
As of 2024, approximately 15% of Canadians live with Diabetes Mellitus (DM). Type I DM accounts for 5-10% of these cases and is more commonly associated with Diabetic Ketoacidosis (DKA). Patient’s with DKA may present with varied levels of acuity, requiring prompt recognition and initiation of appropriate treatment to prevent further deterioration.
Despite its prevalence, the management of DKA continues to evolve, with new evidence challenging long-standing protocols. In this post, we explore the latest updates in DKA care, including recommendations from the Joint British Society and the American Diabetes Association (ADA) guidelines.
Objectives:
- Review the pathophysiology of DKA
- Define DKA
- Discuss the four pillars of DKA management, which include:
- Restoration of extracellular fluid volume
- Correction of electrolyte abnormalities
- Correction of ketoacidosis
- Correction of hyperglycemia
Understanding DKA: Pathophysiology and Diagnosis
Under normal physiological conditions, glucose is the primary energy substrate or metabolic fuel for ATP production and aerobic metabolism. Our bodies maintain relatively stable blood glucose levels through three primary methods: GI absorption in the fed state and glycogenolysis and gluconeogenesis in the fasting state. Insulin is the primary hormone responsible for lowering blood glucose levels in the fed state. Glucagon is the primary counter-regulatory hormone responsible for maintaining blood glucose levels in the fasting and/or starving state.
Type I DM is characterized by autoimmune destruction of pancreatic beta cells, resulting in hyperglycemia and the eventual need for exogenous insulin due to absolute insulin deficiency. Type II DM is characterized by a relative insulin deficiency due to a combination of pancreatic beta cell damage and increased insulin resistance.
The first step in the pathophysiology of DKA is a significant insulin deficiency resulting in an inability of cells to uptake and utilize blood glucose. This results in hyperglycemia and increased activity of counter-regulatory hormones (glucagon, catecholamines, cortisol), which further worsens hyperglycemia. Eventually, lipolysis with fatty acid oxidation to ketone bodies ensues. Secondary to hyperglycemia and insulin deficiency, patients typically experience osmotic diuresis resulting in dehydration and electrolyte disturbances.
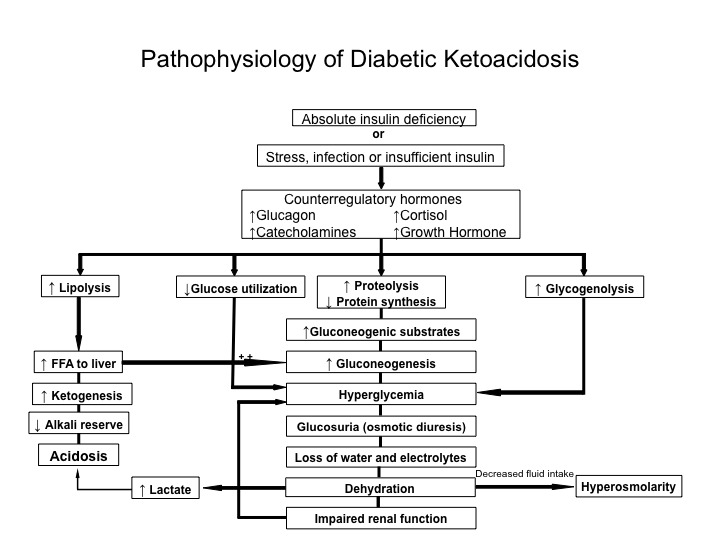
Figure 1. DKA Pathophysiology. Image from Wolfsdorg et al 2006.
Definition of DKA:
There is no universally agreed-upon definition or definitive diagnostic criteria for DKA. The following is classically used:
- Serum glucose >11.1 mmol/L
- Anion gap >12 mmol/L with positive serum/urine ketones
- pH ≤7.3 or HCO₃ ≤15 mmol/L
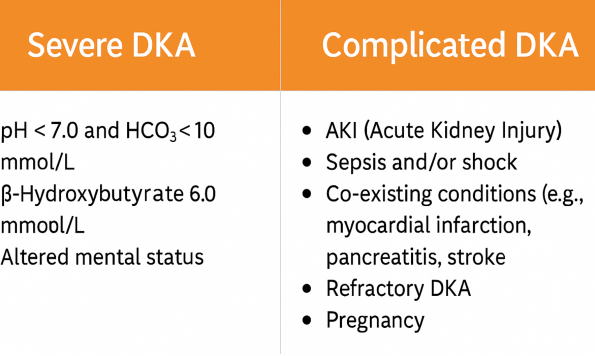
The American Diabetes Association (ADA) further stratifies DKA into mild, moderate, and severe based on pH, beta-hydroxybutyrate level, bicarbonate level, and mental status.
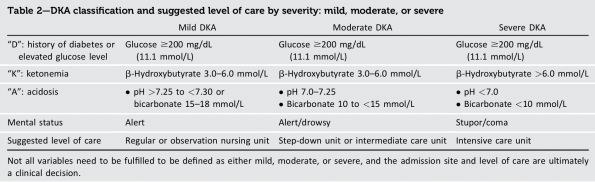
Image from American Diabetes Association, Diabetes Care 2024
DKA Triggers:
- Infection
- Insulin omission
- Initial presentation
- Ischemia
- Intoxication
- Pregnancy (Impregnanted to keep the I)
- Iatrogenic (i.e. medications)
Euglycemic DKA and SGLT2 Inhibitors:
Euglycemic DKA is often triggered by SGLT2 inhibitors, but it can also occur in other ketogenic states such as pregnancy. SGLT2 inhibitors have become a commonly used medication in patients with Type II DM and other comorbidities like heart failure with reduced ejection fraction and chronic kidney disease due to proven mortality benefits. The sodium-glucose transporter 2 is located in the renal proximal convoluted tubule. This is responsible for the reabsorption of approximately 90% of filtered glucose in the kidneys. SGLT2 inhibitors block glucose reabsorption, leading to glycosuria and osmotic diuresis. Furthermore, the pathophysiology of euglycemic DKA remains very similar to ‘classical DKA’; however, with a potentially normal serum glucose, it will be important to have an updated medication list to identify culprit drugs and maintain a high level of suspicion in the right clinical context.
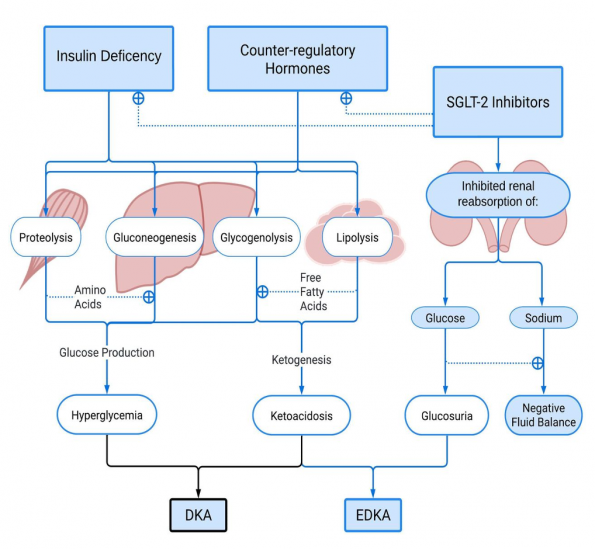
Figure 2. Euglycemic DKA pathophysiology. Image from Chow et al. 2023.
Clinical Pearl
Urine ketones are mainly acetoacetate, and these are only a surrogate measurement of the clinically relevant capillary or serum ketone 3-beta-hydroxybutyrate. In diabetic ketoacidosis, the 3-beta-hydroxybutyrate to acetoacetate ratio increases from 1:1 to 5:1. Measuring urine ketones may therefore initially underestimate the severity of DKA or result in delayed diagnosis. Therefore, if euglycemic DKA is on your differential, do not rely on urine ketone testing alone. Order a serum 3-beta-hydroxybutyrate level if it is available at your institution, as it will be more sensitive during the early stages of disease progression.
Treatment of DKA in the Emergency Department
Fluid resuscitation: Choosing the right IV fluids
One of the mainstays of DKA treatment is IV fluids. The overall goal of IV fluids is to resuscitate and stabilize the patient and eventually normalize extracellular fluid volume. At the same time, this will lower blood glucose levels and alter electrolyte concentrations. The consensus amongst different guidelines has been to use a 0.9% sodium chloride solution as your initial choice of IV fluid. The question remains as to whether Ringer’s lactate is a better choice of fluid in these patients to prevent worsening acidosis. A systematic review and meta-analysis by Szabo et al. (2024) was published in the Journal of Diabetes Metabolism Research and Review comparing DKA resolution when fluid resuscitated with balanced electrolyte solutions versus 0.9% sodium chloride solution. Results showed that balanced electrolyte solutions (e.g., Ringer’s Lactate) may resolve DKA faster and reduce complications like hyperchloremic acidosis when compared to 0.9% sodium chloride solution.
Another systematic review and meta-analysis by Hammond et al (2020) looked at fluid comparison in critically ill adults. This study found that balanced crystalloids are associated with lower hospital and 30-day mortality and less incidence of AKI. The reason this may be important in DKA is mainly due to the high chloride content in the 0.9% NaCl solution, which can precipitate hyperchloremic acidosis in addition to ketoacidosis.
Bottom line
If the patient appears clinically well and fits the mild/moderate DKA criteria, it probably doesn’t matter what fluid you resuscitate them with; pick your poison. If the patient has a significant AKI, poor baseline lung function, or is critically ill with severe DKA, this is the patient for whom using Ringer’s lactate upfront and continuing to monitor the total volume of fluid administered is likely beneficial.
Clinical Pearl
Possibly an even more important point when discussing fluids is the decision on how to administer them. There has been a lot of research in both adult and pediatric DKA surrounding the two-bag method. This method means you have one bag containing saline WITHOUT dextrose, and the other containing saline WITH dextrose. Both bags contain identical electrolyte concentrations. The two bags are connected via a Y-connector, allowing rapid adjustment of the proportion of dextrose delivered by varying the infusion rates of each bag while maintaining a constant total fluid rate. A recent systematic review and meta-analysis by Srikrishnaraj et al (2025) supports the two-bag method (saline with and without dextrose) for reducing hypoglycemia and shortening DKA resolution time. The study also found lower rates of hypokalemia and insulin infusion duration in adults.
Correction of Electrolyte Abnormalities
Sodium
- Hyponatremia is a common laboratory finding in DKA
- The reduction in serum sodium is primarily linked to the effective osmolality of uncontrolled hyperglycemia; this is termed “hyperosmolar hyponatremia.”
- Typically, serum sodium levels will quickly correct after initiation of insulin therapy
- The true sodium status is best assessed by calculating the glucose–corrected sodium concentration (click here to access the MDCalc Sodium Correction for Hyperglycemia Calculator).
- Practically, it is easiest to remember that for every 5.6 mmol/l increase in glucose, a patient’s serum sodium will drop by approximately 1.6 mmol/l.
What is a major complication related to IV fluids and hyponatremia in DKA?
- Cerebral edema is likely caused by miscalculated fluid resuscitation with either a hypotonic solution or excessive volume, contributing to decreased effective plasma osmolality
- Another widely accepted theory of pathogenesis is ischemia-reperfusion injury and capillary leakage in the setting of inflammation and impaired autoregulation
Should we be worried about cerebral edema as a complication of DKA treatment?
- The highest rates of cerebral edema are in the pediatric population
- Kuppermann et al (2018) conducted a large 13-center randomized controlled trial published in the New England Journal of Medicine, looking at 0.9% NaCl solution vs. 0.45% NaCl solution, along with rates of fluid administration in the pediatric population, and found the following:
- Very low rates of any neurologic deterioration (3.5%), and even less clinically apparent brain injury (0.9%). There were also no significant differences between memory and IQ scores between groups.
In summary, the incidence of clinically significant cerebral edema is exceedingly low in the pediatric patient population and even lower in adults. The most important aspects of treatment to best protect our patients from this complication are to calculate a corrected sodium level and recheck serum osmolality to ensure it is not dropping by more than approximately three millimoles per kilogram per hour.
Potassium
- Potassium is the primary intracellular cation in the human body.
- In DKA, there is an extracellular shift and a total body potassium deficit of approximately 2-5 mmol/kg.
- To put this in perspective, under normal conditions, our bodies contain approximately 50 mmol/kg of potassium. So, patients with DKA will lose anywhere from 5-10% of their total potassium stores.
Potassium replacement should be tailored:
- In most individuals, we want to administer 10 mmol of potassium for every 0.1 mmol/L desired increase in serum potassium.
- Oral potassium may be suitable for patients at some point during their hospital stay, but it is not recommended initially due to unreliable bioavailability in the setting of acute illness, and I would not recommend PO supplementation while under the Emergency Physician’s care.
- If IV access is established:
- Serum [K] between 4.1 and 5.4 mmol/L ⇒ administer KCl 20 mmol/L
- Serum [K] between 3.3 and 4.0 mmol/L ⇒ administer KCl 40 mmol/L
- Assess kidney function and ensure adequate urine output after the initial 2-hour electrolyte check
- Adjust KCl administration based on patient response.
- In severe DKA, there should be a low threshold for ED providers to obtain central venous access if initial serum [K] ≤ 3.3 mmol.
Extended Electrolytes
- No indication for routine replacement of calcium, magnesium, or phosphate.
- If initial laboratory values are below the lower limit of normal or the patient is symptomatic, then treat accordingly
- Keep in mind that hypomagnesemia will impact your ability to correct hypokalemia, so it is very reasonable to aim for a Magnesium level of >1.0 mmol/L.
- Phosphate replacement is only indicated if a patient shows signs of muscle weakness, respiratory compromise, and their phosphate is less than 1.0 mmol/l.
Sodium Bicarbonate
- Consensus amongst all guidelines is that it should only be considered in severe DKA (pH ≤ 7.0) or if there is a coexisting illness where it is indicated.
Correction of Ketoacidosis and Hyperglycemia
Insulin Therapy:
Subcutaneous insulin is the most common route of administration for both hospitalized patients and patients living with diabetes in the community. So, why is it that we use intravenous insulin for the treatment of DKA?
- Rapid onset of action
- Predictable pharmacokinetics
- Easily titratable
- Improved glycemic control in critically ill patients
Bottom line
Diabetes Canada, the American Diabetes Association, and the Joint Diabetes British Diabetic Societies for inpatient care agree that IV insulin infusion is the standard of care when treating patients with severe and complicated DKA.
Clinical Pearl
Current guidelines recommend against the routine use of an intravenous insulin bolus during DKA management as it increases the risk of hypoglycemia, hypokalemia, and might create greater shifts in serum osmolality.
Intravenous insulin infusion + basal insulin
The ADA standard of care 2025 guidelines suggest that providing basal long-acting insulin in conjunction with the IV insulin infusion may prevent rebound hyperglycemia without increased risk of hypoglycemia. The Joint British Diabetes Societies have been very clear since 2013, stating that intermediate or long-acting insulin should always be continued in patients with DKA if they are on it at home. While it is reasonable for basal insulin to be ordered in conjunction with intravenous insulin therapy, this should only be done once it is an established part of your institution’s DKA protocol to ensure consistency across providers and prevent human errors.
Standalone subcutaneous insulin
Emerging evidence supports standalone subcutaneous (SC) insulin for the treatment of certain patients with DKA. The ADA guidelines 2025 suggest that SC insulin is as effective as IV human regular insulin in treating mild to moderate DKA in uncomplicated patients. SC insulin protocols may be safer and more cost-effective than treatment with IV insulin.
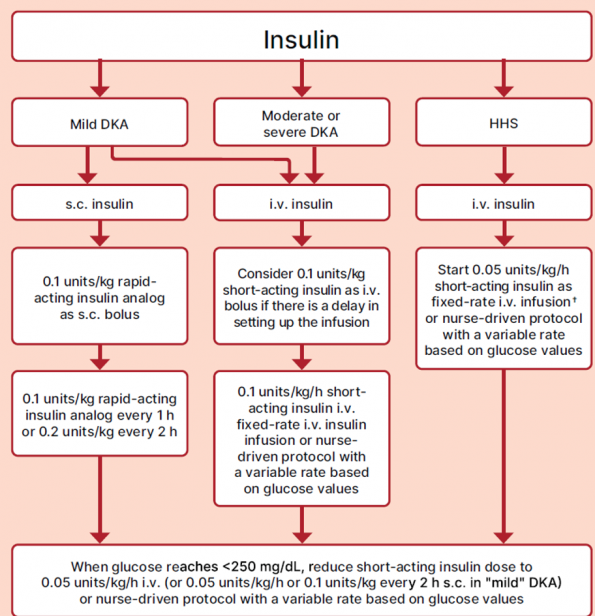
Figure 3. Insulin therapy guidelines for DKA and HHS. Image from Diabetes Care 2025.
Several recent studies, including the CRABI-DKA trial by Ibarra Jr et al (2025) have shown safety and efficacy with using a combination of both rapid-acting insulin analogues and long-acting insulin analogues for the treatment of mild to moderate DKA. Although not endorsed by any major guidelines yet, this is an exciting area of research that may be incorporated into guidelines in the future.
Subcutaneous insulin protocols show promise in the following settings:
- Institutions that require ICU admission for IV insulin infusions
- Low resource settings where IV insulin infusions are not feasible
- Potentially in the pre-hospital setting as a bridge to definitive care either in the community or hospital setting
Summary and Key Takeaways
- Measure a serum beta-hydroxybutyrate level if you suspect euglycemic DKA
- Preferentially use Ringer’s Lactate over 0.9% NaCl in severe DKA
- The overall risk of cerebral edema is low, be more cautious in the pediatric population
- IV potassium is preferred in the ED: tailor dosing to serum levels
- Continue basal insulin when appropriate; consider standalone SC insulin for mild DKA in the appropriate setting
- Protocol standardization is essential for safe and effective care
References
Alnuaimi, A., Mach, T., Reynier, P., Filion, K. B., Lipes, J., & Yu, O. H. Y. (2024). A systematic review and meta-analysis comparing outcomes between using subcutaneous insulin and continuous insulin infusion in managing adult patients with diabetic ketoacidosis. BMC Endocrine Disorders, 24, 133. https://doi.org/10.1186/s12902-024-01666-6
American Diabetes Association Professional Practice Committee. (2025). Diabetes care in the hospital: Standards of care in diabetes—2025. Diabetes Care, 48(Suppl. 1), S321–S334. https://doi.org/10.2337/dc25-S016
Caldwell, T., Walton, S., & Long, B. (2025). Is subcutaneous insulin administration safe and effective for the treatment of mild to moderate diabetic ketoacidosis? Annals of Emergency Medicine, 85(3), 273–275. https://doi.org/10.1016/j.annemergmed.2024.10.020
Canadian Diabetes Association. (2018). Appendix 6: Types of insulin. Canadian Journal of Diabetes, 42(Suppl 1), S314. https://doi.org/10.1016/j.jcjd.2017.12.006
Chow, E., Clement, S., & Garg, R. (2023). Euglycemic diabetic ketoacidosis in the era of SGLT-2 inhibitors. BMJ Open Diabetes Research & Care, 11, e003666. https://doi.org/10.1136/bmjdrc-2023-003666
Defante, M. L. R., de Souza, M. M., Mendes, B. X., De Hollanda Morais, B. A. A., Prizão, V. M., Parolin, S. A. E. C., & Francisco, H. V. (2024). Subcutaneous rapid-acting insulin analogues in mild to moderate diabetic ketoacidosis: A meta-analysis of randomized controlled trials. Journal of Diabetes and Its Complications, 38, 108882. https://doi.org/10.1016/j.jdiacomp.2024.108882
Goguen, J., & Gilbert, J. (2018). Hyperglycemic emergencies in adults. Canadian Journal of Diabetes, 42(Suppl 1), S109–S114. https://doi.org/10.1016/j.jcjd.2017.10.013
Griffey, R. T., Schneider, R. M., Girardi, M., Yeary, J., McCammon, C., Frawley, L., Ancona, R., & Cruz-Bravo, P. (2023). The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. Academic Emergency Medicine, 30(8), 800–808. https://doi.org/10.1111/acem.14685
Hammond, N. E., et al. (2019). Balanced crystalloids versus saline in critically ill adults: A systematic review and meta-analysis. American Journal of Respiratory and Critical Care Medicine, 199(9), 1107–1115. https://doi.org/10.1164/rccm.201806-1160OC
Hsia, E., Seggelke, S., Gibbs, J., Hawkins, R. M., Cohlmia, E., Rasouli, N., Wang, C., Kam, I., & Draznin, B. (2012). Subcutaneous administration of glargine to diabetic patients receiving insulin infusion prevents rebound hyperglycemia. Journal of Clinical Endocrinology & Metabolism, 97(9), 3132–3137. https://doi.org/10.1210/jc.2012-1244
Ibarra, F., Cruz, M., Chinnock, B., Sunde, C., Campagne, D., & Uller, M. (2025). Evaluation of an alternative approach to managing diabetic ketoacidosis: Combination rapid-acting and basal subcutaneous insulin (CRABI-DKA). Annals of Pharmacotherapy, 59(3), 277–288. https://doi.org/10.1177/10600280251331967
Joint British Diabetes Societies for Inpatient Care (JBDS). (2023). The management of diabetic ketoacidosis in adults. Revised March 2023. Retrieved from https://abcd.care/joint-british-diabetes-societies-jbds-inpatient-care-group
Kuppermann, N., Ghetti, S., Schunk, J. E., Stoner, M. J., Rewers, A., McManemy, J. K., … Glaser, N. S. (2018). Clinical trial of fluid infusion rates for pediatric diabetic ketoacidosis. New England Journal of Medicine, 378(24), 2275–2287. https://doi.org/10.1056/NEJMoa1716816
Palmer, B. F., & Clegg, D. J. (2016). Physiology and pathophysiology of potassium homeostasis. Advances in Physiology Education, 40(4), 480–490. https://doi.org/10.1152/advan.00121.2016
Rao, P., Jiang, S., Kipnis, P., Patel, D. M., Katsnelson, S., Madani, S., & Liu, V. X. (2022). Evaluation of outcomes following hospital-wide implementation of a subcutaneous insulin protocol for diabetic ketoacidosis. JAMA Network Open, 5(4), e226417. https://doi.org/10.1001/jamanetworkopen.2022.6417
Sarikaya, Z. T., Gucyetmez, B., Ozdemir, D., Dogruel, B., Ayyildiz, A., Kesecioglu, J., & Telci, L. (2025). Diabetic ketoacidosis fluid therapy algorithm in the golden hours: Iatrogenic hyperchloremic acidosis instead of unmeasured anion acidosis. Journal of Clinical Medicine, 14(4125). https://doi.org/10.3390/jcm14124125
Srikrishnaraj, A., Souter, A. R., Woods, N., Van Aarsen, K., Iansavitchene, A., Haas, N. L., & Yan, J. W. (2025). Two-bag versus one-bag method for adult and pediatric diabetic ketoacidosis management: A systematic review and meta-analysis. Annals of Emergency Medicine. Advance online publication. https://doi.org/10.1016/j.annemergmed.2025.07.032
Stuhr, K., LeeMaster, R., Hickman, A. W., Reachi, B., Pace, W., & Meek, C. (2023). Subcutaneous insulin versus traditional intravenous insulin infusion in treatment of mild to moderate diabetic ketoacidosis. Journal of Emergency Medicine, 65(3), e221–e228. https://doi.org/10.1016/j.jemermed.2023.02.017
Szabó, G. V., Szigetváry, C., Turan, C., Engh, M. A., Terebessy, T., Fazekas, A., Farkas, N., Hegyi, P., & Molnár, Z. (2024). Fluid resuscitation with balanced electrolyte solutions results in faster resolution of diabetic ketoacidosis than with 0.9% saline in adults: A systematic review and meta-analysis. Diabetes/Metabolism Research and Reviews, e3831. https://doi.org/10.1002/dmrr.3831
Thammakosol, K., & Sriphrapradang, C. (2023). Effectiveness and safety of early insulin glargine administration in combination with continuous intravenous insulin infusion in the management of diabetic ketoacidosis: A randomized controlled trial. Diabetes, Obesity and Metabolism, 25(3), 815–822. https://doi.org/10.1111/dom.14929
Umpierrez, G. E., Cuervo, R., Karabell, A., Latif, K., Freire, A. X., & Kitabchi, A. E. (2004). Treatment of diabetic ketoacidosis with subcutaneous insulin aspart. Diabetes Care, 27(8), 1873–1878. https://doi.org/10.2337/diacare.27.8.1873
Umpierrez, G. E., Davis, G. M., ElSayed, N. A., Fadini, G. P., Galindo, R. J., Hirsch, I. B., Klonoff, D. C., McCoy, R. G., Misra, S., Gabbay, R. A., Bannuru, R. R., & Dhatariya, K. K. (2024). Hyperglycemic crises in adults with diabetes: A consensus report. Diabetes Care, 47(8), 1257–1275. https://doi.org/10.2337/dci24-0032
Walls, R. M., Hockberger, R. S., Gausche-Hill, M., Erickson, T. B., Wilcox, S. R., & Brown, C. A. III (Eds.). (2023). Rosen’s emergency medicine: Concepts and clinical practice (10th ed.). Elsevier. ISBN: 978-0-323-75789-8
Wolfsdorf, J., Glaser, N., & Sperling, M. A. (2006). Diabetic ketoacidosis in infants, children, and adolescents: A consensus statement from the American Diabetes Association. Diabetes Care, 29(5), 1150–1159. https://doi.org/10.2337/dc06-9099
Zhang, L., & Tamilia, M. (2018). Euglycemic diabetic ketoacidosis associated with the use of a sodium–glucose cotransporter-2 inhibitor. CMAJ, 190(25), E766–E768. https://doi.org/10.1503/cmaj.171319
Zheng, D. J., Iskander, S., Vujcic, B., Amin, K., Valani, R., & Yan, J. W. (2022). Comparison of adult diabetic ketoacidosis treatment protocols from Canadian emergency departments. Canadian Journal of Diabetes, 46(3), 269–276. https://doi.org/10.1016/j.jcjd.2021.10.010
