Contrast media agents are among the most commonly administered pharmaceutical compounds worldwide, improving diagnostic accuracy across a wide range of imaging studies and enabling angiographic procedures. In Canada alone, an estimated 2.7 million contrast-enhanced computed tomography (CT) scans were performed in 2019.¹ As a result, contrast media is nearly ubiquitous in emergency medicine (EM). However, like any medication, contrast media can cause adverse reactions that pose unique diagnostic and management challenges in the emergency department.
Recently updated 2025 Canadian, American, and European guidelines, published by the Canadian Association of Radiologists (CAR)/Canadian Society of Allergy and Clinical Immunology (CSACI), the American College of Radiology (ACR)/American Academy of Allergy, Asthma, and Immunology (AAAAI), and the European Society of Urogenital Radiology (ESUR), outline a major shift in the prevention and management of contrast media hypersensitivity reactions (HRs), commonly referred to as allergic reactions.2–6 These recommendations have important implications for both emergency medicine practice and departmental protocols.
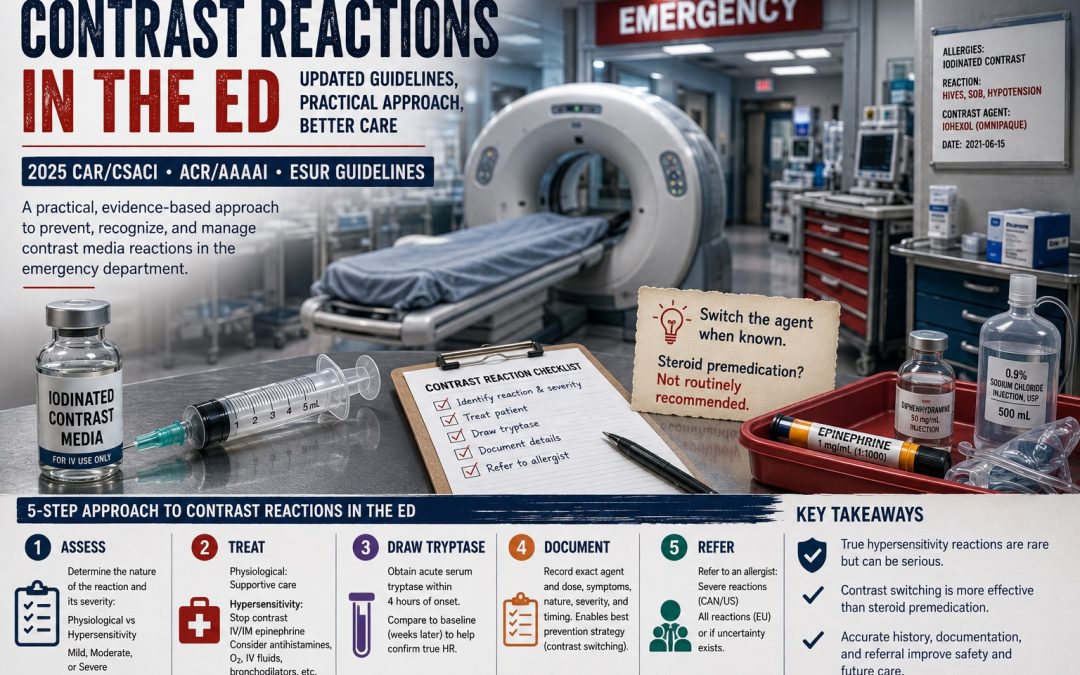
This post reviews the current evidence and provides a practical, guideline-based approach to preventing, recognizing, and managing contrast media reactions in the emergency department.
Background
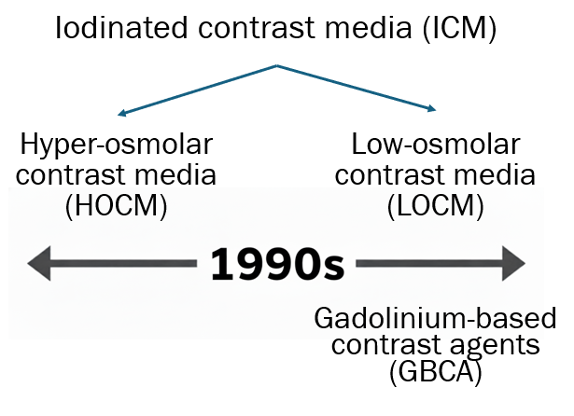
There are two main types of contrast media used for imaging in the emergency department (ED), each consisting of multiple agents with distinct chemical structures.
- Iodinated contrast media (ICM) for computed tomography (CT)
- Hyperosmolar contrast media (HOCM) were the predominant agents from the 1950s through the 1990s. They were largely replaced in the 1990s by low-osmolar contrast media (LOCM), which are now used almost universally.
- Gadolinium-based contrast agents (GBCA) for magnetic resonance imaging (MRI)
- GBCAs have been used in clinical practice since the 1990s.
The remainder of this post focuses primarily on hypersensitivity reactions to iodinated contrast media used for CT imaging. Reactions to GBCAs are discussed briefly near the end.
Iodine, Seafood and Contrast
Although topical iodine-containing antiseptics can cause contact dermatitis, iodine itself is not an allergen. It is naturally present in the human body, routinely added to table salt in North America, and is essential for normal physiological function. Likewise, the IgE-mediated allergic reaction to shellfish is directed against tropomyosin—not iodine—despite this common misconception. Accordingly, patients with self-reported or IgE-confirmed seafood allergy are not at increased risk of contrast media hypersensitivity reactions compared with the general population.
Bottom line: Iodine is not an allergen, and a history of seafood or shellfish allergy should not influence decision-making regarding the administration of iodinated contrast media.⁴
Pathophysiology
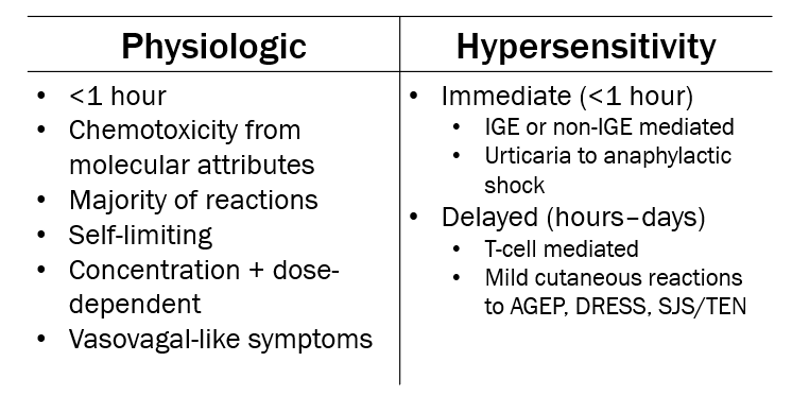
There are 2 types of contrast reactions, physiological and hypersensitivity (AKA allergic). It is very important to distinguish between the 2 types as this will significantly impact management in the ED.
The 2025 ACR Manual on Contrast Media further classifies both physiological and hypersensitivity reactions into three severity categories: mild, moderate, and severe.⁷ This widely used classification system provides a practical framework for assessing and managing contrast reactions in the emergency department.
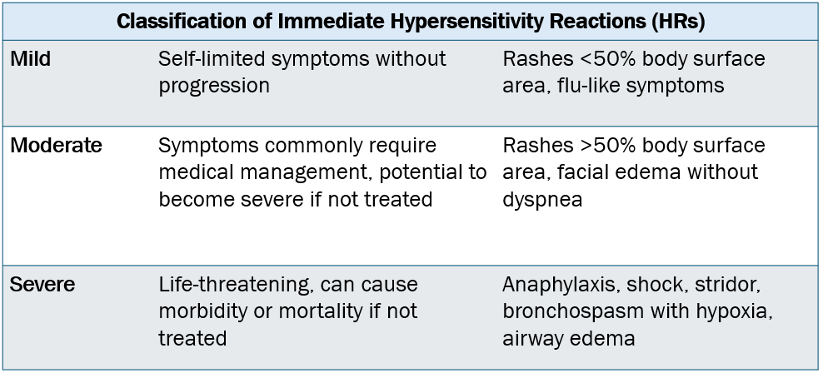
Adapted from the 2025 ACR manual on contrast media
All 3 of the 2025 guidelines highlight the importance of trying to differentiate the type and severity of previous and current reactions to inform next steps.
Physiological Reactions
Physiological reactions occur as a result of the chemotoxic effects of contrast media and are not true allergic reactions, although patients may describe them as such. They account for the majority of contrast reactions, are almost always self-limiting, and often resemble vasovagal reactions.
Distinguishing physiological reactions from hypersensitivity reactions is important, as management differs substantially. Patients with a history of physiological reactions do not require preventative treatment before future contrast administration beyond routine monitoring. If a physiological reaction does occur in the ED, management consists of observation and supportive care.
Hypersensitivity Reactions
True hypersensitivity reactions (HRs) to contrast media are uncommon. A large South Korean study of more than 11.7 million low-osmolar contrast media (LOCM) administrations reported an immediate HR rate of just 0.38%, with severe reactions occurring in only 0.02% of cases. Delayed HRs were even less common, occurring in 0.05% of administrations.⁸
Despite their rarity, contrast media HRs present a unique challenge in the emergency department, where patient acuity, time-sensitive imaging, and the necessity of contrast for certain diagnoses often limit management options. Traditionally, prevention has relied on routine premedication protocols, most commonly using corticosteroids. However, the 2025 Canadian, American, and European guidelines represent a significant shift away from this longstanding practice.
Preventing Hypersensitivity Reactions in the ED
Risk Factors
The only clinically important risk factor for a contrast media hypersensitivity reaction (HR) is a history of a previous contrast media HR. No additional screening is routinely recommended. This again underscores the importance of obtaining details of any prior reaction to distinguish a true HR from a physiological reaction, as this distinction directly influences management.
Premedication
Premedication protocols using antihistamines and corticosteroids have long been the standard approach to preventing recurrent HRs. Common regimens include traditional 12–13-hour oral corticosteroid protocols or accelerated intravenous (IV) corticosteroid protocols used in emergency settings.
Antihistamines
Evidence supports the use of antihistamines to reduce the risk of recurrent HRs, particularly in patients with a history of mild reactions. Accordingly, antihistamine premedication is recommended for patients with previous mild-to-moderate HRs. Although evidence is more limited for patients with prior severe reactions, antihistamines remain reasonable when the potential benefits are felt to outweigh the risks.
Antihistamines should be administered approximately 1 hour before contrast administration. The CSACI recommends second- or third-generation antihistamines, such as cetirizine or desloratadine, over first-generation agents such as diphenhydramine. However, many centres currently only have IV first-generation antihistamines available for patients who cannot take oral medications.
Corticosteroids
The widely used 12- and 13-hour oral corticosteroid premedication protocols originated from two studies published in 1981 and 1987 involving hyperosmolar contrast media (HOCM), which were associated with substantially higher rates of HRs and have not been routinely used since the 1990s.⁹˒¹⁰ When these protocols were later evaluated using the much safer low-osmolar contrast media (LOCM), the evidence was limited, inconsistent, and difficult to interpret because of significant methodological limitations, including non-randomized study designs, lack of control groups, and the markedly lower baseline reaction rates associated with LOCM.
The accelerated IV corticosteroid regimen commonly used in the ED is largely based on a 2017 study by Mervak et al., which demonstrated that a 5-hour IV regimen (2.5% breakthrough reaction rate) was non-inferior to the traditional 13-hour oral regimen (2.1%). Importantly, however, neither protocol eliminated moderate or severe breakthrough reactions.¹¹
More recent evidence has further challenged the routine use of corticosteroid premedication. A 2017 review combining data from three studies estimated a number needed to treat (NNT) of 56,900 to prevent a single fatal reaction.¹² In addition, systemic corticosteroids carry well-recognized risks, including hyperglycemia, psychosis, insomnia, sepsis, venous thromboembolism, and increased fracture risk. Premedication protocols may also contribute to delayed diagnosis, prolonged emergency department length of stay, and other downstream effects on patient care.¹³
Taken together, these data have led to a significant shift in recent guidelines. The 2025 CAR/CSACI guideline recommends against routine corticosteroid premedication for patients with a history of HRs of any severity to LOCM. The 2025 ACR/AAAAI consensus statement recommends considering corticosteroid premedication for patients with previous moderate HRs and continues to recommend it for those with previous severe HRs when no acceptable alternative imaging study exists, while acknowledging that the supporting evidence is of very low quality. The ESUR guideline considers corticosteroid premedication optional for patients with a prior severe reaction when the culprit contrast agent is unknown.
Contrast Switching
The widespread use of routine corticosteroid premedication has long made it the cornerstone of prophylaxis against contrast media HRs. However, the recent shift toward contrast switching has the potential to significantly change emergency medicine practice and departmental protocols. The rationale is straightforward: contrast agents differ in their chemical structures, and when the culprit agent is known, switching to a different agent may be the most effective strategy for preventing recurrent reactions.
Several studies support this approach. In 2021, McDonald et al. found that re-administering the same contrast agent, with or without corticosteroid premedication, did not alter reaction rates, whereas switching to a different agent significantly reduced recurrent reactions regardless of premedication use.¹⁴ Similarly, a systematic review and meta-analysis by Umakoshi et al. involving 7,155 patients found that contrast substitution reduced the risk of breakthrough reactions by 61%, while premedication had no significant effect on recurrent reaction rates.¹⁵
Overall, current evidence suggests that switching iodinated contrast agents is more effective than corticosteroid premedication when the culprit agent is known. This recommendation is supported by all three updated guidelines.
When contrast switching is indicated, the radiology department should be notified so an alternative agent with a different chemical structure can be selected based on local availability.
The key limitation is that contrast substitution is only possible if the previously administered contrast agent is known. This further emphasizes the importance of accurately documenting the specific contrast agent whenever a hypersensitivity reaction occurs.
Three Special Circumstances
Gadolinium-Based Contrast Agents (GBCA)
As with iodinated contrast media, most reactions to GBCAs are physiological rather than hypersensitivity reactions. The only clinically important risk factor is a history of a previous GBCA hypersensitivity reaction. For these patients, antihistamine premedication 1 hour before contrast administration is recommended, routine corticosteroid premedication is not, and contrast switching should be performed whenever possible.
Pediatrics
There is little pediatric-specific evidence regarding prevention of contrast media HRs. Accordingly, local experts recommend applying the same approach used in adults.
Non-Vascular Contrast Media
Although less common in the ED, contrast media may occasionally be administered via non-vascular routes, such as enteric contrast. Interestingly, both hyperosmolar and low-osmolar contrast agents continue to be used for these indications. For patients with a history of contrast media HRs, the CAR/CSACI guideline recommends against routine corticosteroid premedication and instead recommends contrast switching for both future vascular and non-vascular contrast administration.
Summary: A Practical Clinical Approach
- Previous mild or moderate HR: If the culprit contrast agent is known, notify radiology to arrange contrast substitution. If the culprit agent is unknown and switching is therefore not possible, administer a second- or third-generation antihistamine 1 hour before contrast administration. Routine corticosteroid premedication is not recommended, although the 2025 American guideline states that it may be considered for patients with previous moderate reactions.
- Previous severe HR (e.g., anaphylaxis): Discuss alternative non-contrast imaging with radiology whenever appropriate. If contrast administration is essential and the culprit agent is known, arrange contrast substitution and administer the study with close monitoring. If the culprit agent is unknown, contrast may still be administered when clinically necessary, provided appropriate personnel and resources are immediately available to recognize and manage anaphylaxis (e.g., ED, ICU, Anesthesia, or Rapid Response teams). Guideline recommendations regarding corticosteroid premedication differ: it is not recommended by the 2025 Canadian guideline, optional in the 2025 European guideline, and recommended by the 2025 American guideline.

Source: 2025 CAR/CSACI guideline6
Treating Hypersensitivity Reactions in the ED
Although true hypersensitivity reactions (HRs) to contrast media are rare, they will inevitably occur in the emergency department. Once recognized, the following stepwise approach can be used to guide management.
Step 1: Determine the Reaction Type and Severity
First, determine whether the reaction is physiological or a true hypersensitivity reaction, then classify its severity as mild, moderate, or severe. This distinction guides both acute management and future preventative strategies.
Step 2: Treat the Patient
Physiological reactions are managed with observation and supportive care. Hypersensitivity reactions should be managed according to standard allergic reaction and anaphylaxis protocols, including immediate cessation of contrast administration, intramuscular epinephrine when indicated, and consideration of adjunctive therapies such as antihistamines, supplemental oxygen, IV fluids, and bronchodilators.¹⁶
Step 3: Draw a Tryptase Level
For patients who will require outpatient allergy assessment (see Step 5), obtain an acute serum tryptase level within 4 hours of symptom onset. Although this result is unlikely to influence ED management, comparison with a baseline tryptase level obtained weeks later can help allergists determine whether the reaction represented true mast cell activation. Accurately distinguishing physiological from hypersensitivity reactions may have lifelong implications for future imaging and patient care.
Step 4: Document the Reaction Thoroughly
Documentation should include:
- The exact contrast agent and dose administered.
- The symptoms experienced.
- The nature of the reaction (physiological vs. hypersensitivity).
- The severity of the reaction.
- The timing of symptom onset.
Careful documentation has long-term value, as identifying the culprit contrast agent allows for contrast switching, currently the most effective strategy for preventing recurrent hypersensitivity reactions.
Step 5: Refer to an Allergist
The Canadian and American guidelines recommend outpatient allergy referral for patients who experience a severe contrast media HR. The European guideline recommends referral following any contrast media HR. Referral is also reasonable whenever there is uncertainty regarding the nature of the reaction or future contrast administration is anticipated.
Summary
Contrast-enhanced imaging is indispensable in emergency medicine, making patients with previous contrast reactions a common and important clinical challenge. The updated 2025 CAR/CSACI, ACR/AAAAI, and ESUR guidelines represent a significant shift in the prevention and management of contrast media hypersensitivity reactions, moving away from routine corticosteroid premedication and toward a more individualized, evidence-based approach that emphasizes accurate characterization of prior reactions and contrast switching when appropriate.
Emergency physicians are well positioned to lead these practice changes in collaboration with radiology and allergy colleagues. By adopting these updated recommendations, we can improve patient safety, reduce unnecessary treatment and delays, and optimize the care of patients requiring contrast-enhanced imaging in the ED and beyond.
References
- Macdonald DB, Hurrell C, Costa AF, et al. Canadian Association of Radiologists Guidance on Contrast Associated Acute Kidney Injury. Can Assoc Radiol J. 2022;73(3):499-514. doi:10.1177/08465371221083970
- Van Der Molen AJ, Van De Ven AAJM, Vega F, et al. Hypersensitivity reactions to contrast media: Part 1. Management of immediate and non-immediate hypersensitivity reactions in adults. Updated guidelines by the ESUR Contrast Media Safety Committee. Eur Radiol. 2025;35(11):6798-6810. doi:10.1007/s00330-025-11675-1
- Van Der Molen AJ, Van De Ven AAJM, Vega F, et al. Hypersensitivity reactions to contrast media: Part 2. Prevention of recurrent hypersensitivity reactions in adults. Updated guidelines by the ESUR Contrast Media Safety Committee. Eur Radiol. 2025;35(11):6811-6825. doi:10.1007/s00330-025-11676-0
- Wang C, Ramsey A, Lang D, et al. Management and Prevention of Hypersensitivity Reactions to Radiocontrast Media: A Consensus Statement from the American College of Radiology and the American Academy of Allergy, Asthma & Immunology. Radiology. 2025;315(2):e240100. doi:10.1148/radiol.240100
- Byrne A, Macdonald DB, Kirkpatrick IDC, et al. CAR/CSACI Practice Guidance for Contrast Media Hypersensitivity. Can Assoc Radiol J. 2025;76(3):400-416. doi:10.1177/08465371241311253
- Byrne A, Macdonald DB, Kirkpatrick IDC, et al. CAR/CSACI Practice Guidance for Contrast Media Hypersensitivity: Update for Unknown Contrast Agents. Can Assoc Radiol J. Published online December 26, 2025:08465371251401551. doi:10.1177/08465371251401551
- American College of Radiology. ACR Manual on Contrast Media. Published online 2025. Accessed October 30, 2025. https://edge.sitecorecloud.io/americancoldf5f-acrorgf92a-productioncb02-3650/media/ACR/Files/Clinical/Contrast-Manual/ACR-Manual-on-Contrast-Media.pdf
- An J, Jung H, Kwon OY, et al. Differences in Adverse Reactions Among Iodinated Contrast Media: Analysis of the KAERS Database. The Journal of Allergy and Clinical Immunology: In Practice. 2019;7(7):2205-2211. doi:10.1016/j.jaip.2019.02.035
- Greenberger PA, Patterson R, Simon R, Lieberman P, Wallace W. Pretreatment of high-risk patients requiring radiographic contrast media studies. Journal of Allergy and Clinical Immunology. 1981;67(3):185-187. doi:10.1016/0091-6749(81)90059-2
- Lasser EC, Berry CC, Talner LB, et al. Pretreatment with Corticosteroids to Alleviate Reactions to Intravenous Contrast Material. New England Journal of Medicine. 1987;317(14):845-849. doi:10.1056/NEJM198710013171401
- Mervak BM, Cohan RH, Ellis JH, Khalatbari S, Davenport MS. Intravenous Corticosteroid Premedication Administered 5 Hours before CT Compared with a Traditional 13-Hour Oral Regimen. Radiology. 2017;285(2):425-433. doi:10.1148/radiol.2017170107
- Davenport MS, Cohan RH. The Evidence for and Against Corticosteroid Prophylaxis in At-Risk Patients. Radiologic Clinics of North America. 2017;55(2):413-421. doi:10.1016/j.rcl.2016.10.012
- Berlyand Y, Fraga JA, Succi MD, et al. Impact of iodinated contrast allergies on emergency department operations. The American Journal of Emergency Medicine. 2022;61:127-130. doi:10.1016/j.ajem.2022.08.052
- McDonald JS, Larson NB, Kolbe AB, et al. Prevention of Allergic-like Reactions at Repeat CT: Steroid Pretreatment versus Contrast Material Substitution. Radiology. 2021;301(1):133-140. doi:10.1148/radiol.2021210490
- Umakoshi H, Nihashi T, Takada A, et al. Iodinated Contrast Media Substitution to Prevent Recurrent Hypersensitivity Reactions: A Systematic Review and Meta-Analysis. Radiology. 2022;305(2):341-349. doi:10.1148/radiol.220370
- Shaker MS, Wallace DV, Golden DBK, et al. Anaphylaxis—a 2020 practice parameter update, systematic review, and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) analysis. Journal of Allergy and Clinical Immunology. 2020;145(4):1082-1123. doi:10.1016/j.jaci.2020.01.017