Valvular heart disease is everywhere in emergency medicine, but it is sneaky.
We see the older patient with recurrent dyspnea whose chest radiograph is unremarkable and BNP is only mildly elevated. We see the patient in shock whose physiology never quite fits sepsis. We see syncope without an obvious cause, recurrent episodes of heart failure, pulmonary edema that seems disproportionate to the degree of systolic dysfunction, and patients whose symptoms have been blamed on everything except the diseased valve driving the presentation.
The problem isn’t that valvular heart disease is rare, it’s that we’re often not looking for it.
For many emergency physicians, focused cardiac ultrasound has become an extension of the physical exam. We routinely assess for pericardial effusions, estimate global left ventricular systolic function, evaluate for right ventricular strain, and use the IVC to help guide volume assessment.
Valve assessment, however, is often left to formal echocardiography. It feels like the domain of cardiology, filled with spectral Doppler, pressure gradients, continuity equations, valve areas, and measurements that seem unrealistic during a busy emergency department shift.
Fortunately, bedside valve assessment doesn’t have to be that complicated.
Our goal isn’t to perform a comprehensive echocardiogram or formally grade the severity of every lesion. It’s to recognize when a valve appears significantly abnormal and could plausibly explain why the patient in front of us is sick.
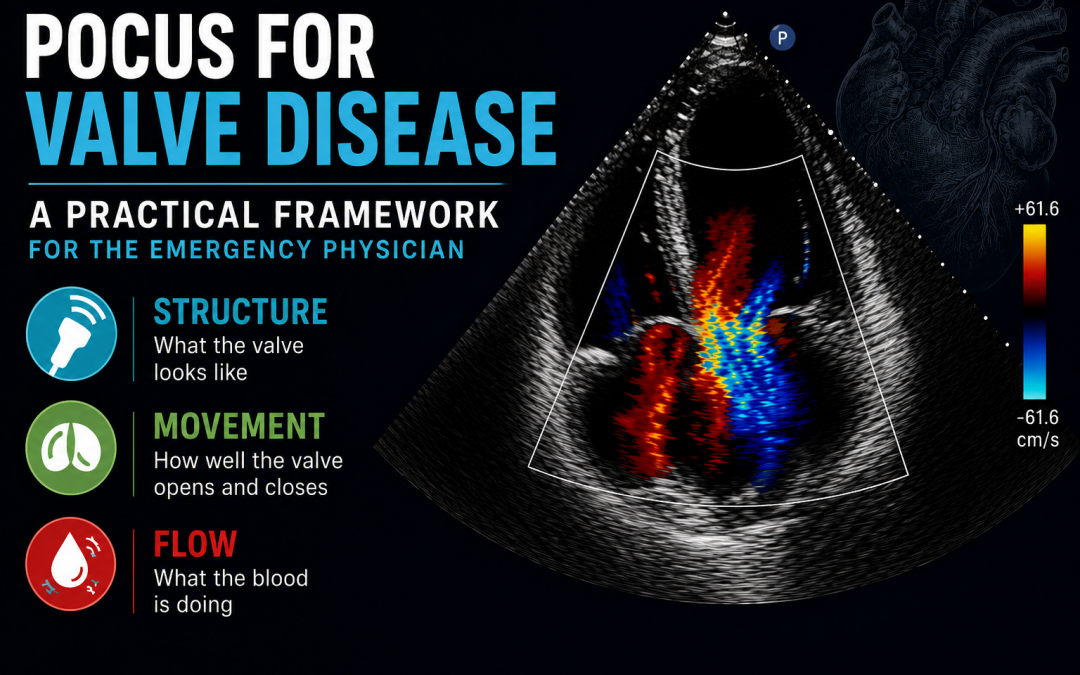
Fortunately, you can accomplish a surprising amount by answering just three questions:
- How does the valve look?
- How does it move?
- How is blood flowing across it?
Those three questions form the foundation of bedside valvular PoCUS and provide a practical framework for identifying clinically important valve disease in the emergency department.
For an in-depth guide to bedside echocardiography, check out our handbook here.
Why Emergency Physicians Should Care About Valves
Valvular heart disease is common, and it’s becoming even more common as our population ages. More than one in eight adults over the age of 75 has moderate or severe valvular disease. Even before severe disease develops, valve pathology is frequently encountered. Aortic sclerosis alone affects approximately one-quarter to one-third of adults over 65 years of age and nearly half of those older than 85.
The lesions emergency physicians are most likely to encounter include:
- Aortic stenosis
- Mitral regurgitation
- Tricuspid regurgitation
The question isn’t whether we’re seeing these patients, it’s whether we’re recognizing them.
Valvular disease rarely presents with a classic picture. Instead, patients often arrive with nonspecific complaints that overlap with countless other emergency department diagnoses, including:
- Dyspnea
- Shock
- Syncope
- Recurrent heart failure
- Undifferentiated hypotension
Unfortunately, the physical examination isn’t always enough. Murmurs may be subtle, atypical, or even absent in advanced disease. Patients with critical aortic stenosis, for example, may generate surprisingly quiet murmurs because severely reduced cardiac output produces less turbulent flow across the valve.
Similarly, our standard focused cardiac ultrasound examination often stops after evaluating:
- Pericardial effusion
- Global LV systolic function
- Right ventricular size and function
While these are all essential components of cardiac PoCUS, many important valvular lesions cannot be recognized unless we deliberately examine the valves themselves.
If we aren’t looking at the valves, we’re going to miss valve disease.
The Causes of Valve Disease You Need to Know
Although the list of valvular disorders is long, most disease encountered in emergency medicine falls into one of four broad categories:
1. Degenerative Disease
Degenerative disease is by far the most common mechanism in older adults. Common examples include:
- Calcific aortic stenosis
- Mitral annular calcification
- Degenerative mitral regurgitation
These valves gradually become thickened, increasingly echogenic, progressively less mobile, and ultimately dysfunctional.
2. Functional or Ischemic Disease
Sometimes the valve itself is structurally normal. Instead, ventricular remodeling or ischemia alters the geometry of the supporting apparatus, preventing the valve from functioning normally.
Examples include:
- Functional mitral regurgitation secondary to left ventricular dilation
- Ischemic mitral regurgitation following myocardial infarction
Recognizing this distinction is important because a normal-looking valve can still produce severe regurgitation.
3. Primary Structural Disease
Intrinsic abnormalities of the valve may also be responsible, including:
- Mitral valve prolapse
- Bicuspid aortic valve
- Congenital valvular lesions
Although these conditions often present earlier in life, they may not become clinically significant until much later.
4. Acute Valvular Emergencies
Finally, there are the lesions emergency physicians cannot afford to miss.
These include:
- Infective endocarditis with leaflet destruction
- Papillary muscle rupture following myocardial infarction resulting in acute severe mitral regurgitation
- Acute aortic regurgitation secondary to type A aortic dissection
- Acute decompensation of previously compensated severe valvular disease
These patients frequently deteriorate rapidly. Failure to consider an acute valvular lesion can delay the diagnosis entirely.
A Simpler Framework: The Three Pillars of Valve Assessment
Valve assessment becomes much more approachable when you simplify it into three components:
- Structure
- Movement
- Flow
That’s it. Every valve examination begins by asking the same three questions.
- What does the valve look like?
- How well does it move?
- What is blood doing across it?
Evaluating each of these pillars individually, and then integrating them together, provides a rapid, reproducible approach to bedside valve assessment that is well suited to emergency medicine.
1. Structure
Every valve assessment begins with structure.
Before you turn on color Doppler or start looking for regurgitant jets, take a moment to simply look at the valve. B-mode imaging often provides more information than we give it credit for, particularly when interpreted alongside the surrounding cardiac chambers.
Start with the valve itself. Ask:
- Does it look normal?
- Is it thickened?
- Is it calcified?
- Does it appear unusually echogenic?
- Is there a vegetation or other abnormal mass?
Once you’ve assessed the valve, zoom out.
The heart adapts remarkably well to chronic valvular disease. Over months to years, pressure and volume overload produce predictable remodeling of the surrounding chambers. Often, these secondary changes are just as informative as the valve itself.
Look for:
- Left atrial dilation
- Left ventricular dilation
- Concentric left ventricular hypertrophy
- Right atrial or right ventricular enlargement
These findings shouldn’t be interpreted in isolation. Rather, they should support what you’re seeing at the valve. A thickened, immobile mitral valve becomes much more convincing when it’s accompanied by a markedly enlarged left atrium. Likewise, a calcified aortic valve with concentric LV hypertrophy paints a much stronger picture of chronic pressure overload than either finding alone.
The more the valve and the surrounding chambers tell the same story, the more confident you can be in your diagnosis.
Structural Findings Suggestive of Stenosis
Stenotic valves typically share a common appearance.
Look for valves that are:
- Thickened
- Echogenic
- Calcified
- Poorly mobile
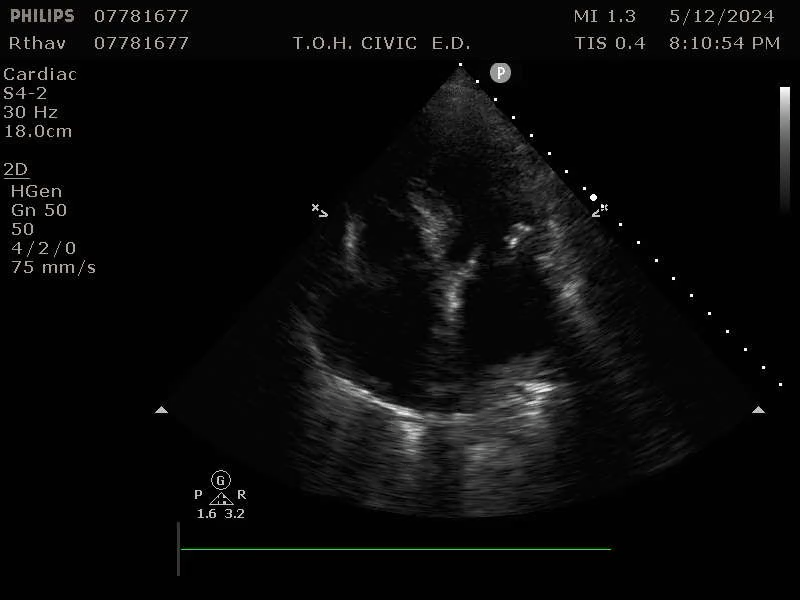
Figure 1: thickened, hyperechoic, and stiff mitral valve seen in A4C view
Chronic pressure overload also leaves characteristic changes within the myocardium.
In aortic stenosis, you may see:
- Concentric left ventricular hypertrophy
- A relatively small LV cavity
- Evidence of diastolic dysfunction
These findings reflect years of pumping against an increasingly fixed obstruction.
In mitral stenosis, the predominant structural consequence is left atrial enlargement.
A chronically elevated transmitral gradient increases left atrial pressure over time, eventually leading to marked dilation.
Fig 2: Left atrium dilation in setting of chronic severe MS
Remember, none of these findings independently diagnose severe stenosis. Many elderly patients have calcified valves, and ventricular hypertrophy has numerous causes. However, when multiple structural findings fit together, they substantially increase the likelihood of clinically important disease.
Structural Findings Suggestive of Regurgitation
Regurgitant lesions produce a different pattern of remodeling.
Instead of pressure overload, chronic regurgitation creates volume overload of the receiving chamber. As blood repeatedly flows backwards during each cardiac cycle, the affected chambers gradually enlarge to accommodate the increased volume.
Typical examples include:
- Chronic mitral regurgitation: dilation of both the left atrium and left ventricle
- Chronic aortic regurgitation: left ventricular dilation
- Severe tricuspid regurgitation: right atrial and right ventricular dilation
Fig 3: Dilated LV and LA in setting of severe chronic MR. Also note the thickened, irregular appearance of the MV leaflets.
Just as with stenosis, these chamber changes aren’t specific. Cardiomyopathy, hypertension, and atrial fibrillation can all produce chamber enlargement. However, when the remodeling pattern matches the valve abnormality you’re seeing, your confidence in the diagnosis increases considerably.
Vegetations
Occasionally, structural assessment reveals something much more dramatic.
Vegetations should immediately raise concern for infective endocarditis, particularly when they are identified in the appropriate clinical context. Classically, vegetations appear:
- Mobile
- Irregular
- Attached to a valve leaflet
Not every mobile structure is a vegetation. Lambl’s excrescences, fibroelastomas, redundant chordae, and imaging artifact can all mimic endocarditis. Conversely, a negative PoCUS examination certainly doesn’t exclude infective endocarditis, especially when vegetations are small or image quality is limited.
Nevertheless, identifying a large, independently mobile mass attached to a valve in a febrile patient with positive blood cultures should immediately escalate your concern and prompt urgent comprehensive echocardiography.
One final point is worth emphasizing. Emergency physicians don’t need to determine whether a valve area measures 0.7 or 0.9 cm² at the bedside. That’s the role of comprehensive echocardiography. Instead, ask yourself a simpler question: Does this valve look significantly abnormal, and do the surrounding chambers support what I’m seeing? If the answer is yes, you’ve already accomplished the most important part of structural valve assessment.
2. Movement: How is the Valve Functioning?
Once you’ve assessed the valve’s structure, the next step is determining how well it functions. Fortunately, valve motion can be distilled into one simple concept:
- Stenotic valves don’t open well.
- Regurgitant valves don’t close well.
If you keep those two principles in mind, you’ll recognize many clinically important lesions before you even activate color Doppler.
Stenosis: Does the Valve Open?
A healthy valve should open widely and effortlessly. As stenosis develops, the leaflets become progressively thicker, stiffer, and less mobile. Eventually, the valve becomes fixed in position, creating an obstruction to forward blood flow. When evaluating for stenosis, focus on leaflet excursion.
Ask yourself:
- Do the leaflets open fully?
- Is their movement symmetric?
- Do they appear stiff or restricted?
- Does the valve seem fixed throughout systole or diastole?
The more restricted the valve appears, the greater the likelihood that significant stenosis is present.
Fig 4: Example of severe AS in PSLA view. Note the tight, largely immobile aortic valve.
Although this sounds straightforward, remember that no single finding should be interpreted in isolation. A mildly calcified valve with reasonable excursion may represent sclerosis rather than clinically important stenosis. Conversely, a severely calcified valve that barely opens, particularly when accompanied by concentric LV hypertrophy and turbulent flow, should immediately raise concern for severe disease.
A normal valve opens widely, a stenotic valve opens only partially.
Regurgitation: Does the Valve Close?
Regurgitation is fundamentally a failure of valve closure. Instead of preventing backward flow, the leaflets fail to meet properly during closure, allowing blood to leak into the receiving chamber. Before reaching for color Doppler, look carefully at the valve itself.
Signs of significant regurgitation include:
- Poor leaflet coaptation
- A visible coaptation gap
- A flail leaflet
- Chordal rupture
- Papillary muscle rupture
Sometimes the mechanism is immediately obvious. A flail posterior mitral leaflet following myocardial infarction tells you almost everything you need to know before you’ve even looked at the regurgitant jet. Likewise, a large coaptation defect or ruptured papillary muscle should immediately raise concern for acute severe mitral regurgitation.
Fig 5: MR seen in PSLA view. Note the gap between the anterior and posterior MV leaflets at the end of diastole
Remember that acute and chronic regurgitation can appear very different. In chronic disease, compensatory remodeling may produce a markedly enlarged atrium or ventricle. In acute regurgitation, however, the chambers may still appear relatively normal because they haven’t had time to remodel. These patients are often much sicker despite the absence of dramatic structural changes. Clinical context always matters.
3. Flow
Structure tells you what the valve looks like. Movement tells you how well it’s functioning. Color Doppler answers the final question: What is the blood actually doing?
If B-mode imaging shows the anatomy, color Doppler shows the physiology. It allows you to visualize blood flow across the valve in real time, helping identify both stenotic and regurgitant lesions that may be difficult or impossible to appreciate on grayscale imaging alone.
At its simplest, color Doppler tells you three things:
- The direction of blood flow
- The relative velocity of that flow
- Whether the flow is smooth or turbulent
Fortunately, you don’t need to be a Doppler expert to recognize important pathology. Understanding a few basic principles will allow you to identify many clinically significant valve lesions at the bedside.
Understanding the Colours
One of the most common misconceptions is that the Doppler colors represent arteries and veins. They don’t.
Instead, the colors simply describe the direction that blood is moving relative to the ultrasound probe. A useful mnemonic is BART:
- Blue = Away from the probe
- Red = Toward the probe
Aortic flow, mitral inflow, pulmonary venous flow, and regurgitant jets can all appear either red or blue depending entirely on the imaging window and the orientation of the probe.
Focus less on the color itself and more on whether the direction of flow makes physiologic sense.
The Mosaic Pattern Matters
Equally important is the appearance of the color signal. Normal blood flow is relatively laminar and produces a fairly uniform color pattern. As blood accelerates through a narrowed valve, or leaks backward through an incompetent one, the flow becomes increasingly chaotic.
Instead of a single uniform color, you’ll begin to see a mixture of reds, blues, yellows, and greens creating the classic mosaic appearance. This pattern reflects high-velocity turbulent flow and is usually the result of aliasing, a concept we’ll discuss in more detail shortly.
Rather than viewing the mosaic pattern as an artifact, think of it as an important clue. It’s often exactly what severe valvular disease looks like.
Typical examples include:
- Severe stenosis, producing a narrow, high-velocity turbulent forward jet.
- Severe regurgitation, producing a turbulent backward jet extending into the receiving chamber.
Color Doppler doesn’t tell you everything about valve severity, but it quickly tells you where blood is moving, and where it shouldn’t be.
Fig 6: turbulent mosaic jet in setting of severe chronic AR seen on PSLA view
Getting the Machine Settings Right
Color Doppler is only as good as the image you acquire. Poor machine settings can make normal flow appear abnormal, or hide pathology that is actually present. Before deciding whether a valve is severely diseased, take a few seconds to optimize your image.
Fortunately, only three settings matter for most bedside valve assessments:
- Gain
- Nyquist limit
- Color box size
Mastering these three adjustments will dramatically improve the quality of your Doppler images.
Gain
Gain controls how much the Doppler signal is amplified.
If the gain is set too high, color begins to “bleed” into surrounding tissue and normal laminar flow may appear turbulent. Small physiologic jets suddenly look pathologic, making regurgitation appear much worse than it really is.
If the gain is set too low, the opposite happens. Color signal disappears, and significant regurgitant jets may look deceptively small or disappear altogether.
A simple bedside trick is to slowly increase the gain until random color speckling begins to appear throughout the image. Then reduce it just enough for the background speckling to disappear. This usually provides an appropriate balance between sensitivity and artifact.
Fig 7: Examples of gain differences. Clip taken from Alberta Sono
Nyquist Limit and Aliasing
The Nyquist limit is the maximum velocity that color Doppler can accurately display. When blood travels faster than this limit, the ultrasound machine can no longer represent the velocity correctly. Instead, the color abruptly wraps around, creating the familiar mosaic appearance known as aliasing.
You’ll often see:
- Sudden red becoming blue, or blue becoming red
- A mosaic pattern containing multiple colors
- Chaotic flow within a jet
Although aliasing is technically an imaging artifact, it is often a useful one. High-velocity flow is exactly what we expect to see in severe valvular disease.
For example:
- Severe aortic stenosis produces a narrow, high-velocity forward jet that frequently aliases.
- Severe regurgitation often produces a high-velocity backward jet with the same mosaic appearance.
Rather than trying to eliminate aliasing, recognize it as a clue that blood is moving very quickly.
Fig 8: Examples of Nyquist differences. Clip taken from Alberta Sono
Optimize Your Color Box
Finally, don’t overlook the size of the color box. A larger color box requires the machine to process much more information, reducing frame rate and degrading image quality.
For the best Doppler images:
- Make the color box as small as practical.
- Center it over the valve of interest.
- Align it with the expected direction of flow.
- Avoid including unnecessary cardiac structures.
A smaller, well-positioned color box produces a higher-quality image and makes abnormal flow patterns much easier to appreciate.
Recognizing Severe Stenosis
Formal assessment of valvular stenosis is complex. Cardiologists use spectral Doppler to measure peak velocity, mean pressure gradients, and valve area before assigning severity. That isn’t the goal of bedside PoCUS.
In the emergency department, our job is to recognize when a valve appears severely stenotic and determine whether it explains the patient’s presentation. Rather than focusing on measurements, look for a consistent pattern.
A severely stenotic valve is typically:
- Thickened and calcified
- Restricted with markedly reduced leaflet excursion
- Associated with chamber remodeling that reflects chronic pressure overload
- Producing a narrow, turbulent, high-velocity forward jet on color Doppler
When several of these findings are present together, the diagnosis becomes much more convincing than any single feature alone.
Severe Aortic Stenosis
Severe aortic stenosis should raise concern when you see:
- A heavily calcified, poorly mobile aortic valve
- Markedly reduced leaflet excursion
- Concentric left ventricular hypertrophy
- A narrow, turbulent forward jet across the valve
Fig 9: B-mode and Doppler clips of severe AS seen from A4C view. Clip taken from Poniros et al., 2025.
Severe Mitral Stenosis
Similarly, severe mitral stenosis is suggested by:
- Thickened mitral valve leaflets
- Reduced opening of the mitral valve
- Marked left atrial enlargement
- A turbulent, high-velocity inflow jet across the valve
No single finding confirms severe stenosis. Calcification alone does not equal obstruction, and chamber remodeling may have other causes.
The diagnosis becomes much more reliable when the structural abnormalities, valve motion, Doppler findings, and clinical presentation all point in the same direction.
Recognizing Severe Regurgitation
Regurgitant lesions are often easier to recognize because they are fundamentally visual diagnoses. Rather than asking whether the valve opens normally, ask whether it closes effectively.
A severely regurgitant valve generally has three features:
- A structural abnormality that explains the leak
- A large regurgitant jet on color Doppler
- Chamber remodeling consistent with chronic volume overload, when the lesion is chronic
Common structural clues include:
- A flail leaflet
- Poor leaflet coaptation
- A visible coaptation gap
- Papillary muscle rupture
- Chordal rupture
Color Doppler then helps confirm what you’re seeing. Findings that should raise concern for severe regurgitation include:
- A large eccentric jet
- A wall-hugging jet
- A regurgitant jet occupying more than half of the receiving chamber
- Flow convergence (PISA)
- A prominent vena contracta
You don’t need to measure these quantitatively in the emergency department. Instead, recognize that the larger and more hemodynamically significant the jet appears, the more likely severe regurgitation is present.
Severe Mitral Regurgitation
Features suggestive of severe mitral regurgitation include:
- Poor leaflet coaptation or a flail leaflet
- A large regurgitant jet extending deep into the left atrium
- Left atrial and left ventricular enlargement in chronic disease
Severe Aortic Regurgitation
Severe aortic regurgitation often demonstrates:
- An abnormal or poorly coapting aortic valve
- A broad regurgitant jet directed into the left ventricle
- Left ventricular dilation in chronic disease
- Turbulent aliased flow across the valve
One important caveat is that acute regurgitation behaves differently. Patients with papillary muscle rupture or acute aortic regurgitation may have relatively normal chamber sizes because there has been insufficient time for cardiac remodeling. Despite this, they are often critically ill. Normal chamber dimensions should never reassure you when the clinical picture suggests an acute valvular catastrophe.
Fig 10: B mode and Doppler views of severe AR. Interestingly this case shows a mixed picture of both AR and AS in the same valve, which signifies severe disease. Clip taken from Poniros et al., 2025.
An Integrated Approach
No single ultrasound finding should be interpreted in isolation. A calcified valve does not necessarily indicate severe stenosis. A regurgitant jet alone may overestimate severity. A dilated chamber has a broad differential diagnosis. The strength of bedside valve assessment comes from integrating multiple findings into a coherent clinical picture.
Ask yourself:
- Does the valve look abnormal?
- Does it move abnormally?
- Does color Doppler demonstrate abnormal flow?
- Do the chambers show the expected physiologic response?
- Does all of this fit the patient’s presentation?
When the answer to those questions is yes, your confidence in the diagnosis should be high.
When the findings don’t fit together, resist the temptation to overcall severity. Instead, describe what you see objectively.
For example:
- Significant valvular disease
- Findings concerning for severe valve pathology
Those patients should undergo comprehensive echocardiography and, when appropriate, early cardiology consultation.
References
- Alberta Sono. (n.d.). Colour Doppler. https://www.albertasono.ca/colour-doppler/
- Pellett, A. A., & Kerut, E. K. (2004). The Doppler equation. Echocardiography, 21(2), 197–198. https://doi.org/10.1111/j.0742-2822.2004.03081.x
- (accessed 2026). Valvular heart disease in older adults. Wolters Kluwer. https://www.uptodate.com
- Alzahrani, H., Woo, M. Y., Johnson, C., Pageau, P., Millington, S., & Thiruganasambandamoorthy, V. (2015). Can severe aortic stenosis be identified by emergency physicians when interpreting a simplified two-view echocardiogram obtained by trained echocardiographers? Critical Ultrasound Journal, 7(1), 15. https://doi.org/10.1186/s13089-015-0022-8
- Baumgartner, H., Hung, J., Bermejo, J., Chambers, J. B., Evangelista, A., Griffin, B. P., Iung, B., Otto, C. M., Pellikka, P. A., & Quiñones, M. (2009). Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. Journal of the American Society of Echocardiography, 22(1), 1–23. https://doi.org/10.1016/j.echo.2008.11.029
- Baumgartner, H., Hung, J., Bermejo, J., Chambers, J. B., Edvardsen, T., Goldstein, S., Lancellotti, P., LeFevre, M., Miller, F., Otto, C. M., & others. (2017). Recommendations on the echocardiographic assessment of aortic valve stenosis: A focused update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Journal of the American Society of Echocardiography, 30(4), 372–392. https://doi.org/10.1016/j.echo.2017.02.009
- Poniros, A., Nevin, K., Tang, G. H. L., & Safi, L. M. (2025). How to scan patients with severe aortic stenosis. JACC: Case Reports, 30(21), 104415. https://doi.org/10.1016/j.jaccas.2025.104415
- Stenberg, R., Bowling, J., Jacquet, J., Watkins, K., Eggleston, J., Hill, A., & Krizo, J. (2024). Point-of-care ultrasound diagnosis of acute valvular emergencies. American Journal of Emergency Medicine, 58, 30–36. https://doi.org/10.1016/j.ajem.2023.10.050 (verify exact DOI if needed)
- Via, G., Hussain, A., Wells, M., Reardon, R., ElBarbary, M., Noble, V., Tsung, J. W., Neskovic, A. N., Price, S., Oren-Grinberg, A., Liteplo, A., Cordioli, R., Naqvi, N., Tols, J., Labovitz, A., Kimura, B., Breitkreutz, R., Nazerian, P., Vignon, P., … International Liaison Committee on Focused Cardiac Ultrasound (ILC-FoCUS). (2014). International evidence-based recommendations for focused cardiac ultrasound. Journal of the American Society of Echocardiography, 27(7), 683.e1–683.e33. https://doi.org/10.1016/j.echo.2014.05.001
- Zoghbi, W. A., Adams, D., Bonow, R. O., Enriquez-Sarano, M., Foster, E., Grayburn, P. A., Hahn, R. T., Han, Y., Hung, J., Lang, R. M., Little, S. H., Shah, D. J., Shernan, S., Thavendiranathan, P., Thomas, J. D., Weissman, N. J., & others. (2017). Recommendations for noninvasive evaluation of native valvular regurgitation. Journal of the American Society of Echocardiography, 30(4), 303–371. https://doi.org/10.1016/j.echo.2017.01.007