
Migraine is among the most common presentations to emergency departments (EDs), yet its management remains highly variable. Despite strong evidence supporting specific parenteral therapies, ineffective treatments persist while high-value procedural options remain underused.
The management of acute migraine in the ED has been guided for nearly a decade by the prior American Headache Society (AHS) evidence-based guideline in 2016 [1], and the Canadian Headache Society (CHS) guideline in 2015 [2]. The state of migraine care in the emergency department until recently has been summarized in a recent review that integrates the AHS and CHS guidelines [3]. Since that time, the landscape of acute migraine care has evolved substantially. New randomized controlled trials have been published, peripheral nerve blocks have been increasingly studied in ED populations, and novel therapeutic classes—notably calcitonin gene–related peptide (CGRP) antagonists—have emerged.
The 2025 AHS Guideline Update on Acute Treatment of Migraine in the Emergency Department [4]was developed to address these gaps. Building on the prior guideline, this update incorporates newly published evidence, and, for the first time, integrates peripheral nerve blocks alongside pharmacologic treatments.
This post reviews how the guideline was developed, presents the results structured by recommendation tier, and elaborates on two areas of high relevance to emergency physicians: dopamine antagonists, and greater occipital nerve blocks (GONB).
Why These Guidelines Matter
The 2025 AHS guideline is the first international guideline to:
- Harmonize parenteral medications and nerve blocks within a single ED treatment framework
- Formally evaluate parenteral CGRP antagonists regarding their possible use in the ED setting
Methods
The guideline was developed by a multidisciplinary panel that consisted of four neurologists, and two emergency physicians with a headache-focused practice or research program. Half of the panel was Canadian and half American.
Scope
- Adults presenting to the ED with migraine (any ICHD version)
- Parenteral therapies only (injectable medications and nerve blocks)
- Randomized controlled trials reporting outcomes within 6 hours
- Comparators: placebo, sham, or another parenteral therapy
- Studies included in the 2016 AHS guideline were excluded
Evidence Review
A systematic review was registered with PROSPERO, approved by the AHS Guideline Committee, and PRISMA guidelines were followed. A search was performed across MEDLINE, Embase, Cochrane, ClinicalTrials.gov, and the WHO International Clinical Trials Registry. Two authors screened the studies, and data were extracted to a standardized worksheet. Risk of bias was assessed using American Academy of Neurology (AAN) criteria.
The recommendations were formulated using the AAN guideline process, which involves evaluation the number of supporting studies, the class/quality of the studies (i.e., class I, class II, class III, or class IV), the effect size or magnitude of benefit, the consistency of the results, and adverse events.
A planned meta-analysis was not possible since no intervention had at least 2 studies meeting pre-specified criteria for pooling.
Results

Twenty-six randomized controlled trials met inclusion criteria:
- 13 Class I
- 8 Class II
- 5 Class III
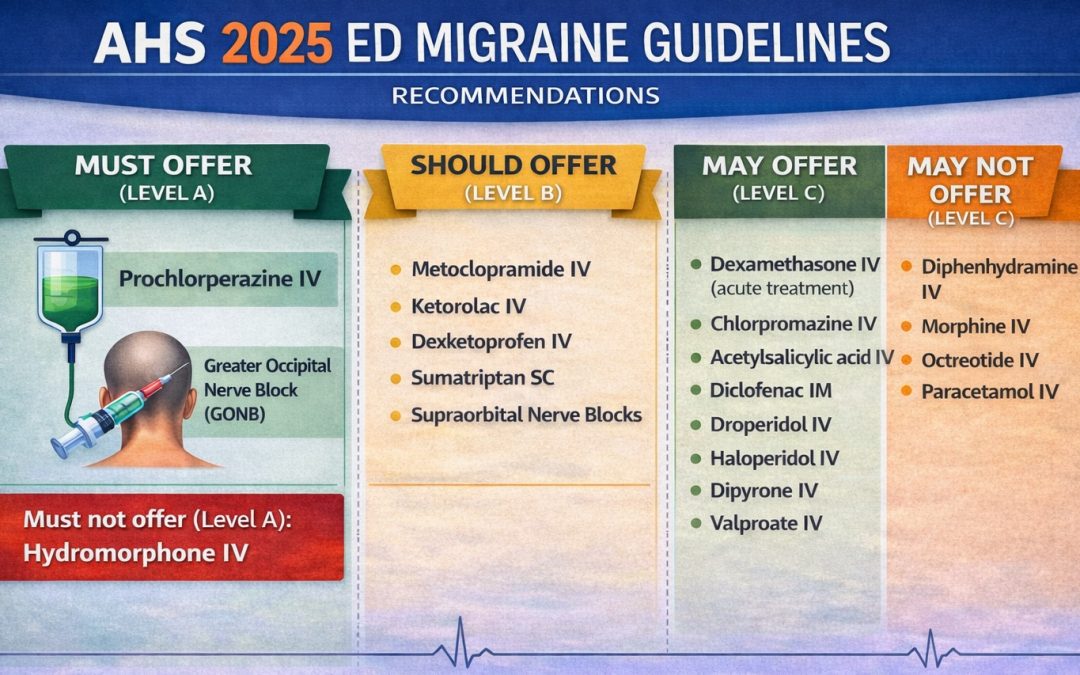
Recommendation Tiers
Level A — Must Offer
- Prochlorperazine IV
- Greater occipital nerve block (GONB)
Level A — Must NOT Offer
- Hydromorphone IV
Level B — Should Offer
- Metoclopramide IV
- Ketorolac IV
- Dexketoprofen IV
- Sumatriptan SC
- Supraorbital nerve blocks
Level C — May Offer
- Dexamethasone IV (acute treatment)
- Chlorpromazine IV
- Acetylsalicylic acid IV
- Diclofenac IM
- Droperidol IV
- Haloperidol IV
- Dipyrone IV
- Valproate IV
Level C — May NOT Offer
- Diphenhydramine IV
- Morphine IV
- Octreotide IV
- Paracetamol IV
Dopamine Antagonists: Prochlorperazine vs Metoclopramide
Dopamine antagonists remain foundational in ED migraine care. A key finding of the 2025 AHS guideline is that prochlorperazine was upgraded from “should offer” to “must offer”, while metoclopramide retains a “should offer” recommendation. The 2025 AHS guideline distinguishes these agents based on consistency and quality of evidence, not clinical familiarity. Metoclopramide is supported by a broader but more heterogeneous evidence base, while prochlorperazine demonstrates more consistent benefit across high-quality comparative trials.
| Question | Metoclopramide | Prochlorperazine |
|---|---|---|
| How strong is the evidence overall? | Many studies, but variable designs and inconsistent results | Fewer studies, but more consistent, higher-quality evidence |
| Head-to-head or active comparator performance | Often similar to other agents, sometimes underperforms | Comparable to other effective agents; strong comparative performance |
| Placebo-controlled clarity | Mixed signal, including at least one Class I study that did not meet its primary endpoint | Clearer, more reproducible benefit across trials |
| 2025 AHS guideline conclusion | Level B — Should Offer | Level A — Must Offer |
(For a more indepth analysis of the evidence, read the 2025 guideline).
Practical takeaway: Use prochlorperazine first-line when available. Offer metoclopramide if prochlorperazine is unavailable.
Greater Occipital Nerve Blocks (GONB)
One of the most practice-changing aspects of the 2025 guideline is the inclusion of nerve blocks alongside other parenteral treatments and the recommendation of greater occipital nerve blocks (GONB) of Level A – Must Offer.
This recommendation is supported by three Class I randomized controlled trials and one Class II randomized controlled trial, all conducted in acute-care or ED populations and included in the guideline.
| Study | Comparator | Result |
|---|---|---|
| Friedman 2018 | Sham | Superior |
| Friedman 2020 | Metoclopramide IV | Inferior overall, comparable among experienced injectors |
| Hokenek 2021 | Sham | Superior |
| Korucu 2018 | Dexketoprofen + metoclopramide vs sham | Superior |
Based on three positive Class I studies (including two sham-controlled trials) and supportive Class II evidence, GONB received a Level A – Must Offer recommendation.
With regards to the other cranio-facial nerve blocks, the following studies met the inclusion criteria:
- Superior orbital nerve blocks (SONB) were evaluated in 1 Class I study SONB were superior to sham, however more efficacious when combined with GONB [25]
- Sphenopalatine blocks (SPG) were evaluated in 1 Class II study in the outpatient setting using the TX360 © apparatus showing superiority to sham at 30 minutes [26]. A Class III study of intranasal lidocaine + metoclopramide showed no difference compared with placebo + metoclopramide at 30 minutes [27]. Studies of SPG blocks were heterogenous across a multitude of settings and headache disorders, often with lack of clarity as to whether the SPG was truly blocked or simply intranasal lidocaine anesthetizing the maxillary nerve.
- No eligible studies of the auricotemporal nerve met inclusion criteria.
Dexamethasone (Acute Treatment)
- Dexamethasone is well established in reducing headache relapse after ED discharge
- Evidence for acute benefit is mixed:
- Class I trial (Karimi et al. 2017) [28]:
- Comparable efficacy to sodium valproate 400 mg IV
- Class II trial (Mazaheri et al. 2015) [29]:
- Comparable efficacy to sodium valproate 400 mg IV
- Class III trial (Khazaei et al.) [30]:
- Comparable efficacy to chlorpromazine, ketorolac, and metoclopramide
- Class I trial (Karimi et al. 2017) [28]:
- Previously, the 2016 AHS guideline found 1 Class II study reported comparable efficacy to morphine, and Class III studies reporting comparable efficacy to valproic acid and inferiority to propofol [1].
- Based on this, dexamethasone received a Level C – May Offer recommendation for acute migraine treatment, distinct from its established role in preventing headache recurrence.
Parenteral CGRP Monoclonal Antibodies: Why Eptinezumab Was Evaluated
The 2025 AHS guideline is the first ED-focused migraine guideline to formally evaluate a parenteral CGRP antagonist. Four parenteral CGRP antagonists are approved of migraine prevention: erenumab SC, fremanezumab SC, galcanezumab SC, and eptinezumab IV. Given that eptinezumab is administered intravenously, an RCT was conducted to evaluate whether it is effective at acutely treating a migraine attack [31].
In total, 480 patients were enrolled and randomized to either receiving eptinezumab IV or placebo within hours of a migraine attack onset. Eptinezumab was superior to placebo achieving 2-hour headache freedom in 23.5% compared with 12.0% of those receiving placebo.
The trial, however, was conducted primarily in the outpatient setting. Ultimately, as a result, no recommendation was given to eptinezumab in the ED pending future ED-specific studies.
Practical Take-Home Points
- Prochlorperazine IV and GONB are must-offer therapies
- Metoclopramide remains appropriate when prochlorperazine is unavailable
- Dexamethasone may be used for acute treatment, beyond recurrence prevention
- Opioids should be avoided
References
Orr SL, Friedman BW, Christie S, et al. Management of Adults with Acute Migraine in the Emergency Department: The American Headache Society Evidence Assessment of Parenteral Pharmacotherapies. Headache. 2016;56(6):911-940. doi:10.1111/HEAD.12835;REQUESTEDJOURNAL:JOURNAL:15264610;ISSUE:ISSUE:DOI
- Orr SL, Aubé M, Becker WJ, et al. Canadian Headache Society systematic review and recommendations on the treatment of migraine pain in emergency settings. Cephalalgia. 2015;35(3):271-284. doi:10.1177/0333102414535997
- Cortel-LeBlanc MA, Orr SL, Dunn M, James D, Cortel-LeBlanc A. Managing and Preventing Migraine in the Emergency Department: A Review. Ann Emerg Med. 2023;82(6):732-751. doi:10.1016/j.annemergmed.2023.05.024
- Robblee J, Minen MT, Friedman BW, Cortel-LeBlanc MA, Cortel-LeBlanc A, Orr SL. 2025 guideline update to acute treatment of migraine for adults in the emergency department: The American Headache Society evidence assessment of parenteral pharmacotherapies. Headache: The Journal of Head and Face Pain. 2025;00(11):16. doi:10.1111/HEAD.70016
- Doğan NÖ, Pekdemir M, Yılmaz S, et al. Intravenous metoclopramide in the treatment of acute migraines: A randomized, placebo-controlled trial. Acta Neurol Scand. 2019;139(4):334-339. doi:10.1111/ANE.13063;REQUESTEDJOURNAL:JOURNAL:16000404;PAGE:STRING:ARTICLE/CHAPTER
- Yavuz E, Gulacti U, Lok U, Turgut K. Intravenous metoclopramide versus dexketoprofen trometamol versus metoclopramide+ dexketoprofen trometamol in acute migraine attack in the emergency department: A randomized double-blind controlled trial. Am J Emerg Med. 2020;38(11):2254-2258. doi:10.1016/J.AJEM.2020.04.038
- Friedman BW, Irizarry E, Williams A, et al. A Randomized, Double-Dummy, Emergency Department-Based Study of Greater Occipital Nerve Block With Bupivacaine vs Intravenous Metoclopramide for Treatment of Migraine. Headache. 2020;60(10):2380-2388. doi:10.1111/HEAD.13961;CTYPE:STRING:JOURNAL
- Hodgson SE, Harding AM, Bourke EM, Taylor DM, Greene SL. A prospective, randomized, double-blind trial of intravenous chlorpromazine versus intravenous prochlorperazine for the treatment of acute migraine in adults presenting to the emergency department. Headache. 2021;61(4):603-611. doi:10.1111/HEAD.14091;PAGE:STRING:ARTICLE/CHAPTER
- Friedman BW, Irizarry E, Solorzano C, et al. Randomized study of IV prochlorperazine plus diphenhydramine vs IV hydromorphone for migraine. Neurology. 2017;89(20):2075-2082. doi:10.1212/WNL.0000000000004642;REQUESTEDJOURNAL:JOURNAL:WNL;JOURNAL:JOURNAL:WNL;WGROUP:STRING:PUBLICATION
- Korucu O, Dagar S, Çorbacioglu K, Emektar E, Cevik Y. The effectiveness of greater occipital nerve blockade in treating acute migraine-related headaches in emergency departments. Acta Neurol Scand. 2018;138(3):212-218. doi:10.1111/ANE.12952;WGROUP:STRING:PUBLICATION
- Abiri S, Chegin M, Soleimani R, Hatami N, Kalani N, Rayatdoost E. Propofol + Granisetron vs. Propofol + Metoclopramide in Symptom Management of Acute Migraine Headache; a Double-Blind Randomized Clinical Trial. Arch Acad Emerg Med. 2022;10(1):e19-e19. doi:10.22037/AAEM.V10I1.1561
- Khazaei M, Hosseini Nejad Mir N, Yadranji Aghdam F, Taheri M, Ghafouri-Fard S. Effectiveness of intravenous dexamethasone, metoclopramide, ketorolac, and chlorpromazine for pain relief and prevention of recurrence in the migraine headache: a prospective double-blind randomized clinical trial. Neurological Sciences 2019 40:5. 2019;40(5):1029-1033. doi:10.1007/S10072-019-03766-X
- Gaffigan ME, Bruner DI, Wason C, Pritchard A, Frumkin K. A Randomized Controlled Trial of Intravenous Haloperidol vs. Intravenous Metoclopramide for Acute Migraine Therapy in the Emergency Department. Journal of Emergency Medicine. 2014;49(3):326-334. doi:10.1016/j.jemermed.2015.03.023
- Friedman BW, Garber L, Yoon A, et al. Randomized trial of IV valproate vs metoclopramide vs ketorolac for acute migraine. Neurology. 2014;82(11):976-983. doi:10.1212/WNL.0000000000000223
- Friedman BW, Corbo J, Lipton RB, et al. A trial of metoclopramide vs sumatriptan for the emergency department treatment of migraines. Neurology. 2005;64(3):463-468. doi:10.1212/01.WNL.0000150904.28131.DD
- Fernandes Filho SMM, Costa MS, Fernandes MT, Foerster MV. Comparação de dipirona intravenosa com metoclopramida intravenosa no tratamento de crise aguda de enxaqueca: ensaio clínico randomizado. Arq Neuropsiquiatr. 2006;64(4):1005-1008. doi:10.1590/S0004-282X2006000600023
- Cameron JD, Lane PL, Speechley M. Intravenous Chlorpromazine vs Intravenous Metoclopramide in Acute Migraine Headache. Academic Emergency Medicine. 1995;2(7):597-602. doi:10.1111/J.1553-2712.1995.TB03596.X;CTYPE:STRING:JOURNAL
- Cete Y, Dora B, Ertan C, Ozdemir C, Oktay C. A randomized prospective placebo-controlled study of intravenous magnesium sulphate vs. metoclopramide in the management of acute migraine attacks in the Emergency Department. Cephalalgia. 2005;25(3):199-204. doi:10.1111/J.1468-2982.2004.00840.X;SUBPAGE:STRING:ABSTRACT;WEBSITE:WEBSITE:PERICLES;JOURNAL:JOURNAL:14682982;REQUESTEDJOURNAL:JOURNAL:14682982;WGROUP:STRING:PUBLICATION
- Funato Y, Kimura A, Matsuda W, Uemura T, Kobayashi K, Sasaki R. Pain relief effect of metoclopramide vs. sumatriptan for acute migraine attack: A single-center, open-label, cluster-randomized controlled non-inferiority trial. GHM open. 2024;4(2):95-98. doi:10.35772/ghmo.2023.01026
- Cameron JD, Lane PL, Speechley M. Intravenous Chlorpromazine vs Intravenous Metoclopramide in Acute Migraine Headache. Academic Emergency Medicine. 1995;2(7):597-602. doi:10.1111/J.1553-2712.1995.TB03596.X;CTYPE:STRING:JOURNAL
- Friedman BW, Esses D, Solorzano C, et al. A Randomized Controlled Trial of Prochlorperazine Versus Metoclopramide for Treatment of Acute Migraine. Ann Emerg Med. 2008;52(4):399-406. doi:10.1016/j.annemergmed.2007.09.027
- Miller MA, Levsky ME, Enslow W, Rosin A. Randomized evaluation of octreotide vs prochlorperazine for ED treatment of migraine headache. Am J Emerg Med. 2009;27(2):160-164. doi:10.1016/J.AJEM.2008.01.015
- Tanen DA, Miller S, French T, Riffenburgh RH. Intravenous sodium valproate versus prochlorperazine for the emergency department treatment of acute migraine headaches: A prospective, randomized, double-blind trial. Ann Emerg Med. 2003;41(6):847-853. doi:10.1067/mem.2003.195
- Friedman BW, Mohamed S, Robbins MS, et al. A Randomized, Sham-Controlled Trial of Bilateral Greater Occipital Nerve Blocks With Bupivacaine for Acute Migraine Patients Refractory to Standard Emergency Department Treatment With Metoclopramide. Headache. 2018;58(9):1427-1434. doi:10.1111/HEAD.13395;JOURNAL:JOURNAL:15264610;WGROUP:STRING:PUBLICATION
- Hokenek NM, Ozer D, Yılmaz E, et al. Comparison of greater occipital nerve and supra orbital nerve blocks methods in the treatment of acute migraine attack: A randomized double-blind controlled trial. Clin Neurol Neurosurg. 2021;207:106821. doi:10.1016/J.CLINEURO.2021.106821
- Cady R, Saper J, Dexter K, Manley HR. A double-blind, placebo-controlled study of repetitive transnasal sphenopalatine ganglion blockade with Tx360® as acute treatment for chronic migraine. Headache. 2015;55(1):101-116. doi:10.1111/HEAD.12458;ISSUE:ISSUE:DOI
- Avcu N, Doğan NÖ, Pekdemir M, et al. Intranasal Lidocaine in Acute Treatment of Migraine: A Randomized Controlled Trial. Ann Emerg Med. 2017;69(6):743-751. doi:10.1016/j.annemergmed.2016.09.031
- Karimi N, Tavakoli M, Charati JY, Shamsizade M. Single-dose intravenous sodium valproate (Depakine) versus dexamethasone for the treatment of acute migraine headache: a double-blind randomized clinical trial. Clin Exp Emerg Med. 2017;4(3):138-145. doi:10.15441/CEEM.16.199
- Mazaheri S, Poorolajal J, Hosseinzadeh A, Fazlian MM. Effect of Intravenous Sodium Valproate vs Dexamethasone on Acute Migraine Headache: A Double Blind Randomized Clinical Trial. PLoS One. 2015;10(3):e0120229. doi:10.1371/JOURNAL.PONE.0120229
- Khazaei M, Hosseini Nejad Mir N, Yadranji Aghdam F, Taheri M, Ghafouri-Fard S. Effectiveness of intravenous dexamethasone, metoclopramide, ketorolac, and chlorpromazine for pain relief and prevention of recurrence in the migraine headache: a prospective double-blind randomized clinical trial. Neurological Sciences 2019 40:5. 2019;40(5):1029-1033. doi:10.1007/S10072-019-03766-X
- Winner PK, McAllister P, Chakhava G, et al. Effects of Intravenous Eptinezumab vs Placebo on Headache Pain and Most Bothersome Symptom When Initiated During a Migraine Attack: A Randomized Clinical Trial. JAMA. 2021;325(23):2348-2356. doi:10.1001/JAMA.2021.7665

We interviewed two of the authors of the AHS guidelines on the Skeptics’ Guide to EM. https://thesgem.com/2026/01/sgem-xtra-hit-me-with-your-best-block-2025-ahs-ed-migraine-guidelines/
What about prochloperazine IM ? Any evidence of its efficacy? Thank you
Dear Hasan,
There is a 1996 study showing IM prochlorperazine superior to metoclopramide. Aside from this, I haven’t seen any other studies.
DOI: 10.1016/S0735-6757(96)90171-0
Warm regards
Miguel