Hip fractures are a common emergency department presentation and, with an aging population, their incidence will continue to rise. These injuries are profoundly painful, and many patients experience moderate to severe pain for at least one month following fracture (Morrison & Siu, 2025). Uncontrolled acute pain is a major contributor to the high prevalence of delirium in this population (Francis, 1992). Delirium is not benign and is associated with surgical delays, prolonged immobility, higher complication rates, and lasting loss of independence (Sala et al., 2023).
As emergency physicians, our role in hip fracture management includes accurate neurovascular assessment, timely surgical referral, and, critically, effective analgesia.
Peripheral nerve blocks (PNBs) for hip fractures significantly improve pain scores (Hayashi et al., 2024), reduce the risk of acute in-hospital delirium (Thompson et al., 2018), may decrease the risk of chest infection and time to first mobilization (Guay et al., 2018), and are associated with reduced hospital length of stay and health system cost (Hamilton et al., 2019). Health Quality Ontario recommends PNBs as a quality standard for multimodal analgesia in patients with hip fracture (Health Quality Ontario, 2017).
Because early pain control can meaningfully alter downstream outcomes, suboptimal analgesia represents a missed opportunity to improve patient trajectories. Yet despite strong evidence and CAEP-endorsed recommendations supporting early regional anesthesia for hip fractures (Ritcey et al., 2016), fewer than 5 out of every 100 patients hospitalized with hip fracture receive a PNB (Neuman et al., 2020), highlighting a clear and actionable gap in care.
It’s not you, it’s me (i.e., you, the reader…)
That gap in care likely has far more to do with providers and institutions than with patients themselves. A 2022 population-based cross-sectional study by McGinn and colleagues demonstrated that 86% of variation in PNB receipt among hip fracture patients was not explained by patient-level factors, but rather varied six-fold depending on the hospital and anesthetist providing care.
While McGinn et al. examined anesthesiologist-delivered blocks, PNBs are well within the scope of emergency medicine practice. The barrier may be limited training, lack of confidence, or uncertainty around which block to perform.
Let’s fix that.
This month, we break down the two most commonly used fascia iliaca block approaches:
-
Infra-Inguinal Fascia Iliaca Block (IIFI)
-
Supra-Inguinal Fascia Iliaca Block (SIFI)
Our goal is to clarify the differences and help you decide which block best fits your practice.
You may recall Dr. Gilbertson’s excellent PoCUS Pearl from May 2025 on the SIFI block. This month’s pearl builds on that foundation while introducing an additional option you can consider at the bedside.
What are these blocks?
-
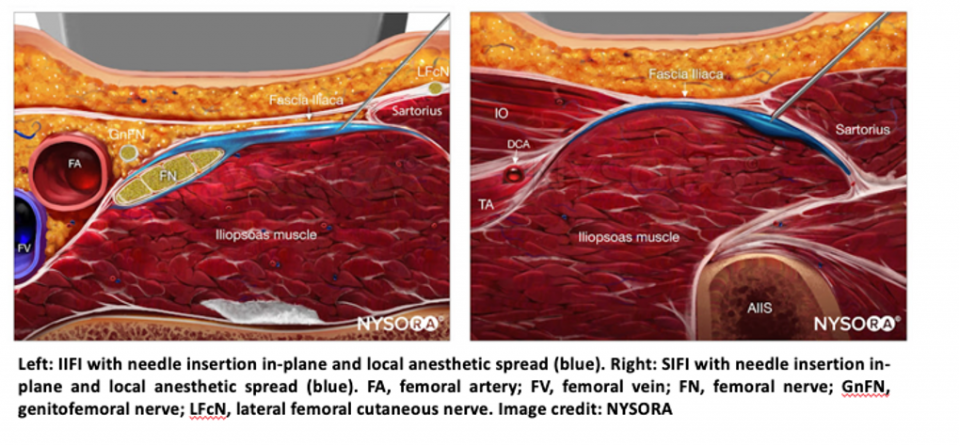
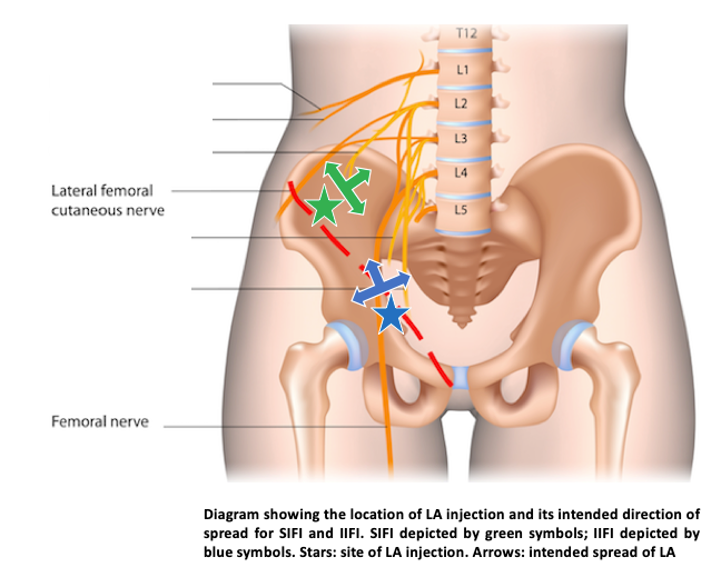
The fascia iliaca block delivers local anesthetic into the plane between the fascia iliaca and the iliacus muscle, where the femoral nerve (FN) and lateral femoral cutaneous nerve (LFCN) run.
-
A large volume of local anesthetic spreads along this fascial plane, allowing blockade of multiple nerves with a single injection.
-
Compared with a femoral nerve block, fascia iliaca blocks enhance safety by permitting injection at a distance from both the nerve and vascular structures, reducing the risk of neural or vascular injury.
SIFI vs IIFI
-
IIFI:
-
Relies on cephalad spread of local anesthetic.
-
Below the inguinal ligament, the LFCN exits the fascia iliaca plane and the femoral nerve begins branching, leading to variable LFCN blockade (Ramlogan & Uppal, 2024).
-
-
SIFI:
-
Places local anesthetic more proximally, where the femoral nerve remains unbranched and the FN and LFCN lie closer together.
-
In addition to FN and LFCN blockade, SIFI may capture the sensory distribution of the obturator nerve (ON), resulting in enhanced analgesia.
-
-
Motor effects:
-
Both approaches can cause quadriceps weakness.
-
The degree of weakness is typically less pronounced with SIFI.
-
Setting up your block
Equipment
You will need:
-
Echogenic nerve block needle (or a 20G or 22G spinal needle)
-
50-cc syringe or two 20-cc syringes
-
Syringe extension tubing
-
Chlorhexidine prep applicators
-
Sterile ultrasound gel
-
Ultrasound probe cover
-
Sterile gloves
-
Sterile drape and towels
-
Bandage or gauze
-
A helper to inject local anesthetic while you maintain probe and needle control
Local anesthetic
-
30–40 cc of bupivacaine 0.25% or ropivacaine 0.5%
-
Consider formulations with epinephrine to reduce the risk of local anesthetic systemic toxicity (LAST).
-
A brief aside on volume:
-
The optimal volume for fascia iliaca blocks has not been definitively established. Current literature supports 30–40 cc (Major & Narayanan, 2023).
-
Because these are fascial plane blocks, larger volumes are required to achieve spread along the plane rather than focal nerve deposition.
-
Dosing should always be individualized based on patient weight and comorbidities.
Ultrasound machine
-
High-frequency linear probe with a “nerve” preset selected
Performing the block
|
SIFI |
IIFI |
|
|---|---|---|
|
Patient |
Bed flat, patient supine, leg extended and externally rotated (if patient can tolerate) |
Bed flat, patient supine |
|
Probe |
Lateral edge of probe over patient’s ASIS and medial edge pointed towards the umbilicus, obliquely (image c, below). 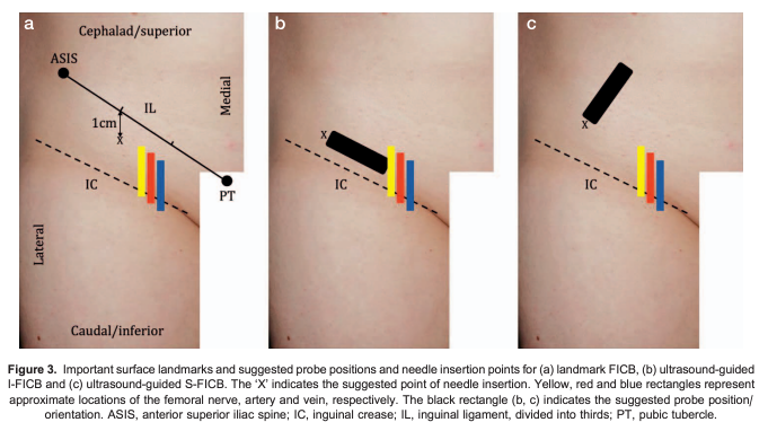 Image credit: Major and Narayanan, 2023 |
Probe transverse, just distal to the inguinal ligament, over the femoral crease (image b, below). |
|
Anatomic |
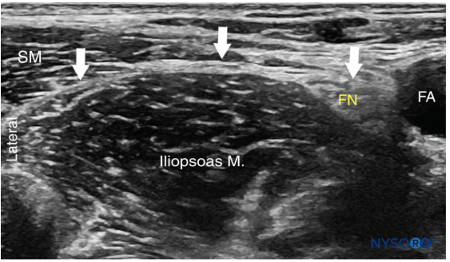
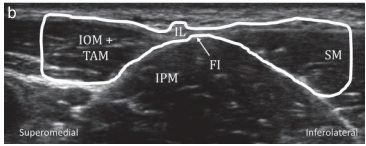
Find your “bowtie” sign formed by the sartorius muscle (SM) and internal oblique muscle (IOM) overlying the iliacus or iliopsoas muscle (IPM; see image below).
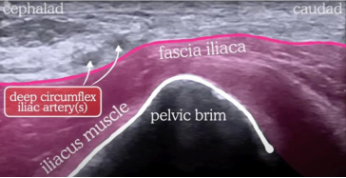
Visualize the deep circumflex iliac artery (DCIA), and avoid this area with your needle. The hyperechoic line overlying the iliacus muscle is your target, the fascia iliaca.
|
Identify the femoral artery, then slide laterally until you obtain the following view. The hyperechoic line overlying the iliopsoas is your target, the fascia iliaca.
|
|
Needle |
In-plane with ultrasound probe, directed inferior to superior. Insert your needle until just underneath the fascia iliaca (you may feel a “pop” as you pierce the fascia iliaca). |
In-plane with ultrasound probe. Advance the needle until just underneath the fascia iliaca. |
|
Local |
Have your helper inject a small volume of local anesthetic and look for hydrodissection along the fascial plane. If correctly placed, local anesthetic should spread linearly along and underneath the fascial plane. An additional clue that you are in the correct fascial plane is that your local anesthetic should displace the deep circumflex iliac artery anteriorly (i.e., nearfield). If in the correct position, inject your total volume of local anesthetic. |
Have your helper inject a small volume of local anesthetic and look for hydrodissection along the fascial plane. If correctly placed, local anesthetic should spread linearly along and underneath the fascial plane. If in the correct position, inject your total volume of local anesthetic. |
|
Contraindications |
Patient refusal, local anesthetic allergy, infection at injection site. Note that anticoagulation is not necessarily a contraindication to this procedure. As always, weigh the risks and benefits on a case-by-case basis. |
Patient refusal, local anesthetic allergy, infection at injection site. Note that anticoagulation is not necessarily a contraindication to this procedure. As always, weigh the risks and benefits on a case-by-case basis. |

Complications…LAST
Because these blocks require large volumes of local anesthetic, vigilance for LAST is essential.
-
Early symptoms: perioral numbness, metallic taste, dizziness, tinnitus
-
Severe manifestations: confusion, seizures, hypotension, cardiac arrest
Management is beyond the scope of this article. Core principles include stopping the injection, calling for help, initiating resuscitation, and administering lipid emulsion therapy.
Summary
-
Fascia iliaca blocks provide a safe and effective alternative to traditional femoral nerve blocks for hip fracture analgesia.
-
Key differences between IIFI and SIFI include:
-
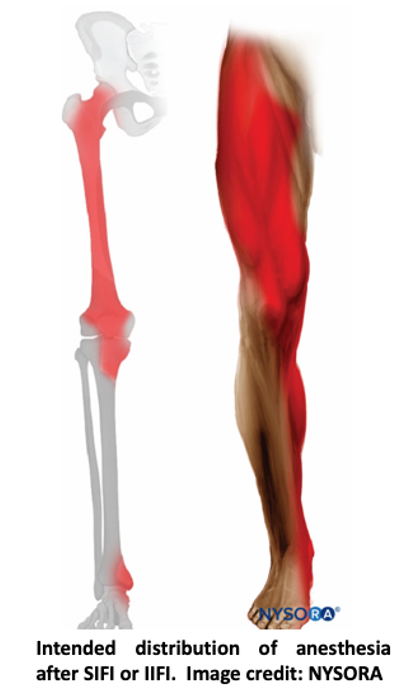
Nerves targeted: FN and LFCN (IIFI) versus FN, LFCN, and potentially ON (SIFI)
-
Motor effects: relative quadriceps sparing with SIFI
-
-
Both blocks are well within the scope of emergency medicine practice and represent a meaningful opportunity to improve patient outcomes.
Supplemental material
- Dr Ki-Jinn Chin’s and Jeff Gadsden’s YouTube videos on fascia iliaca blocks
References
- Francis J Delirium in older patients. J Am Geriatr Soc. 1992;40829- 838
- Guay J, Kopp S. Peripheral nerve blocks for hip fractures in adults. Cochrane Database of Systematic Reviews 2020, Issue 11. Art. No.: CD001159. DOI: 10.1002/14651858.CD001159.pub3. Accessed 02 December 2025.
- Guay, J., Parker, M. J., Griffiths, R., & Kopp, S. L. (2018). Peripheral Nerve Blocks for Hip Fractures: A Cochrane Review. Anesthesia and analgesia, 126(5), 1695–1704. https://doi.org/10.1213/ANE.0000000000002489
- Hamilton, G. M., Lalu, M. M., Ramlogan, R., Bryson, G. L., Abdallah, F. W., McCartney, C. J. L., & McIsaac, D. I. (2019). A Population-based Comparative Effectiveness Study of Peripheral Nerve Blocks for Hip Fracture Surgery. Anesthesiology, 131(5), 1025–1035. https://doi.org/10.1097/ALN.0000000000002947
- Hayashi, M., Yamamoto, N., Kuroda, N., Miura, T., Kamimura, Y., & Shiroshita, A. (2024). Peripheral nerve blocks in the preoperative management of hip fractures: A systematic review and network meta-analysis. Annals of Emergency Medicine, 83(6), 522–538. https://doi.org/10.1016/j.annemergmed.2024.01.006
- Health Quality Ontario. (2017). Hip fracture: Quality standard — Quality statement 3: Multimodal analgesia. Retrieved December 2, 2025, from
https://www.hqontario.ca/Evidence-to-Improve-Care/Quality-Standards/View-all-Quality-Standards/Hip-Fracture/Quality-Statement-3-Multimodal-Analgesia - Major, J., & Narayanan, M. (2023). Fascia iliaca compartment block: An update. Anaesthesia Tutorial of the Week. World Federation of Societies of Anaesthesiologists. https://www.wfsahq.org/resources/anaesthesia-tutorial-of-the-week/
- McGinn, R., et al. (2022). Hospital-, anaesthetist-, and patient-level variation in peripheral nerve block utilisation for hip fracture surgery: A population-based cross-sectional study. British Journal of Anaesthesia, 128(1), 198–206. https://doi.org/10.1016/j.bja.2021.10.019
- Morrison, RS & Siu, AL. (2025). Hip fracture in older adults: Epidemiology and medical management. In UpToDate. Retrieved November 21, 2025, from https://www.uptodate.com/contents/hip-fracture-in-older-adults-epidemiology-and-medical-management?search=hip%20fracture%20elderly&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2
- Neuman, M. D., Elkassabany, N. M., Ochroch, J., Newcomb, C., Brensinger, C., Mehta, S., Gaskins, L. J., & Lane-Fall, M. B. (2020). Nerve block use after hip fracture versus elective hip or knee arthroplasty: Retrospective analysis. Journal of the American Geriatrics Society, 68(4), 835–840. https://doi.org/10.1111/jgs.16362
- (n.d.). Ultrasound-guided fascia iliaca block. Retrieved November 24, 2025, from https://www.nysora.com/topics/regional-anesthesia-for-specific-surgical-procedures/lower-extremity-regional-anesthesia-for-specific-surgical-procedures/ultrasound-guided-fascia-iliaca-block/
- Ramlogan, R., & Uppal, V. (2024). Hip fracture analgesia: How far ahead are we? Canadian Journal of Anesthesia, 71, 692–697. https://doi.org/10.1007/s12630-023-02536-3
- Ritcey, B., Pageau, P., Woo, M. Y., & Perry, J. J. (2016). Regional nerve blocks for hip and femoral neck fractures in the emergency department: A systematic review. Canadian Journal of Emergency Medicine, 18(1), 37–47.
- Sala, A., Vitali, A., Remelli, F., Zurlo, A. and Volpato, S. 2022. Delirium in hip fractured patients. JOURNAL OF GERONTOLOGY AND GERIATRICS. 71, 1 (Sep. 2022), 8-14. DOI:https://doi.org/10.36150/2499-6564-N544.
- Thompson, C., Brienza, V. J. M., Sandre, A., Caine, S., Borgundvaag, B., & McLeod, S. (2018). Risk factors associated with acute in-hospital delirium for patients diagnosed with a hip fracture in the emergency department. Canadian Journal of Emergency Medicine, 21(3), 343–350. https://doi.org/10.1017/cem.2018.383