Smarter Starts and Safer Stops: Antibiotic Stewardship in the ED
by Mejbel Alazemi | Mar 12, 2026 |
Antimicrobial stewardship (AMS) is about using the right antibiotic, only when needed, and choosing the appropriate dose, route, and duration. The goal is to treat infections effectively while reducing harm, both to the individual and to the healthcare system. It’s not about withholding care. It’s about balancing benefit and risk, ensuring that antibiotics still work tomorrow by being smart with how we use them today.
We hear about this and conceptulize this idea constantly, but we aim to give you some more practical pearls with this point that you can take into your next patient encounter. In this post we’re going to focus on
- The myth of IV antibiotics being superior to PO antibiotics (spoiler: they’re not)
- 3 specific cases where antibiotic coverage can be better targetted
- Penicillin allergies myths, and how to challenge
- Asymptomatic bacteriuria, and the delirium workup
- And practical tips for helping our patients
In Canada, outpatient antibiotics cause over 280,000 ED visits and 26,000 hospital admissions each year due to adverse drug events, costing over $400 million annually.¹
Globally, 4.95 million deaths in 2019 were associated with drug-resistant infections.² In Canada, 26% of bacterial infections are resistant to at least one first-line antibiotic, contributing to 14,000 deaths annually.³
This isn’t just a looming threat, it’s already here. And antimicrobial stewardship is one of our strongest tools to fight it.
Antimicrobial resistance can undermine everything we do in healthcare. We can’t treat cancer if we can’t treat infections. We can’t do surgery if we can’t treat infections. We need antibiotics to work to support modern medicine.
Why Is Stewardship Still a Challenge?
If we know stewardship is important, why is it still an issue? Because changing physician behavior is hard, and the biggest predictor of how we practice is how we were taught. When we’re unsure, we often prescribe antibiotics “just in case.”
If we miss a serious infection, that can be directly pinned on us. But if we give someone C. difficile from unnecessary antibiotics, we’re unlikely to be blamed. No one says, “You caused this.” It’s often seen as just an unfortunate side effect.
So we end up ignoring potential harm to the patient in order to protect ourselves from the risk of missing something or facing a medicolegal consequence, and that’s just bad medicine.
That’s why it’s so important to pause and ask ourselves, and I love this question: are you treating the patient, or are you treating yourself? Especially when you’re thinking about giving an antibiotic “just in case.”
Antibiotic Use in the ED
Emergency Departments account for a large share of antibiotic prescriptions in Canada. Between 2012 and 2018, 66% of infection-related ED visits resulted in an antibiotic, nearly twice the rate seen in community clinics.⁴ Yes, we see sicker patients, but we also face diagnostic uncertainty, time pressure, and patient expectations, all of which push us toward “just in case” prescribing.
A national audit found that 1 in 5 ED antibiotic prescriptions were inappropriate.⁵ So which conditions were driving the numbers?
Antibiotics were used in 70% of ED visits for sinusitis, yet more than half of those patients didn’t need them. Seventy-five percent of dental complaints received antibiotics, when most simply needed dental care.⁶
We’ve come to accept this high rate of antibiotic use as normal. But it’s worth challenging that mindset. Imagine if we replaced the word “antibiotic” with “chemotherapy.” What if we said that 20% of chemotherapy was inappropriate, or that patients didn’t need it? There would be outrage.
Yet we tolerate this level of misuse with antibiotics every day. It’s part of our prescribing culture, defaulting to “just in case.”
The ED is a high-risk zone for overprescribing, but that also makes it a high-impact zone for stewardship. Every improved decision here has ripple effects.
The “Momentum” of ED Antibiotics
Part of the challenge is the diagnostic uncertainty and cognitive overload we face in the ED. So what happens? We err on the side of “broad-spectrum, just in case.”
But here’s the catch: ED antibiotics tend to stick. A U.S. study found that 75% of antibiotics started in the ED were continued after admission, often unchanged. And once broad-spectrum agents like pip-tazo are started, they’re rarely de-escalated.⁷
But does using a broad-spectrum antibiotic actually lead to better outcomes? Not really.
A Canadian study of sepsis found that over half of patients received antibiotics broader than necessary, yet outcomes were no better.⁸ Overtreating doesn’t help the patient, but it does fuel resistance. Emergency clinicians work in an environment where the temptation to over-treat is strong. By integrating antimicrobial stewardship into our practice, we can protect patients from avoidable complications and improve overall care.
The IV vs PO Myth
Let’s talk about the IV versus oral (PO) antibiotic myth, one of the most deeply ingrained ideas in emergency medicine.
There’s a common notion that IV antibiotics are faster, stronger, and more appropriate for “serious” infections. Many of us have been taught that more severe infections require IV therapy, and that starting with an IV dose and then switching to oral antibiotics somehow “kickstarts” treatment.
But is any of that actually true?
This is one of the most persistent misconceptions we face: IV equals stronger. For many infections, that simply isn’t the case.
Several antibiotics, including fluoroquinolones, Septra, doxycycline, and clindamycin, have excellent oral bioavailability. When given orally, they achieve serum concentrations equivalent to IV dosing.⁹
The clinical outcomes reflect this. A meta-analysis of seven studies involving more than 1,300 patients hospitalized with pneumonia found no difference in mortality between IV and oral therapy. Patients who received oral antibiotics actually had shorter hospital stays.¹⁰
That makes intuitive sense. If oral bioavailability weren’t good, why would we use oral antibiotics at all?
Earlier evidence tells the same story. A 2013 Cochrane review examining low-risk febrile neutropenia in cancer patients, covering more than 2,300 participants across 22 randomized controlled trials, found no difference in treatment failure or mortality between oral and IV regimens.¹¹
More recent data reinforces this. A 2023 meta-analysis of 12 randomized trials involving over 2,100 adults with pneumonia showed that oral antibiotics were not only equivalent but were actually associated with lower mortality.¹² Clinical cure rates and adverse events were similar, and hospital stays were shorter with oral therapy.
So when patients are stable, oral therapy doesn’t just match IV, it may actually be better.
And it’s not just pneumonia or febrile neutropenia. A 2023 review of 21 randomized trials across a range of infections reached the same conclusion: for stable patients, oral antibiotics are just as effective as IV therapy.¹³
These findings are echoed by Choosing Wisely Canada, which recommends against IV antibiotics when agents with excellent oral bioavailability are available.¹⁴ Oral therapy avoids the risks of venous access, is easier to administer, and often gets patients home faster. If the patient is stable and the gut works, use it. It’s just as effective, safer, and more efficient.
Take pyelonephritis as an example, a serious infection that many clinicians still default to IV treatment for. But the evidence doesn’t support that reflex. In adults with pyelonephritis or complicated urinary tract infections, oral fluoroquinolones are non-inferior to IV therapy. A Cochrane review of 15 randomized trials found no difference in cure rates between oral regimens and initial IV therapy, even in pediatric patients.¹⁵
Another common habit deserves scrutiny: giving an IV dose of antibiotics in the ED “just to get things started,” then discharging the patient on oral therapy. It sounds reasonable, but the data doesn’t support this as a routine practice. A 2016 systematic review of 27 studies involving more than 4,400 children with acute pyelonephritis found that oral antibiotics alone were just as effective as combined IV-to-oral regimens.¹⁶ Oral treatment also avoided IV-related complications and reduced costs. If a patient is stable enough to go home on oral therapy, they probably didn’t need an IV dose in the first place.
We’ve all had that moment: the patient doesn’t look better after 24 hours, and we start to wonder whether the antibiotic failed. But antibiotics don’t work instantly. They often take two to three days to produce meaningful clinical improvement. A lack of improvement on day one doesn’t mean failure, it’s often just the expected course of illness.
Before escalating to IV therapy, pause. Confirm adherence. Double-check the dose. And reassure the patient.

Our infectious diseases colleagues consistently emphasize that for agents like azithromycin and respiratory fluoroquinolones, oral therapy is highly effective. Historically, concerns focused on beta-lactams due to lower oral absorption. But emerging evidence shows that high-dose oral beta-lactams can successfully complete treatment, even for bacteremia, challenging the assumption that IV therapy is always necessary.
If you think your pneumonia patient is going home, or may only need a short admission, start with oral antibiotics. Internal Medicine is likely to continue whatever we initiate in the ED. By avoiding unnecessary switches and reflexively reaching for ceftriaxone and azithromycin, we can minimize harm to the patient’s gut, reduce antimicrobial resistance, and lower the risk of C. difficile infection.
For further in-depth reading, check out these great posts from First10EM and RebelEM on the topic.
Putting Stewardship Into Practice
Three common ED scenarios where AMS can change our approach:
Diverticulitis
For years, we treated all diverticulitis with antibiotics. But that has changed. New evidence and updated guidelines now support no antibiotics for uncomplicated diverticulitis in immunocompetent, clinically stable patients.¹⁷
Multiple studies have shown no difference in recovery time, complications, or recurrence when antibiotics are withheld, while significantly reducing adverse effects and unnecessary antibiotic exposure.¹⁷ ¹⁸ ¹⁹ This is low-hanging stewardship fruit.
The approach is simple: talk with the patient, share the evidence, and provide clear discharge instructions. This is a strong example of antimicrobial stewardship in action, safely reducing antibiotic use in a condition where antibiotics are unlikely to offer clinical benefit.
For a deeper dive on diverticulitis, read more here.
Sinusitis
Sinusitis is another major opportunity for antimicrobial stewardship. Most cases are viral and resolve without antibiotics, which means our most impactful interventions are often reassurance, education, and symptomatic management.
Despite clear guidelines, antibiotics are still prescribed in 50–70% of ED sinusitis encounters, and more than half of these prescriptions are not indicated.²⁰ Part of the challenge is uncertainty. When are antibiotics actually indicated?
Canadian guidelines and Choosing Wisely Canada recommend antibiotics only when symptoms persist for more than 7–10 days without improvement, or in cases with severe or worsening features.²¹
We can make a huge impact here by confidently not prescribing antibiotics when they are not needed.
Fever in Non-Neutropenic Cancer Patients
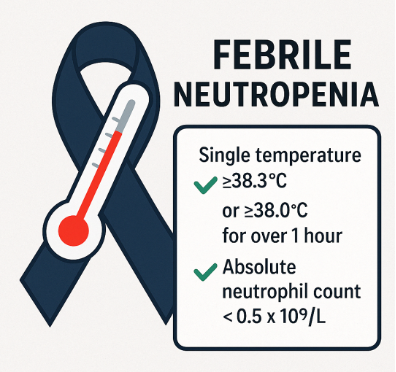
There is a lack of standardized guidelines for non-neutropenic fever in cancer patients. While febrile neutropenia is a true emergency, cancer patients with fever and a normal neutrophil count are common in the ED, and many are treated as if they are neutropenic.
If a patient is not neutropenic, they should generally be approached like any other febrile patient. Perform a full assessment, look for a source, and tailor management accordingly. If the presentation is viral or self-limited, supportive care may be sufficient.
Not every cancer patient with a fever needs piperacillin-tazobactam.
There is a natural tendency to be extra cautious with cancer patients, but caution does not always mean starting broad-spectrum IV antibiotics. Evidence suggests that most febrile cancer patients who are not neutropenic do not have life-threatening infections and often do not require aggressive treatment. In one review, 83% of non-neutropenic febrile cancer patients were admitted, yet nearly 25% were discharged within two days, and serious complications were rare.²² This suggests that many admissions, and the empiric IV antibiotics that come with them, may be avoidable with better risk stratification.
Observational studies show that withholding empiric antibiotics in stable, non-neutropenic patients is often safe, with no survival benefit to broad-spectrum antibiotic use. What does increase, however, are hospital length of stay and antibiotic exposure.²³
So how should we approach these patients? Start with risk assessment.
- Are they clinically well?
- Are labs reassuring?
- Is there a clear source, such as a viral upper respiratory infection or uncomplicated UTI?
If so, outpatient management may be appropriate, just as it would be for an immunocompetent patient.
That said, caution is still warranted. “Non-neutropenic” does not always mean “not immunosuppressed.” Some patients may be vulnerable due to steroids or targeted therapies. And not all fevers are infectious. Tumor-related fever and drug reactions should remain on the differential.
When in doubt, pick up the phone and collaborate with oncology colleagues.
Penicillin Allergies – Decoding the Label
“I’m allergic to penicillin.” We hear it every day in the ED, but it is rarely true.
About 10% of patients report a penicillin allergy, yet when these patients are formally tested, over 90% are not actually allergic.²⁴
Often, the story sounds familiar: “I had a rash as a baby.” “My mom told me I was allergic.”
Sometimes a viral rash was mistakenly blamed on antibiotics.nEven in patients who once had a true IgE-mediated reaction, about 80% lose sensitivity within 10 years. In other words, most penicillin allergy labels are outdated or inaccurate.²⁴
In the ED, we can start the process of de-labeling simply by asking a few more questions.
- What was the reaction?
- How long ago did it happen?
- Which antibiotic caused it?
When someone says, “I’m allergic to penicillin, I got a rash as a baby but I’m not really sure,” that history is almost certainly not a true allergy. For low-risk histories like this, Canadian allergists often recommend a direct oral amoxicillin challenge to definitively remove the label.
If you believe a penicillin is the best agent, for example in a cat bite, I encourage you to give a dose of amoxicillin-clavulanate, observe the patient for 30–60 minutes, and if there is no reaction, discharge them home and document that their penicillin allergy is unlikely to be real.
Why does this matter, and why is it relevant to antimicrobial stewardship? Patients labeled as penicillin-allergic are far more likely to receive broad-spectrum, second-line antibiotics. That increases antimicrobial resistance, side effects, and healthcare costs.
A JAMA study showed that patients with a penicillin allergy label had significantly higher rates of resistant infections, largely because they were prescribed alternative agents unnecessarily.²⁵
We have all heard the warning that there is “10% cross-reactivity” between penicillins and cephalosporins. But that number comes from flawed studies from the 1960s. Current evidence shows the risk is closer to 1%, and that cross-reactivity depends on the R1 side chain, not the beta-lactam ring itself.²⁶
Once we understand that cross-reactivity is driven by R1 side chains, the implications are clear.
Many cephalosporins have different side chains and are safe to use in patients with a reported penicillin allergy. Using a simple side-chain “cheat sheet” can help clarify which antibiotics truly overlap. For example, if a patient has a true allergy to amoxicillin, cephalexin (Keflex) is still a safe option. The risk of cross-reactivity is even lower with third- and fourth-generation cephalosporins.
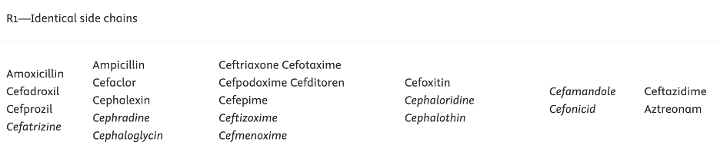
Identical R1 side chains. Cephalosporins with similar structures should be avoided in true allergy.
Table from: https://www.dropthelabel.ca/clinical-resources/table-for-cross-reactivity-for-patients-with-confirmed-or-suspected-antibiotic-allergy
We do not need to reach for broad-spectrum antibiotics at the first mention of “penicillin allergy.”
By clarifying the history and understanding the pharmacology, we can use safer, narrower agents and practice better antimicrobial stewardship.
Asymptomatic Bacteriuria
One of the most common antimicrobial stewardship challenges we face in the ED is asymptomatic bacteriuria (ASB). You have seen this scenario countless times:
- An older adult presents with weakness or confusion.
- A urinalysis is sent and comes back positive.
- The patient denies urinary symptoms.
- Yet most of these patients get started on antibiotics.
The problem is that bacteria in the urine does not equal infection. In many cases, especially in older adults, it represents benign colonization rather than a urinary tract infection.²⁷
The prevalence of asymptomatic bacteriuria is high:
- Up to 19% in community-dwelling older adults
- Up to 50% in long-term care residents
- Nearly 100% in individuals with long-term indwelling catheters
Multiple studies and randomized controlled trials have shown that treating ASB in non-pregnant adults does not improve outcomes and can actually cause harm by increasing antimicrobial resistance and adverse effects.²⁷ As uncomfortable as it can be, especially when families or care homes are pushing for antibiotics, this is where education matters.
A positive urine culture alone almost always reflects colonization, not infection. We need to treat patients, not lab results.
When Should We Even Send a Urine?
According to Choosing Wisely Canada, urine testing should only be performed when minimum criteria for UTI are met.²⁸ In non-catheterized patients, testing is recommended only if there is:
- Acute dysuria
- Two or more of the following
- Fever > 37.9°C
- New urgency
- Frequency
- Suprapubic pain
- Hematuria
- Flank pain
- New incontinence
- In catheterized patients, urine testing should be considered only if there is:
- Fever
- Shaking, chills
- Flank pain
- New delirium after other causes have been ruled out
Falls and confusion alone are not indications for urine testing. In these cases, a positive culture almost always represents colonization.
ASB and Delirium: A Common ED Pitfall
A frequent pitfall in the ED is treating ASB in patients with delirium. We often assume “UTI equals the cause of delirium,” but the evidence does not support this.²⁹ Delirium is usually multifactorial.
Asymptomatic bacteriuria alone does not cause delirium, and without urinary symptoms, UTI should be a diagnosis of exclusion. Even when the urine culture is positive, in a clinically stable patient, a 24-hour trial of hydration and supportive care can be a safe and reasonable first step before starting antibiotics.
A systematic review and meta-analysis published in the Journal of the American Geriatrics Society found insufficient evidence to support a meaningful association between ASB and delirium in adults aged 65 and older.²⁹ Based on this, urine cultures should not be routinely included in delirium workups unless minimum UTI criteria are met.
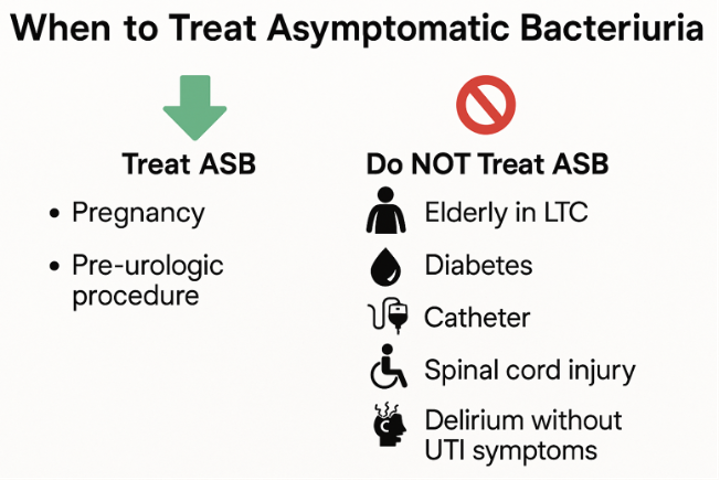
Both the IDSA and Canadian guidelines are clear:
- ASB should only be treated in pregnancy or prior to urologic procedures
- Treating ASB in other populations offers no clinical benefit
- Delirium alone without signs of infection should not trigger urine testing or antibiotic therapy
What About Patients Who Cannot Give a History?
Many delirious patients are not reliable historians.
So how should we approach them?
Infectious diseases experts emphasize that without objective findings of UTI, such as suprapubic tenderness, fever, leukocytosis, or hemodynamic instability, we should not be testing or treating for ASB, even in patients with altered mental status.
The Bottom Line – ASB
The guidelines are clear and the consensus is strong. Do not treat colonization, except in pregnancy or before urologic procedures.
Asymptomatic bacteriuria is incredibly common in the ED, which makes it one of the simplest and highest-impact stewardship opportunities we have.
Because we see it so often, it is also one of the easiest places to start making a meaningful difference.
Every Prescription Matters
Antibiotic overuse is common in the ED, but that also gives us an opportunity to lead change.
Being judicious with antibiotics is not withholding care. It is practicing evidence-based medicine that protects both individual patients and public health.
Even small changes add up.
Cutting just 10% of unnecessary prescriptions could spare hundreds of patients from avoidable side effects and help slow antimicrobial resistance.
Importantly, ED antimicrobial stewardship programs have repeatedly shown that antibiotic use can be reduced without compromising patient outcomes.³⁰
Engage Your Patients
Let’s be honest. Especially when we are tired, it can feel easier to fold to a patient’s request for antibiotics than to explain why they are not needed. But think about it this way.
If a patient asked for narcotics without an indication, would we simply hand over a prescription? Or would we take a moment to explain our reasoning? The same logic applies to antibiotics. Choosing the harder conversation over the easier prescription is part of practicing good medicine.
Antimicrobial stewardship is not about withholding care. It is about delivering safer, more appropriate care. Just as we do not CT every headache, we do not need to treat every fever with piperacillin-tazobactam or IV antibiotics.
And remember: If the gut works, use it.
Antimicrobial stewardship is not just for infectious disease specialists. It is a core part of emergency medicine. Key points to remember:
- Not every positive test means infection. Treat infections, not colonization.
- If antibiotics are needed, tailor them. Use your antibiogram, choose oral therapy when possible, and avoid unnecessarily prolonged courses.
- Do not default to broad-spectrum antibiotics in stable patients. Use the narrowest effective agent.
- Most penicillin allergy labels are low risk, and many can be safely challenged in the ED.
- Confusion and a positive urine test alone do not equal a UTI.
Every decision we make, whether starting or withholding antibiotics, shapes both patient outcomes and public health.
And even small changes in practice can have a major impact.
I want to leave you with this quote:
“No snowflake in an avalanche ever feels responsible.”
It is a powerful reminder that individual actions, while they may seem small, can collectively create massive impact. Antibiotic prescribing works the same way.
One “just in case” prescription does not feel like a big deal in the moment. But across departments and across hospitals, those decisions add up.
They contribute to antimicrobial resistance, C. difficile, and adverse drug events, not because any one of us intends harm, but because we do not always pause to ask ourselves an important question:
Are you treating the patient, or are you treating yourself?
Antimicrobial stewardship is about recognizing that we are all part of that avalanche, and that we also have the power to slow it down. Because in the end, every prescription matters.
References
- Lishman H, Cragg A, Chuang E, Zou C, Marra F, Grant J, Patrick DM, Hohl CM. ICD-10 Codes to Identify Adverse Drug Events Associated with Antibiotics in Administrative Data. Antibiotics (Basel). 2025;14(3):314. https://doi.org/10.3390/antibiotics14030314
- Murray CJ, Ikuta KS, Sharara F, Swetschinski L, Aguilar GR, Gray A, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–55
- Public Health Agency of Canada. Canadian Antimicrobial Resistance Surveillance System — 2021 Report. Ottawa: PHAC; 2022. Available at: https://www.canada.ca/en/public-health/services/publications/drugs-health-products/canadian-antimicrobial-resistance-surveillance-system-report-2021.html
- Saatchi A, Yoo JW, Schwartz KL, Silverman M, Morris AM, Patrick DM, McCormack J, Marra F. Quantifying the gap between expected and actual rates of antibiotic prescribing in British Columbia, Canada. Antibiotics (Basel). 2021;10(11):1428. doi:10.3390/antibiotics10111428.
- Ladines-Lim JB, Fischer MA, Linder JA, Chua KP. Appropriateness of antibiotic prescribing in US emergency department visits, 2016–2021: a national analysis. Antimicrob Steward Healthc Epidemiol. 2024;4:e79. doi:10.1017/ash.2024.79
- Roberts RM, Bartoces M, Thompson S, et al. Antibiotic prescriptions associated with dental-related diagnoses in emergency departments. Ann Emerg Med. 2019;37:2248–55.
- Polgreen PM, Chen Y, Cavanaugh JE, et al. Antibiotic prescribing patterns for adults diagnosed with uncomplicated upper respiratory tract infections in the emergency department and inpatient setting. Infect Control Hosp Epidemiol. 2015;36(12):1452–1455.
Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4569640/
- Lasry D, Chan T, Levin JE, et al. Empiric broad-spectrum antibiotic use in Canadian emergency department sepsis patients compared with microbiologic isolate susceptibility. J Assoc Med Microbiol Infect Dis Can. 2024;9(1):19–28.
doi:10.3138/jammi-2024-0024
- McCarthy K, et al. Oral or intravenous antibiotics? 2020. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7186270/
- Marras TK, Nopmaneejumruslers C, Chan CKN. Efficacy of exclusively oral antibiotic therapy in patients hospitalized with nonsevere community-acquired pneumonia: a retrospective study and meta-analysis. Am J Med. 2004;116(6):385–393. doi:10.1016/j.amjmed.2003.11.013.
- Freifeld AG, Bow EJ, Sepkowitz KA, et al. Oral versus intravenous antibiotic therapy for febrile neutropenia in cancer patients. Cochrane Database Syst Rev. 2013;CD003992. doi:10.1002/14651858.CD003992.pub3. Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003992.pub3/full
- Teng GL, Chi J-Y, Zhang H-M, Li X-P, Jin F. Oral vs parenteral antibiotic therapy in adult patients with community-acquired pneumonia: a systematic review and meta-analysis of randomized controlled trials. J Glob Antimicrob Resist. 2023;32:88–97. doi:10.1016/j.jgar.2022.12.010
- Davar K, Clark D, Centor RM, Dominguez F, Ghanem B, Lee R, Lee TC, McDonald EG, Phillips MC, Sendi P, Spellberg B. Can the future of ID escape the inertial dogma of its past? The exemplars of shorter is better and oral is the new IV. Open Forum Infect Dis. 2023;10(1):ofac706. doi:10.1093/ofid/ofac706
- Choosing Wisely Canada. Choosing Wisely Canada recommendations: Antibiotic stewardship and appropriate use. Choosing Wisely Canada; 2017. Available from: https://choosingwiselycanada.org/recommendation/infectious-disease/
- Smith S, Govender V, Ackermann RJ, et al. Beta-lactam versus aminoglycoside or fluoroquinolone therapy for serious infections: a systematic review. Cochrane Database Syst Rev. 2014;CD003237.pub2. doi:10.1002/14651858.CD003237.pub2. Available from: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003237.pub2/full
- Strohmeier Y, et al. Antibiotics for acute pyelonephritis in children. Cochrane Database Syst Rev. 2014;CD003772.pub4. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10580126
- Isacson D, Smedh K, Nikberg M, et al. Long-term follow-up of the AVOD randomized trial of antibiotic avoidance in uncomplicated diverticulitis. Ann Surg. 2019;269(4):699-704.
- Chabok A, Påhlman L, Hjern F, Haapaniemi S, Smedh K; AVOD Study Group. Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis. Br J Surg. 2012;99(4):532-539.
- Daniels L, Ünlü Ç, de Korte N, et al. Randomized clinical trial of observational versus antibiotic treatment for uncomplicated diverticulitis. Br J Surg. 2017;104(1):52-61.
- Hersh AL, Shapiro DJ, Pavia AT, Shah SS. Antibiotic prescribing in ambulatory pediatrics in the United States. 2015;136(6):105–122. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8615253/
- Choosing Wisely Canada. Antibiotics aren’t always the answer: Choosing Wisely Canada recommendations for antibiotic use in primary care. Toronto (ON): Choosing Wisely Canada Available from: https://choosingwiselycanada.org/primary-care/antibiotics/?highlight=sinusitis
- Worrall GJ, Chaulk P, Matuszczak M, Schwartz B. Antibiotic prescribing for respiratory infections in urgent-care clinics and emergency departments. West J Emerg Med. 2021;22(5):1040–1046. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8487252/
- Li Y, Al Maqrashi Z, Zhan LJ, Siddiqui Z, Jin E, Ellis PM. Use of broad-spectrum antibiotics in adult cancer patients presenting to the emergency department with non-neutropenic fever and/or suspected infection. Support Care Cancer. 2025;33(5):383. doi:10.1007/s00520-025-09419-4
- Trubiano JA, Phillips EJ. Penicillin allergy is not necessarily forever. J Allergy Clin Immunol Pract. 2017;5(3):514–515. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5935455/
- Shenoy ES, Macy E, Rowe T, Blumenthal KG. Evaluation and management of penicillin allergy: a review. JAMA. 2019;321(2):188–199. doi:10.1001/jama.2018.19283.
- Campagna JD, Bond MC, Schabelman E, Hayes BD. The use of cephalosporins in penicillin-allergic patients: a literature review. J Emerg Med. 2012;42(5):612–620. doi:10.1016/j.jemermed.2011.05.035.
- Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Infect Dis. 2019;68(10):e83-e110.
- Choosing Wisely Canada. Urinary tract infection: when to test and when to treat. Toronto (ON): Choosing Wisely Canada; 2017. Available from: https://choosingwiselycanada.org
- Sundvall PD, Ulleryd P, Gunnarsson RK. Delirium in older patients with bacteriuria: a systematic review and meta-analysis. J Am Geriatr Soc. 2011;59(11):2154-2161.
- Savoldi A, Foschi F, Kreth F, Gladstone BP, Carrara E, Eisenbeis S, Buhl M, Marasca G, Bovo C, Malek NP, Tacconelli E. Impact of implementing a non-restrictive antibiotic stewardship program in an emergency department: a four-year quasi-experimental prospective study. Sci Rep. 2020;10:8194. doi:10.1038/s41598-020-65222-7.
-
Dr. Mejbel Alazemi is a junior editor for the EMOttawa Blog, and is a FRCPC resident in the Department of Emergency Medicine, at the University of Ottawa.
View all posts

