree. Dr. Roy Khalife (Benign Hematology) emphasized that he is comfortable prescribing TXA in anticoagulated patients. While he is more cautious in those who are strongly hypercoagulable, he noted that in short-term use for HMB, where the hemostatic balance is already tipped toward bleeding, TXA remains a reasonable choice. A second concern is the co-prescription of TXA and combined OCP. While prospective studies are lacking, there is no evidence showing an increased risk of thrombosis in combined OCP+TXA. We do recognize the increased risk of thrombosis in those on combined OCP at baseline. While prospective studies are lacking, there is evidence that may suggest safety. In prospective studies evaluating TXA in post-partum hemorrhage, there was no increased risk of thrombosis in this population. Given the pregnant individual’s estrogen levels are significantly higher than it would be in a patient on combined OCP, this is a reassuring finding for safety. Tips for prescribing TXA Hormonal Treatment Options The two options that we are most likely to prescribe from the emergency department are the combined oral contraceptive pill or the progesterone only pill. You can refer patients who are wanting to discuss contraception with their primary care provider, or who are unsure about which option is best for them to the SOGC website Sex&U. Combined OCP Combined OCP contain estrogen and progesterone. In a patient desiring contraception, starting an OCP can be very helpful for managing AUB and is a first line treatment. You must ensure your patient does not have any contraindications. Contraindications include but are not limited to the following: It can be very helpful to prescribe 2-3 months of OCP and have the patient follow up with a family physician afterwards. Progesterone Only Pill Cyclic progestin can be used in acute heavy menstrual bleeding in a stable patient. Progesterone-only birth controls can be considered in patients desiring contraception who have contraindications to estrogen. A common option to consider is drospirenone. IUD/surgical procedures The other first line treatment for AUB are progestin containing IUDs. While there can be some irregular spotting initially, control of heavy bleeding overtime is excellent and it is a highly effective contraceptive method. Other procedural treatments include the spectrum from ablation, or myomectomy, to hysterectomy but will often be second, third and fourth line options. Iron While iron won’t impact bleeding itself, it is an important part of management in these patients who are often iron deficient and anemic. As highlighted in the CMAJ review, we now know just how symptomatic iron deficiency even without anemia can be [6]. https://www.hamiltonhealthsciences.ca/wp-content/uploads/2019/08/Choosing-an-Iron-Pill.pdf The best PO iron supplement will be the one your patient will take consistently. The first line option remains iron salts (ferrous gluconate or ferrous sulfate) as they are less expensive than polysaccharide, heme-based or liposomal iron preparations and there is no evidence that more expensive counterparts are more effective. Sholzberg M, Hillis C, Crowther M, Selby R. Diagnosis and management of iron deficiency in females. CMAJ. 2025 Jul 2;197(24):E680–7. https://www.cmaj.ca/content/197/24/E680 Some iron products are covered by ODB while others are not. Resources to verify cost of medications in Ontario include: “Hamilton health Sciences: Choosing an Iron pill” and the CMAJ review referenced above. Treatment is often prolonged and this is another way we can help with inequity associated with this condition. There is weak evidence from several trials that showed that every-other-day therapy may be better tolerated compared to daily therapy, recognizing that intermittent dosing may reduce compliance [6]. Consider IV iron if: Administering IV iron is resource intensive and is not a viable option for most patients who are not anemic. That being said, it’s worth noting that there is RCT evidence that a 1-time dose of IV iron compared with 6 weeks of PO iron resulted in statistically higher rates of anemia correction (73% vs 50%) and significant hemoglobin increases (82% vs 62%). Disposition locally at TOH Management

References:
Authors
![]()
![]()