
Every emergency physician associates influenza with fever. But occasionally, children with influenza present at the opposite end of the spectrum.n During a single influenza season, CHEO encountered six children with laboratory-confirmed influenza who all presented with hypothermia. Several had associated neurologic or muscular manifestations, while others appeared surprisingly well despite markedly low temperatures.
Although uncommon, hypothermia is a recognized manifestation of severe influenza and may be an early marker of systemic illness. This case series reviews six pediatric cases and discusses the evidence behind this unusual presentation and its implications for emergency clinicians.
TL/DR Summary;
- Influenza does not always cause fever.
- Hypothermia is an uncommon but recognized presentation of influenza, particularly in children with more severe disease.
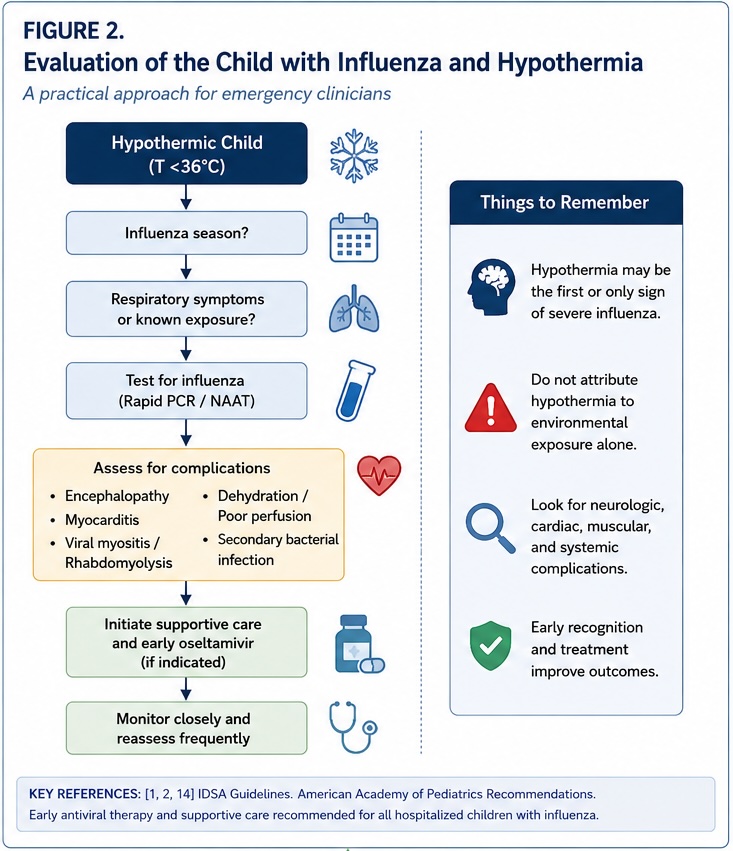
- Children presenting with influenza and hypothermia should be assessed carefully for complications including dehydration, myositis, myocarditis, encephalopathy, rhabdomyolysis, and secondary bacterial infection.
- Supportive care remains the cornerstone of management for hospitalized children with influenza.
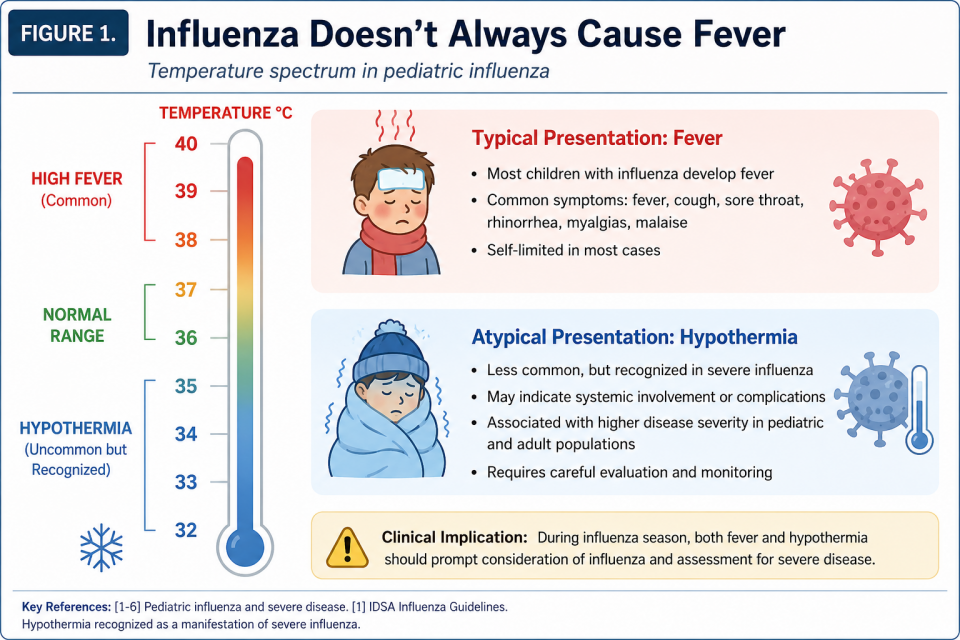
Influenza Doesn’t Always Cause Fever
Influenza remains one of the leading causes of pediatric emergency department visits and hospitalizations each winter. While most children experience a self-limited illness characterized by fever, cough, rhinorrhea, and malaise, the clinical spectrum is remarkably broad. Disease severity ranges from mild upper respiratory tract infection to respiratory failure, encephalopathy, myocarditis, rhabdomyolysis, and multi-organ dysfunction. [1–6]
Fever is so characteristic of influenza that clinicians often use its absence to lower their suspicion for infection. Yet hypothermia has long been recognized as an atypical manifestation of severe influenza and other forms of sepsis. The Infectious Diseases Society of America (IDSA) specifically identifies hypothermia as a potential feature of severe influenza, particularly when accompanied by complications such as myocarditis, encephalopathy, rhabdomyolysis, or shock.¹
Although pediatric literature largely focuses on fever as the defining clinical feature of influenza, hypothermia has been reported in fatal pediatric influenza and is associated with severe systemic illness.[2–6]
Adult data tells a similar story. Hypothermia during influenza infection has been associated with increased illness severity, ICU admission, delayed antimicrobial therapy, and increased mortality.[7–13] While uncommon, it should not be dismissed as a benign physiologic finding.
During one influenza season, we encountered six children with laboratory-confirmed influenza who all presented with hypothermia. Although each child’s presentation differed, together these cases illustrate that hypothermia may represent another manifestation of significant influenza infection rather than an unrelated abnormal vital sign.
Six Cases of Influenza-Associated Hypothermia
Case 1: Influenza A with profound hypothermia and leukopenia
Patient: 5-year-old female Lowest temperature: 33.3°C
A previously healthy five-year-old girl initially developed two days of fever before her parents recorded an unexpectedly low temperature of 33.3°C at home. Upon arrival to the emergency department her temperature remained profoundly low at 34.2°C.
Despite significant hypothermia, she appeared surprisingly well. She was alert, interactive, and demonstrated normal perfusion despite sinus bradycardia. Point-of-care ultrasound showed normal cardiac function.
Investigations revealed leukopenia (WBC 3.8 ×10⁹/L), severe neutropenia (ANC 0.6 ×10⁹/L), mildly elevated D-dimer, and a respiratory viral panel positive for Influenza A. Blood cultures remained negative.
She received active forced-air warming, warmed intravenous fluids, empiric ceftriaxone while awaiting cultures, and oseltamivir. Her temperature normalized within eight hours and she was discharged after forty-eight hours of observation.
Children with profound hypothermia may initially appear deceptively well. Even in clinically reassuring patients, significant hypothermia warrants evaluation for serious infectious and systemic complications.
Case 2: Influenza B with Orthostatic Hypotension, Urticaria, and Hypothermia
Patient: 13-year-old female Lowest temperature: 36.1°C
A previously healthy 13-year-old girl presented with presyncope, exertional dyspnea, diffuse urticaria, and malaise after several days of biphasic fever (maximum 40°C), productive cough, odynophagia, and laryngitis. She had recently recovered from varicella infection.
On arrival she appeared pale and mildly hypothermic (36.1°C) with orthostatic hypotension (88/48 mmHg sitting, improving to 100/60 mmHg supine). She remained hemodynamically stable without respiratory distress.
Laboratory investigations demonstrated leukopenia (WBC 2.7 × 10⁹/L), thrombocytopenia, mild transaminitis, elevated LDH, and a low CRP. Respiratory viral testing was positive for Influenza B. Chest radiography demonstrated mild bilateral perihilar thickening with lower lobe opacities. ECG was normal.
She received intravenous fluids, cetirizine, intramuscular epinephrine for suspected anaphylaxis, empiric ampicillin (later discontinued following viral confirmation), and oseltamivir. Orthostatic symptoms gradually resolved, and she was discharged after seven days.
Influenza can produce significant autonomic dysfunction and circulatory instability that mimics bacterial sepsis or even anaphylaxis. During influenza season, viral infection should remain on the differential for children presenting with unexplained hypotension or presyncope.
Case 3: Influenza A with Dehydration and Hypothermia
Patient: 3-year-old female Lowest temperature: 35.1°C
A previously healthy three-year-old girl developed four days of fever followed by increasing fatigue, reduced oral intake, tachypnea, oliguria, and cold, clammy skin. She also had cough and nasal congestion.
On presentation she was hypothermic (35.1°C), tired but arousable, with preserved oxygenation and mild tachypnea. Examination demonstrated mild cervical lymphadenopathy and focal right-sided wheeze. Chest radiography showed perihilar thickening and bronchial wall thickening consistent with viral lower respiratory tract infection. Respiratory viral testing confirmed Influenza A.
After receiving intravenous fluid resuscitation and passive rewarming, her hydration status, perfusion, and level of alertness improved rapidly. She returned to baseline within ten hours and was discharged home.
In young children, hypothermia may reflect significant dehydration and reduced physiologic reserve rather than overwhelming septic shock. Restoration of intravascular volume often results in rapid normalization of temperature and perfusion.
Case 4: Influenza A Presenting as Viral Myositis
Patient: 10-year-old female Lowest temperature: 35.6°C
A previously healthy ten-year-old girl presented with abrupt onset of severe bilateral calf pain after three days of mild influenza-like symptoms including headache, cough, and otalgia. She was unable to walk comfortably because of pain.
On examination she was hypothermic (35.6°C), pale, and had mottling of the hands and feet. There was marked calf tenderness without swelling, weakness, or neurologic deficit.
Laboratory investigations revealed an elevated creatine kinase (781 U/L) with normal renal function and electrolytes. Respiratory viral testing confirmed Influenza A.
She was managed conservatively with oral hydration, rest, analgesia, and oseltamivir. Symptoms improved progressively, and she was discharged home with return precautions.
Viral myositis is a well-recognized complication of influenza and frequently presents with bilateral calf pain and refusal to walk. Hypothermia should prompt clinicians to consider associated systemic involvement while excluding evolving rhabdomyolysis.
Case 5: Influenza A with Viral Myositis and Refusal to Walk
Patient: 5-year-old male Lowest temperature: 35.9°C
A previously healthy five-year-old boy developed four days of high fever followed by sudden refusal to walk because of bilateral leg pain.
On arrival he was mildly hypothermic (35.9°C), sleepy but easily arousable, and uncomfortable with passive movement of both lower extremities. There was no joint swelling, erythema, or focal neurologic deficit. Point-of-care ultrasound of the hip demonstrated only a small effusion.
Investigations revealed mild leukopenia, neutropenia, normal inflammatory markers, CK elevation (610 U/L), and a positive respiratory viral panel for Influenza A. Radiographs were unremarkable.
Following hydration, analgesia, and supportive care, his symptoms improved significantly. Repeat CK remained stable, and he was discharged after approximately eight hours of observation.
Influenza-associated myositis can closely mimic septic arthritis or osteomyelitis. Bilateral symptoms, normal inflammatory markers, and modest CK elevation should increase suspicion for viral myositis.
Case 6: Influenza A and Epstein-Barr Virus Co-infection
Patient: 2-year-old female Lowest temperature: 35.8°C
A previously healthy two-year-old girl presented with two weeks of persistent fever, cough, nasal congestion, rash, and reduced oral intake despite treatment with amoxicillin and azithromycin.
On examination she was hypothermic (35.8°C), listless but interactive, with diffuse blanching maculopapular rash, bilateral conjunctival injection, and mild cervical lymphadenopathy. Perfusion remained normal.
Laboratory investigations demonstrated mild leukopenia with otherwise reassuring inflammatory markers and normal hepatic and renal function. Respiratory viral testing was positive for Influenza A, while serology confirmed acute Epstein-Barr virus coinfection. Chest radiography demonstrated inflammatory lower respiratory tract changes without focal bacterial pneumonia.
Antibiotics were discontinued, and she received intravenous fluids, passive rewarming, and oseltamivir. She improved clinically and was discharged the same day.
Influenza may coexist with other viral infections, creating clinical pictures that mimic Kawasaki disease or invasive bacterial infection. Positive influenza testing should not prevent clinicians from considering alternative or concurrent diagnoses when the presentation is atypical.
Discussion
This case series describes six pediatric patients who presented over a single influenza season with laboratory-confirmed influenza and concurrent hypothermia, frequently accompanied by neurologic and/or muscular manifestations. Together, these cases suggest that hypothermia may be more common in pediatric influenza, and more clinically meaningful than previously recognized. They also reinforce the importance of careful assessment of vital signs and support treating hypothermia as a potential marker of severe disease, particularly in young children.
Hypothermia has been documented in severe and fatal pediatric influenza, often in association with encephalopathy, shock, myocarditis, rhabdomyolysis, and other forms of multi-organ dysfunction. The Infectious Diseases Society of America (IDSA) specifically recognizes hypothermia as a potential manifestation of severe influenza, particularly when accompanied by complications such as myocarditis, rhabdomyolysis, or encephalopathy.[1] Similarly, the American Academy of Pediatrics (AAP) identifies children younger than five years as being at highest risk for hospitalization and severe outcomes, with neurologic complications, including encephalopathy and seizures, occurring more frequently in this population, particularly among those who are unimmunized.[2][3]
The clinical spectrum of influenza-associated hypothermia is broad, ranging from transient, self-limited episodes to persistent hypothermia associated with critical illness. In our series, hypothermia occurred alongside dehydration, viral myositis, autonomic dysregulation, and viral co-infection, highlighting the heterogeneous nature of this presentation. Several patients also demonstrated neurologic or muscular manifestations, complications that are increasingly recognized as important contributors to morbidity and mortality in pediatric influenza.[3][4][5][6][7] Hypothermia in these settings may reflect cytokine dysregulation, altered thermoregulation, or direct viral effects on the central nervous system.[8][9]
Animal models provide further insight into the underlying physiology, demonstrating that influenza infection can induce hypothermia through a reduction in the hypothalamic thermoregulatory set point, independent of reduced food intake.[8] Young children may be particularly susceptible because of their high surface-area-to-mass ratio and limited thermogenic reserve, reducing their ability to maintain normothermia during systemic illness.[10]
Observational studies in both pediatric and adult populations have consistently shown that hypothermia is associated with worse clinical outcomes, including multi-organ failure, shock, severe neurologic involvement, ICU admission, mechanical ventilation, and death.[2][11][12][13] Although hypothermia itself may not directly cause these outcomes, its presence should be viewed as a warning sign that warrants careful evaluation for underlying complications.
For emergency clinicians, the detection of hypothermia in a child with suspected or confirmed influenza should prompt assessment for severe complications including encephalopathy, myocarditis, viral myositis, rhabdomyolysis, dehydration with poor perfusion, and secondary bacterial infection. Current IDSA and AAP guidelines recommend early initiation of antiviral therapy (e.g., oseltamivir*) and appropriate supportive care for all hospitalized children with influenza, regardless of presenting temperature.[1][2][14] Finally, while outside the scope of this case series, vaccination remains the most effective strategy for preventing severe influenza, yet vaccine uptake continues to be suboptimal among children who experience severe or fatal disease.[5][6][7]
* (Note: the editor of the EMOttawa Blog has previously written about controversies associated with oseltamivir in the past, read more here for an alternative opinion)
Conclusion
Hypothermia is an uncommon but clinically important presentation of pediatric influenza. In this case series, it occurred alongside a diverse range of clinical manifestations—including dehydration, viral myositis, autonomic dysfunction, and viral co-infection—highlighting that influenza-associated hypothermia is not limited to a single disease phenotype. Rather, it may represent an early marker of more severe systemic or neuroinflammatory illness.
During influenza season, hypothermia should not reassure clinicians or lower suspicion for influenza. Instead, it should prompt consideration of influenza in the differential diagnosis while triggering a careful evaluation for serious complications. Early recognition, timely initiation of antiviral therapy, and guideline-directed supportive care remain the cornerstones of management.[1][2][14]
References
- Clinical Practice Guidelines by the Infectious Diseases Society of America: 2018 Update on Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management of Seasonal Influenzaa. Uyeki TM, Bernstein HH, Bradley JS, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2019;68(6):e1-e47. doi:10.1093/cid/ciy866.
- Recommendations for Prevention and Control of Influenza in Children, 2023-2024. Pediatrics. 2023;152(4):e2023063773. doi:10.1542/peds.2023-063773.
- Prevalence, Risk Factors, and Outcomes of Influenza-Associated Neurologic Complications in Children. Antoon JW, Hall M, Herndon A, et al. The Journal of Pediatrics. 2021;239:32-38.e5. doi:10.1016/j.jpeds.2021.06.075.
- Influenza-Associated Deaths among Children in the United States, 2003–2004. Bhat N, Wright JG, Broder KR, et al. The New England Journal of Medicine. 2005;353(24):2559-67. doi:10.1056/NEJMoa051721.
- Pediatric Influenza-Associated Encephalopathy and Acute Necrotizing Encephalopathy – United States, 2024-25 Influenza Season. Fazal A, Harker EJ, Neelam V, et al. MMWR. Morbidity and Mortality Weekly Report. 2025;74(36):556-564. doi:10.15585/mmwr.mm7436a1.
- Reports of Encephalopathy Among Children With Influenza-Associated Mortality – United States, 2010-11 Through 2024-25 Influenza Seasons. Fazal A, Reinhart K, Huang S, et al. MMWR. Morbidity and Mortality Weekly Report. 2025;74(6):91-95. doi:10.15585/mmwr.mm7406a3.
- Influenza-Associated Acute Necrotizing Encephalopathy in US Children. Silverman A, Walsh R, Santoro JD, et al. JAMA. 2025;:2836871. doi:10.1001/jama.2025.11534.
- Hypothetical Pathophysiology of Acute Encephalopathy and Encephalitis Related to Influenza Virus Infection and Hypothermia Therapy. Yokota S, Imagawa T, Miyamae T, et al. Pediatrics International : Official Journal of the Japan Pediatric Society. 2000;42(2):197-203. doi:10.1046/j.1442-200x.2000.01204.x.
- Combined Therapy With Hypothermia and Anticytokine Agents in Influenza a Encephalopathy. Munakata M, Kato R, Yokoyama H, et al. Brain & Development. 2000;22(6):373-7. doi:10.1016/s0387-7604(00)00169-8.
- Pediatric Hypothermia: An Ambiguous Issue. Singer D. International Journal of Environmental Research and Public Health. 2021;18(21):11484. doi:10.3390/ijerph182111484.
- Severe Influenza: Overview in Critically Ill Patients. Sarda C, Palma P, Rello J. Current Opinion in Critical Care. 2019;25(5):449-457. doi:10.1097/MCC.0000000000000638.
- Outcomes of Influenza A(H1N1)pdm09 Virus Infection: Results From Two International Cohort Studies. Lynfield R, Davey R, Dwyer DE, et al. PloS One. 2014;9(7):e101785. doi:10.1371/journal.pone.0101785.
- Epidemiology, Clinical Characteristics, and Outcomes of Influenza-Associated Hospitalizations in US Children Over 9 Seasons Following the 2009 H1N1 Pandemic. Kamidani S, Garg S, Rolfes MA, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2022;75(11):1930-1939. doi:10.1093/cid/ciac296.
- Recommendations for Prevention and Control of Influenza in Children, 2022-2023. Pediatrics. 2022;150(4):e2022059275. doi:10.1542/peds.2022-059275.
