

You can find Part 1 on Hemophilia here. For Part 2, we’ll be focusing on hemolytic anemias and thrombotic microangiopathies, or TMAs for short. Defined simply, hemolytic anemia is the destruction of red blood cells before their normal 120-day lifespan. It’s a broad term that encompasses several different etiologies of hemolysis. There are certain historical features that should set off your spidey senses for hemolytic anemia.

Historical Features to Make You Suspect Hemolytic Anemia
- African, South Asian, or Mediterranean background
- Dark urine
- Recent blood transfusion
- A personal history of any autoimmune disorder or mechanical valve, or a family history of anemia or jaundice
- Any medications received within the last few weeks, especially those known to cause hemolytic anemia such as cephalosporins, tetracyclines, hydrocortisone, metformin, procainamide, and methyldopa, among many others
Clinical Features to Make You Suspect Hemolytic Anemia
- Jaundice
- Splenomegaly
Most importantly, if a patient has new anemia without clear, obvious signs of blood loss, in addition to occult GI bleeding we should be suspicious of a hemolytic process and work them up accordingly. Luckily, the ED workup of potential hemolytic anemia is neither costly nor time-consuming.
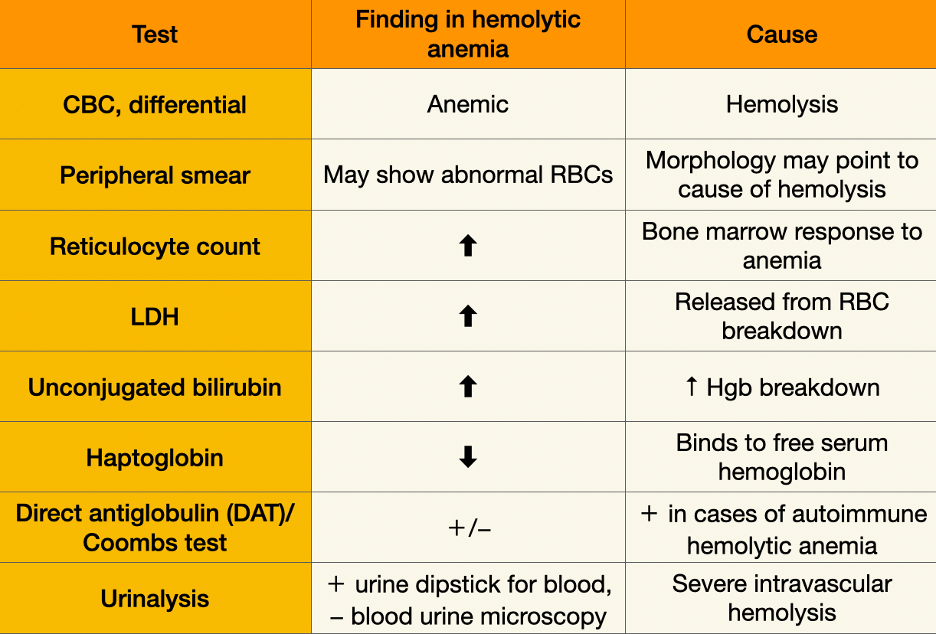
ED Workup of Potential Hemolytic Anemia
-
CBC & Differential
-
Hemolysis typically causes normocytic anemia, but severe hemolysis with reticulocytosis in response can cause the MCV to be elevated, as reticulocytes are larger than mature red blood cells.
-
-
Peripheral Smear
-
The peripheral smear may point us toward the cause of hemolysis, which we’ll come back to in a moment.
-
-
Reticulocyte Count
-
This will tell us whether the bone marrow is reacting appropriately to the anemia by pushing more reticulocytes into circulation.
-
-
LDH, Bilirubin, Haptoglobin
-
Core biomarkers of hemolysis that are part of a hemolytic anemia workup. LDH and bilirubin are elevated because they’re released during RBC breakdown, and haptoglobin is decreased because it binds free serum hemoglobin.
-
-
DAT/Coombs Test & Urinalysis
-
The direct antiglobulin (Coombs) test can be positive or negative in hemolytic anemia, but its utility is in identifying whether this is a case of autoimmune hemolytic anemia, which helps guide treatment. If the hemolysis is severe enough to exhaust the binding capacity of haptoglobin in the serum, free hemoglobin will be filtered out by the kidneys, creating a positive dipstick but negative microscopy for blood.
-
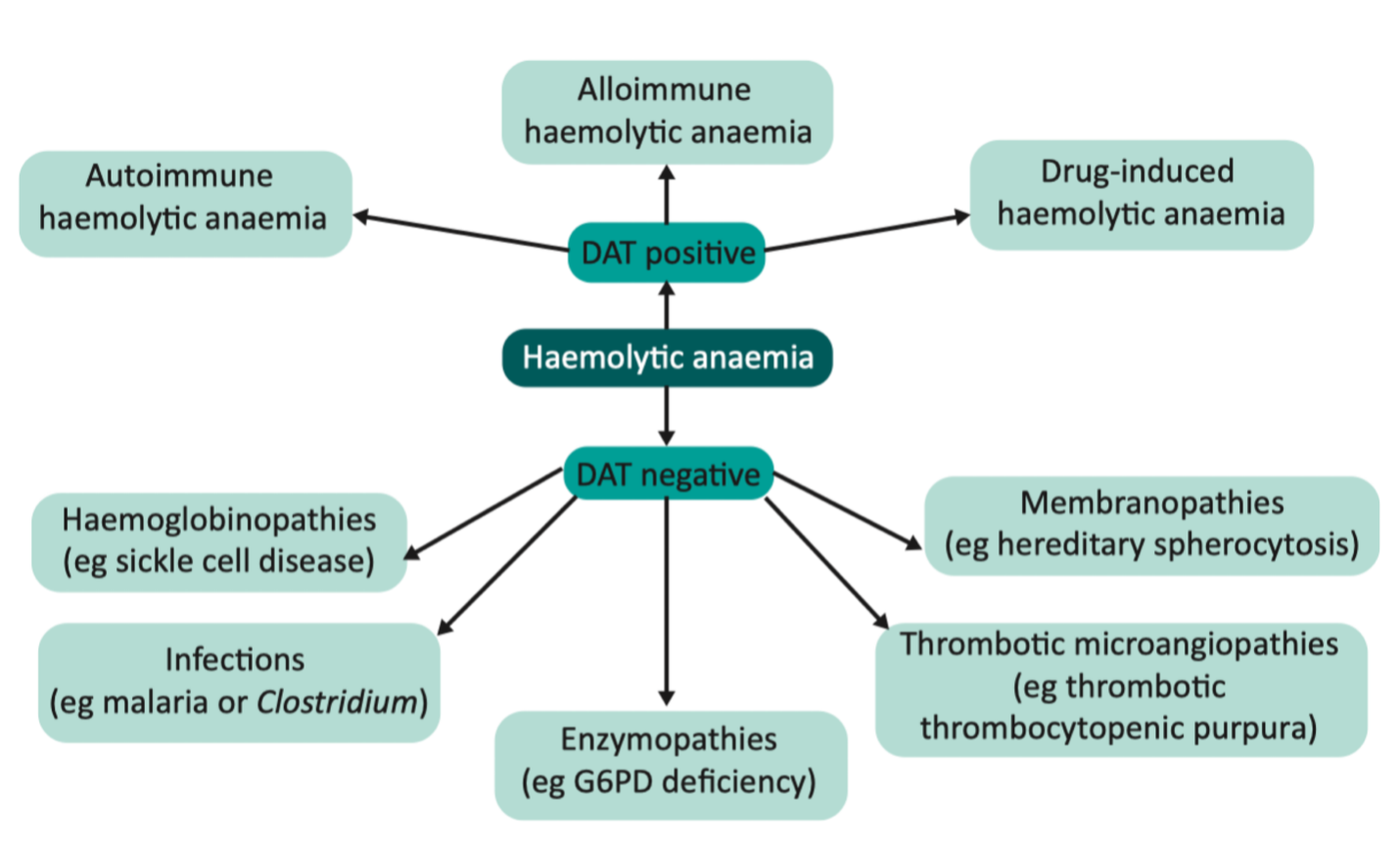
Image source: (https://www.sciencedirect.com/science/article/pii/S1470211824029531?via%3Dihub)
This is a very non-exhaustive diagram, and hemolytic anemias can be categorized according to intrinsic vs. extrinsic, inherited vs. acquired, intravascular vs. extravascular, and DAT positive vs. DAT negative. Each classification on its own would merit a separate post.
For our purposes today, however, hemolytic anemia is a stepping stone to taking a quick look at our third topic — thrombotic microangiopathies.
Thrombotic Microangiopathies (TMAs)
These disorders are complex, so let’s take a practical, ED-workup-based approach to TMAs.
TMAs are a heterogeneous group of disorders with distinct pathophysiologies. All of these disorders have three common features that make up the definition of a TMA:
- Microangiopathic hemolytic anemia (MAHA): anemia plus hemolysis (see above) plus schistocytes on peripheral smear as red blood cells break apart in small vessels.
- Consumptive thrombocytopenia: platelets are being used up in the body.
- End-organ dysfunction: due to endothelial damage or microvascular thrombosis (e.g., ischemia or infarction of the brain, heart, or kidneys).

ED Workup-Based Approach to TMAs
Let’s flesh out our ED workup-based approach to TMAs. This is not a completely comprehensive schema, but one relevant for the most likely presentations we would see in practice.
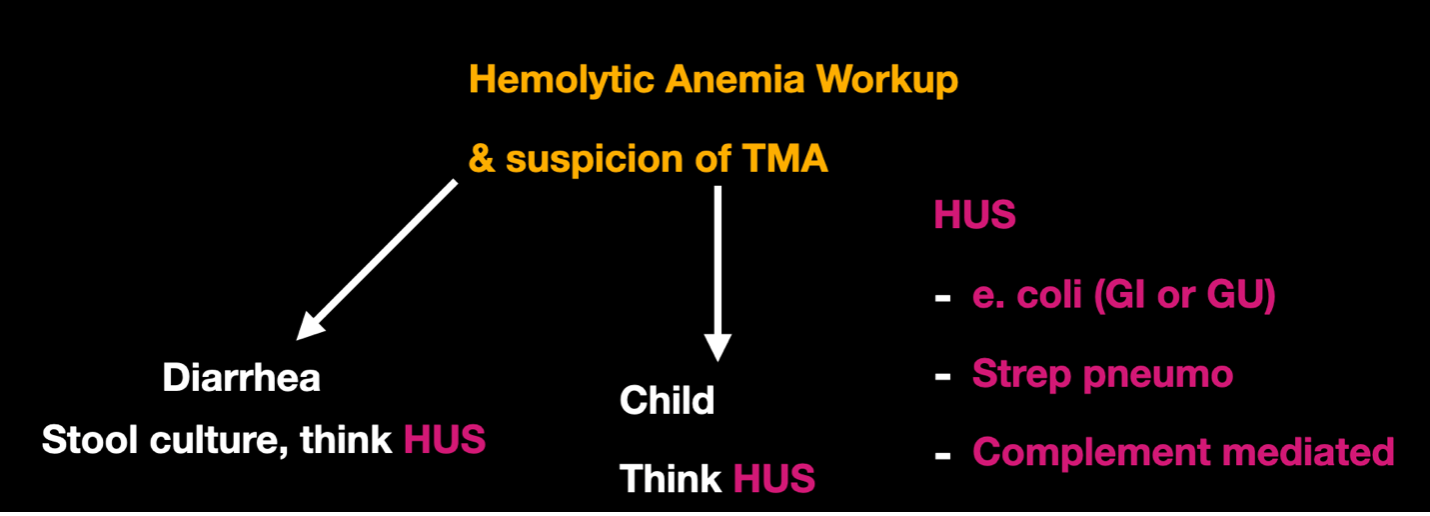
HUS
-
Hemolytic uremic syndrome is most often seen in children, usually under 16 years of age, with the highest incidence in children under 5. Although atypical HUS exists, the vast majority of HUS is typical, associated with Shiga-toxin-producing E. coli GI infections causing diarrhea.
-
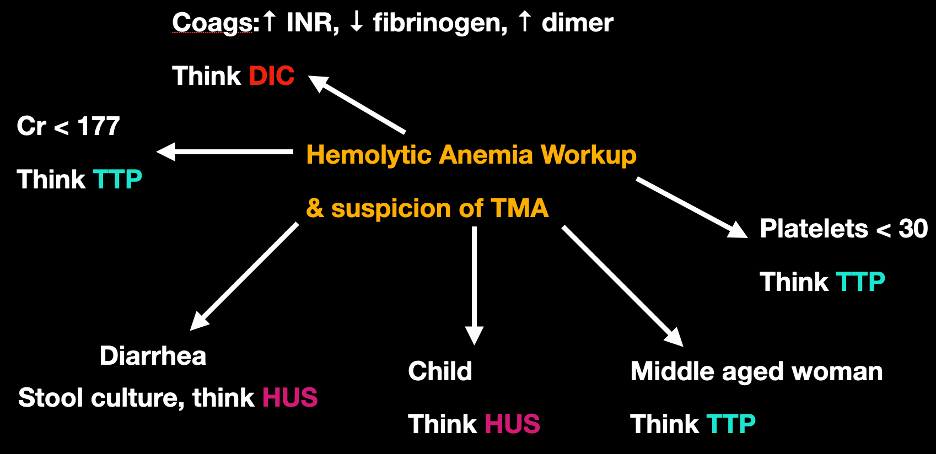
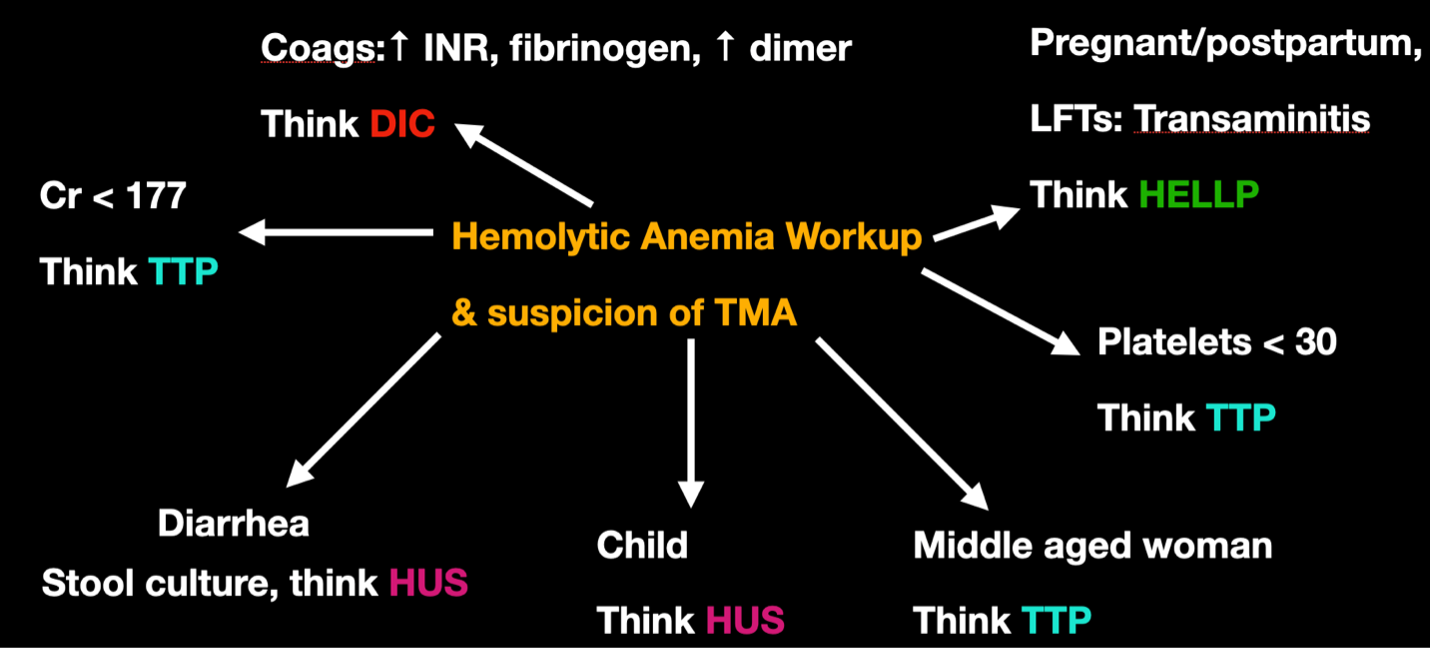
When you think TMA and see a child with diarrhea (especially with severe renal dysfunction), think HUS.
-
In addition to classic HUS, you can also have HUS caused by E. coli genitourinary infections, or by Streptococcus pneumoniae, neither of which would present with diarrhea.
-
Atypical HUS is complement-mediated. Clinically, it’s a diagnosis of exclusion and is still managed with supportive care, with some consideration for anti-complement therapy — not relevant in the ED.
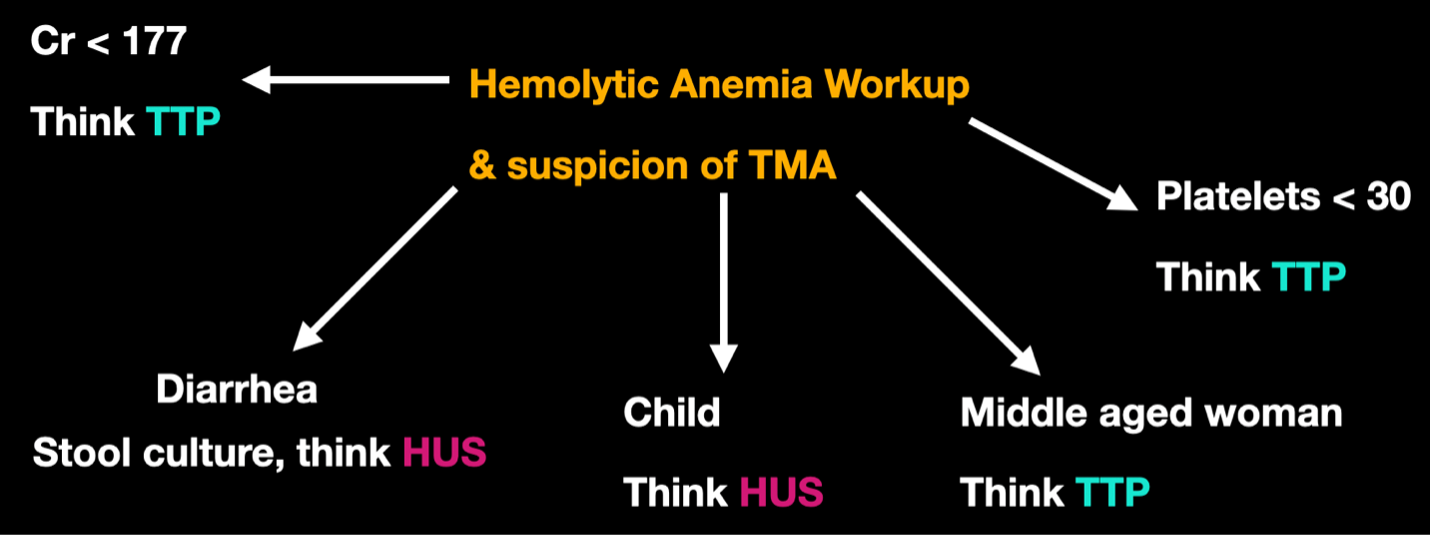
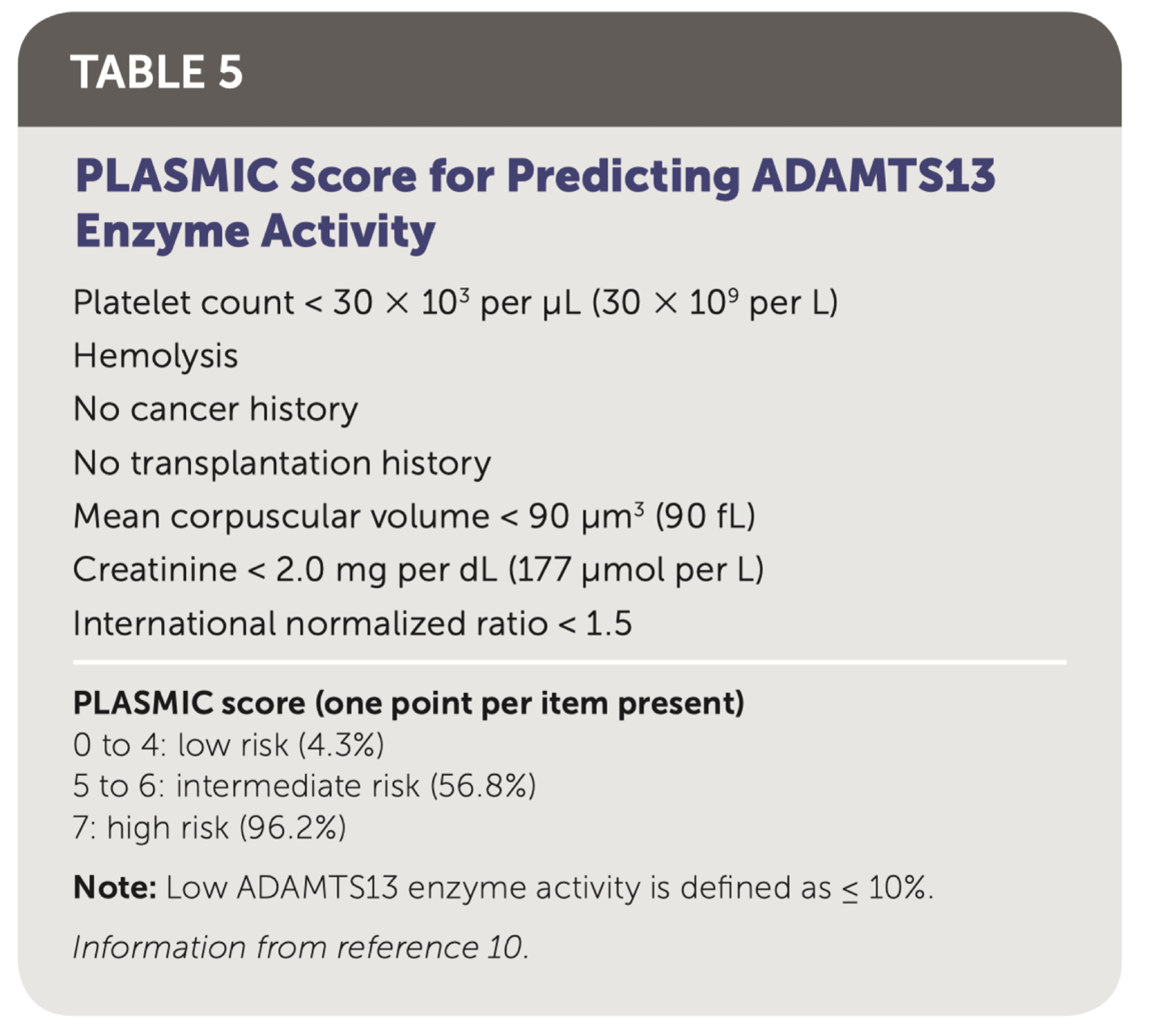
Image source: Hemolytic Anemia: Evaluation and Differential Diagnosis (https://www.aafp.org/pubs/afp/issues/2018/0915/p354.html)
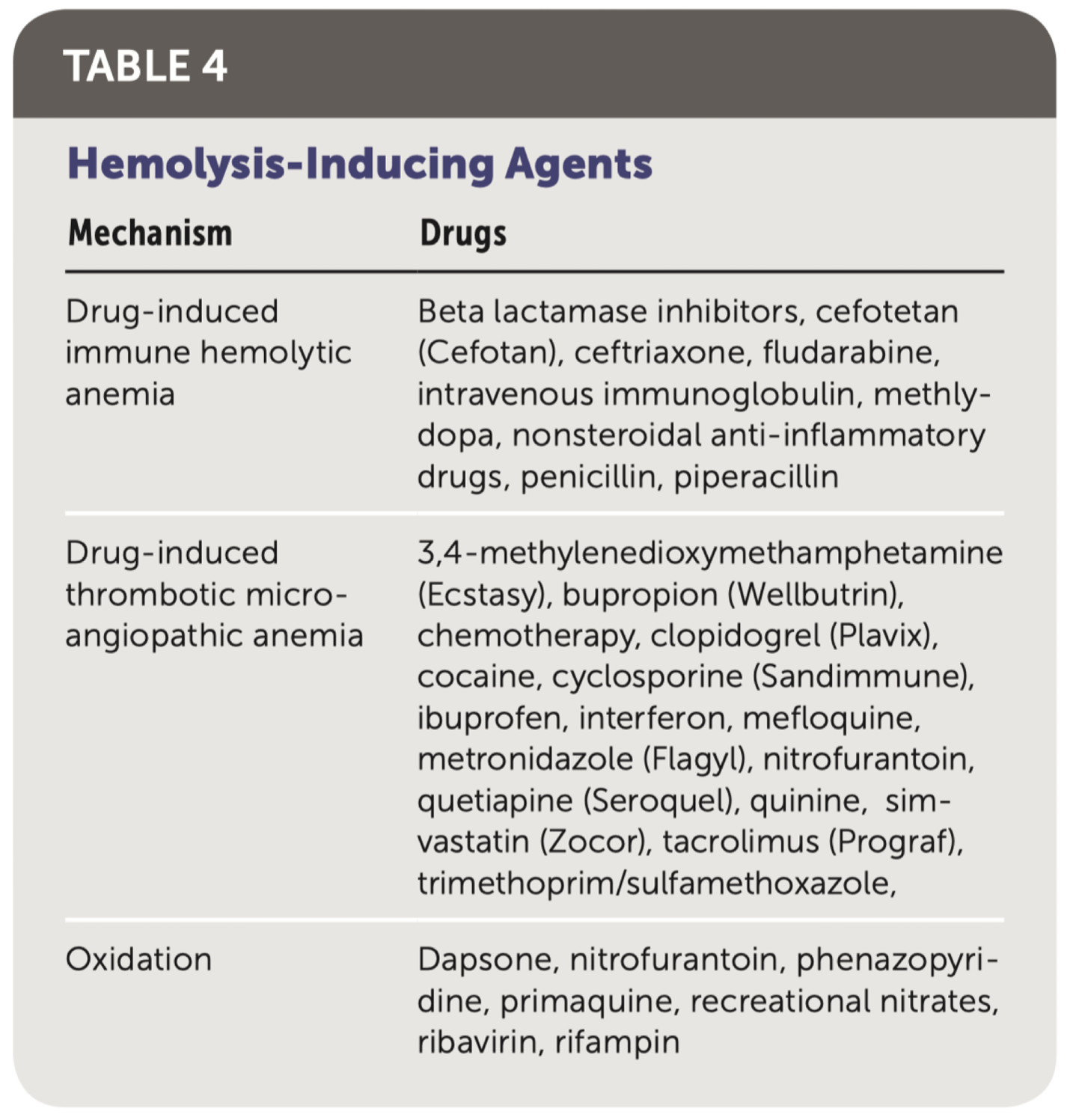
Image source: Hemolytic Anemia: Evaluation and Differential Diagnosis (https://www.aafp.org/pubs/afp/issues/2018/0915/p354.html)
TTP
-
Thrombotic thrombocytopenic purpura is most often associated with adults aged 35–54, with a 2:1 female-to-male ratio. It is associated with comparatively severe thrombocytopenia and less severe renal dysfunction compared to HUS.
-
The hallmark of a diagnosis of TTP is an ADAMTS13 level < 10%. This enzyme cleaves von Willebrand factor multimers in the blood. Traditionally, it has been difficult to obtain an ADAMTS13 level in a timely fashion, so the PLASMIC score was developed to help predict the likelihood of reduced enzyme activity and to guide treatment with plasma exchange. The score is higher when there is a relative lack of coagulopathy and renal injury, which is more consistent with TTP.
-
To make things more confusing, you can have drug-induced TTP, or drug-induced TMA that is not TTP.
DIC
- DIC is differentiated from TTP and HUS by the fact that coagulopathy is unique to DIC.
- The International Society of Thrombosis and Haemostasis and the Japanese Association of Acute Medicine have both published scoring tools for DIC.
HELLP
- If you have a pregnant patient with elevated liver enzymes and a suspicion of TMA, think HELLP.
TMAs can get very complex very quickly. While DIC and HUS are treated with supportive management, and delivery can be the solution to HELLP if pre-partum, TTP has specific management known as therapeutic plasma exchange (PLEX), which has greatly decreased TTP mortality since its creation.
Should we know the PLASMIC Score for TTP? Do we need to order ADAMTS13 levels? What are our hematologists expecting of us — and what should we expect of ourselves?
Expert Opinion – Dr. Tyler James Hematologist and Ottawa Apheresis Program Physician, TOH
Do we need to start PLEX?
“At our centre (TOH), the hematology staff on call and the PLEX staff on call are different physicians. While doing PLEX/Apheresis call, I’ve never been called by the ED directly to initiate PLEX, nor do I think the ED needs to be calling the PLEX staff directly.” It takes time to set up and run PLEX, and during that time the specialty for which plasma exchange may be indicated should be consulted (hematology, neurology, nephrology, or rheumatology), and they can speak with the PLEX physician directly.
“Regarding indications for PLEX, TTP, Guillain-Barré, myasthenia gravis, and acute stroke in patients with sickle cell disease are all emergency-medicine-relevant scenarios in which we should prompt our specialists to consider PLEX when we’re calling for a consult, in addition to our standard ED management. Suspicion for pulmonary-renal syndrome would also be a potential indication.”
And lastly, to end on a reassuring note (regarding the PLASMIC score)
“We don’t need to be calculating yet another score in the ED. Continue to do what we do best — rapid, efficient recognition and stabilization of acutely ill, undifferentiated patients.”
Do we need to send an ADAMTS13?
At our institution, ADAMTS13 is run once daily and is unlikely to significantly affect any ED management, although it may help our colleagues downstream.
Take-Home Points
-
For new unexplained anemia without a clear bleeding source, think about (and order workup for) hemolytic anemia, in addition to considering occult GI blood loss.
-
Hemolytic anemia + consumptive thrombocytopenia + end-organ dysfunction (brain, heart, kidneys) = consider thrombotic microangiopathy.
-
While they may need advanced therapies such as PLEX eventually, prompt resuscitation and supportive care for critically ill patients with hemolytic anemia or TMA is the cornerstone of ED management.
The diagnostic and therapeutic momentum we initiate for our patients often carries far beyond their initial hours in the ED. As emergency physicians, we hold an outsized influence on the trajectory of our patients, and I hope this post provided you with some pearls to make your high-quality emergency medicine practice even better.
References
- https://www.aafp.org/pubs/afp/issues/2018/0915/p354.html
- https://www.sciencedirect.com/science/article/pii/S1470211824029531?via%3Dihub
- https://acrjournals.onlinelibrary.wiley.com/doi/10.1002/art.42681
- https://www.rpthjournal.org/article/S2475-0379(22)01199-2/fulltext
- https://www.sciencedirect.com/science/article/abs/pii/S0022347698703038
- https://link.springer.com/article/10.1007/s00467-005-1843-7
- https://www.thieme-connect.com/products/ejournals/abstract/10.1055/s-0039-1679907
- https://www.thelancet.com/journals/lanhae/article/PIIS2352-3026(16)30018-7/abstract
- https://www.sciencedirect.com/science/article/abs/pii/S0049384811004749
- https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2141.2009.07600.x
