

“When You Hear Hooves, Think Horse, Not Zebra” – Dr. Theodore Woodward
This above sentence is a dictum that every medical student has heard at some point during their training. It’s the reason, that when someone comes in febrile and agitated our first thoughts are to think of sympathomimetic toxidromes, serotonin syndrome, neuroleptic malignant syndrome, alcohol withdrawal, heat stroke, and even more common than that sepsis and intracranial infections such as meningitis and encephalitis.
The so-called “HOT AND CRAZY” differential is however home to a zebra that shouldn’t be forgotten – THYROID STORM.
In today’s blog post, we will aim to tackle this often forgotten but highly deadly complication of a hyperactive thyroid. From basic definitions, diagnosis and management, we hope this will be your one-stop-shop for everything thyroid storm related.
Back to Basics
“If you miss the beginning, the basics, then you are destined to go back and visit the basics” – Anonymous
Understanding the physiology of a functioning hypopituitary access, is the first step in understanding the overactive thyroid. So let’s take it step-by-step:
-
- The hypothalamus releases thyrotropin releasing hormones [TRH].
- TRH stimulates the anterior pituitary to produce thyroid stimulating hormone [TSH].
- TSH stimulates the thyroid gland to produce thyroid hormones: a mixture of Triiodothyronine [T3] and Thyroxine [T4].
- Important to remember: this above step requires the use of IODINE.
- T4 is converted peripherally into T3 via de-iodination.
- T3 raises the basal metabolic rate, by directly stimulating the Na-K-ATPase pump, causing an increased O2 demand and heat production. It also increases gluconeogenesis, and lyposis, while directly stimulating B1 cardiac receptors.
- Overactive Thyroid = Hyperadrenergic State
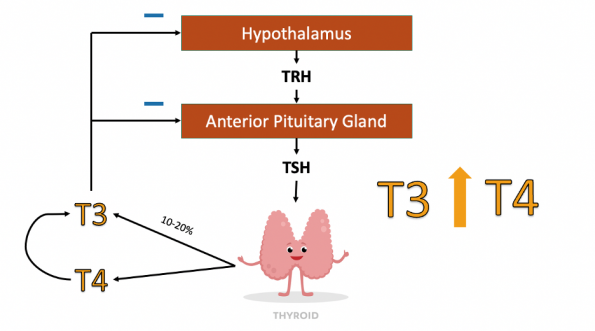
Under normal circumstances when there is an abundance of thyroid hormones, they operate on a negative feedback loop to decrease TRH and TSH release from the hypothalamus and anterior pituitary gland. However, when a disruption in this homeostatic environment occurs, the axis produces excess thyroid hormone [T3 and T4]. This typically occurs via one of three mechanisms:
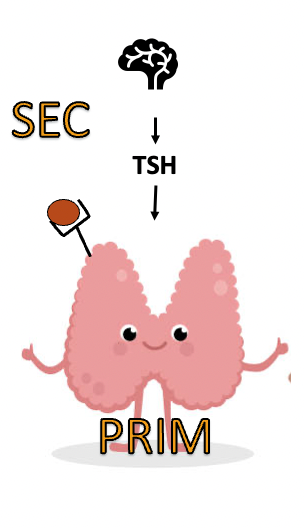 |
Disruption of the Hypopituitary Axis
Primary hyperthyroidism: Overproduction of thyroid hormones occurs directly at the level of the thyroid gland. Example: Graves’ disease – Wherein antibodies chronically stimulate the third via TSH receptors.
Secondary hyperthyroidism: Disruption occurs above the level of the thyroid. Example: pituitary adenomas which secrete TSH. |
 |
Exogenous Source
Additional T3 and T4 originating from outside the hypopituitary access. Examples: Hydatidiform Moles or Synthroid Overdose |
 |
Endogenous Release
Direct injury to the thyroid, often from inflammation or infection, leads to a large release of T3 and T4.
This is Thyroiditis |
Overactive Thyroid Entities
Hyperthyroidism is biochemically defined as an elevated T3 and T4. Often this is associated with a suppressed TSH; in the case of a functional hypopituitary axis. However, biochemical levels do not translate to the clinical environment. The hyperactive thyroid, therefore presents clinically along a spectrum:
-
- Subclinical Hyperthyroidism:
State in which less TSH is produced despite normal biochemical levels of T3 and T4. Typically not associated with any clinical symptoms.
-
- Hyperthyroidism and Thyrotoxicosis:
| Hyperthyroidism | Thyrotoxicosis | Apathetic Thyrotoxicosis |
| Pathological state in which excess thyroid hormones are synthesized, from one of the three previously mentioned mechanisms. Hyperthyroidism is the term typically used to define the biochemical state of elevated T3/T4. | Clinical syndrome that occurs as a result of hyperthyroidism. Symptoms include tachycardia, pyrexia, hyperkinesis, weight loss, diarrhea, nausea, vomiting and more.
Overactive Thyroid = Hyperadrenergic State |
Clinical syndrome where typical symptoms of hyperadrenergia are absent. Patients instead present with apathy, depression, and generalized weakness.
|
-
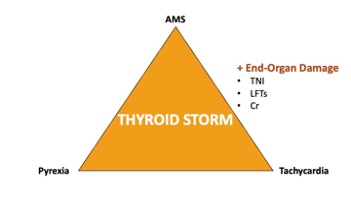
- Thyroid Storm:
Clinical syndrome defined by a triad of pyrexia, AMS and tachycardia, with evidence of end-organ damage.
Why do we Care?
Mortality Rate = 100% if untreated
Mortality Rate = 30-40% if treated
Diagnosing Thyroid Storm
| Thyroid Storm = CLINICAL Diagnosis |
The above statement is an important one to remember. Although lab tests can help support your diagnosis, thyroid storm is ultimately a clinical diagnosis, based on the triad of symptoms discussed above. However, this triad of symptoms is non-specific for thyroid storm, as it can also be present in other entities that fit the “HOT AND CRAZY” differential. So what if their was a tool that could help you with your clinical acumen?
In the literature, their are currently two clinical decision tools that have been developed to assist with the diagnosis of Thyroid Storm.
-
- Burch-Wartofsky Point Scale (BWPS)
- Restrospectively developed in 1993, by Dr. Burch. The point scale aims to determine the likelihood that biochemical hyperthyroidism (i.e. elevated T3/T4) is representative of thyroid storm.
- Score <25 = Unlikely
- Score 25-45 = Equivocal/Impending
- Score >45 = Likely
- It’s use is supported in the 2011 American Thyroid Association Guidelines.
- It relies on scoring of each one of the following clinical signs and symptoms along a spectrum:
- Temperature
- CNS Effects
- GI/Hepatic Dysfunction
- HR
- CHF
- Afib
- Precipitating Event
- Click HERE to be taken to MD Calc Scoring tool.
- Restrospectively developed in 1993, by Dr. Burch. The point scale aims to determine the likelihood that biochemical hyperthyroidism (i.e. elevated T3/T4) is representative of thyroid storm.
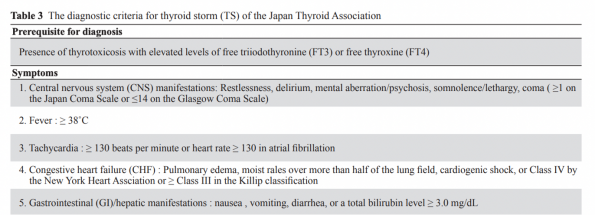
- Japanese Thyroid Association
- Published in 2011 by the Japanese Thyroid Association.
- Derived from evaluation of thyroid storm patients in Japan from 2001 to 2011.
- Much like the BWPS it aims to determine the likelihood of thyroid storm, based on the symptoms listed in Table 3 below (click diagram to link to original paper).
- TSI | If CN Sx + 1 other Sx OR ≥ 3 symptoms (Not CNS manifestations) = Definitive Thyroid Storm
- TS2 | If ≥2 Sx = Thyroid Storm Suspected
- Burch-Wartofsky Point Scale (BWPS)
Should we use these tools?
As you can imagine based on the elements incorporated into each of these tools, these scoring systems have high sensitivity for thyroid storm, but have poor specificity. For example, sepsis with multi-organ failure could easily score >45 on the BWPS tool. A recent study of 125 patients hospitalized with a clinical diagnosis of compensated thyrotoxicosis with NO evidence of thyroid storm, as per the local endocrinology team, emphasized the over-diagnosis of thyroid storm with the use of these tools. In the study 21.6% of patients had a BWPS > 45, while 16.8% had a TS1 score, despite being stable hyperthyroid patients. Ultimately, the tools serve more as a guide to help with understanding the symptoms and signs of thyroid storm, and perhaps categorize the severity of cases. It really isn’t tools we foresee using in the ED.
“Key message is that they’re not perfect and they don’t replace clinical judgement, e.g. can’t hang your hat on the score in many cases. But they can provide you a starting point to help assess severity of cases“
– Dr. Christopher Tran, FRCPC Endocrinologist
When should I consider the Dx of Thyroid Storm?
Here are a few clinical scenarios, that you should consider at minimum testing a TSH for the patient sitting in your emergency department:
- Patients with known hyperthyroidism and an acute illness/deterioration.
- New-onset atrial fibrillation and/or dilated cardiomyopathy.
- New-onset delirium/psychosis plus abnormal vital signs (fever, tachycardia).
- Hyperthermia (temperature 40C).
- Septic-appearing patient without any focus of infection (i.e. distributive shock of unknown origin).
- Classic “Hot and Crazy” presentation.
- Hypo/Hyperactive delirium in the elderly; unless they have had a TSH in the last 3 months.
Managing Thyroid Storm
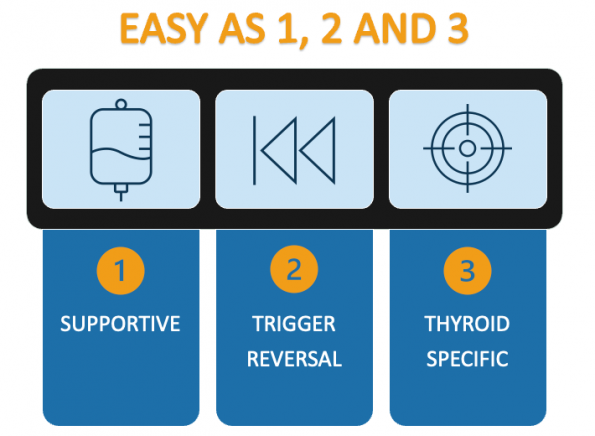
Step 1: Supportive Treatment
Supportive management should always be your first step in management. Remember your ABCs, and address each of these as you would in any other rescucitation. Treatment may include any of the following combinations:
-
- Fluid Rescucitation +/- pressors for refractory hypotension and hypovolemia.
- Antipyretics.
- Passive and Active Cooling.
- Benzodiazepines for management of extreme agitation.
- Investigations for Sepsis, including BCx, and early Abx.
Step 2: Identify and Reverse Potential Triggers
Thyroid Storm often results from undiagnosed hyperthyroidism, that is pushed into overdrive due to an illness trigger. Common triggers are listed in the table below – consequently, most cases of possible thyroid storm should have a full septic work-up, and global metabolic panel including LFTs, VBG and lactate.
| Global Triggers | Thyroid Specific |
| Surgery
Trauma ACS events Strokes DKA Sepsis/Major Infections Viral Illnesses |
Thyroid Surgery
Radioiodine Therapy Cessation of Hyperthyroidism Therapy Thyroid Hormon intentional or unintentional overdose (i.e. synthroid) Aspirin Intoxication (How? It can increase free thyroid hormone levels by displacing thyroid hormone from its protein-binding sites) |
Step 3: Thyroid Targeted Treatment
| Remember the 5Bs
(Block Synthesis, Block Release, Block Conversion, Block Beta and Block Enterohepatic Circulation) |
Block Synthesis: Thyroid Peroxidase Inhibitors
There are currently two thionamide drugs available on the market; Methimazole (MMI) and Propilthiouracil (PTU). These should be the first medication you reach for when you diagnose a thyroid storm, as they inhibit the formation of thyroid hormone, by competitive inhibition of thyroid peroxidase; the enzyme responsible for the conversion of iodide to iodine, and the formation of T4 and T3 from iodine and thyroglobulin. With two agents available on the market, which one should we be reaching for in the ED?
PTU has long been recommended as the preferred agent over methimazole, due to it’s added quality of blocking peripheral conversion of T4 to T3. Early, research additionally demonstrated that PTU dropped T3 levels by 45% in the first 24hrs of treatment, compared to 15% after initiation of methimazole. As such, it is often recommended to use PTU in the cases of severe thyroid storm. However, their currently is no head-to-head trial that directly compares and demonstrates PTU’s superiority. Additionally, PTU does present the risk for liver failure (0.5% risk), and cannot be continued in the outpatient setting. Comparatively, MMI is the preferred agent upon discharge from hospital. Irregardless, use the thyroid perodidase inhibitor you have at your disposal, as per the recommended dosing regime below.
REMEMBER: Although you may be starting these agents independently, you should reach out to your endocrinology colleagues as soon as possible.
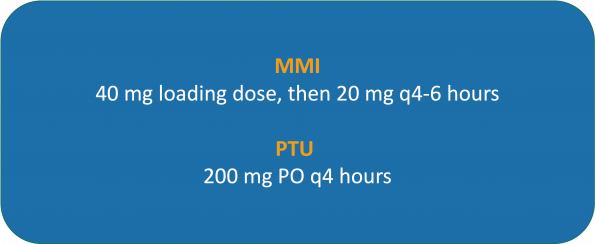
**Pregnancy Exception: Use PTU in the 1st trimester (due to rare MMI teratogenic effects). Use MMI in second and third trimesters.
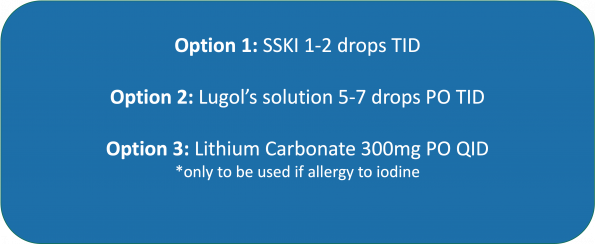
Block Release: Iodine
To block the release of thyroid hormones, Iodine is typically administered. The excess iodine load leads to inhibiton of thyroid synthesis via the Wolff-Chaikoff Effect. In 2010, Takata et al., demonstrated higher efficacy at reaching a euthyroid state, when a thyroid peroxidase inhibitor was combined with iodine, compared to placebo. However, the use of iodine is a double-edged sword. In certain circumstances, the iodine load can actually induce an up-regulation of thyroid hormone release; this is called the Jod-Basedown Effect. It is this same principle that explains activation of hyperthyroidism when patients have underlying Grave’s and receive iodinated contrast. This effect is often seen in individuals with iodine deficiencies, or those who have toxic nodular goiter. This is why it is imperative, that iodine products be given 1 hour after the thyroid peroxidase inhibitors, so as to first limit the production of thyroid hormone, so that in the event that the Jod-Basedown Effect is inacted, their is less thyroid hormone release.
IMPORTANT: Wait 1h post Thyroid Peroxidase Inhibitor administration before giving iodine.
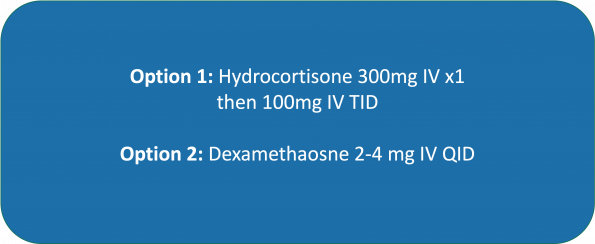
Block Conversion: Steroids
Administration of steroids, decreases peripheral conversion of T4 to T3. They are also favoured in refractory hypotension in the context of thyroid storm, as they may also address relative adrenal insufficiency resulting from the hypermetabolic state.
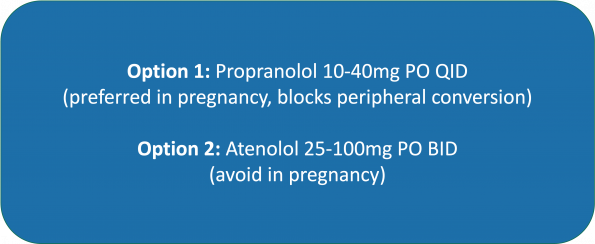
Block Beta : A Word of Caution with the use of Beta-Blockers
The use of beta-blockers is purely to assist with the symptoms that ensue from the adrenergic response triggered by thyroid storm. They provide symptomatic relief from tremors and palpitaitons, while also controlling tachycardia and increasing diastolic filling times (Tagami et al., 2012). It has NO effect on thyroid hormone levels.
However, the blind use of beta-blockers in thyroid storm should be met with caution by the emergency medicine physician. In reviewing the literature, their are enumerable case reports of precipitous decline and death following treatment of thyroid storm with beta-blockers. And this precipitous decline can be equated to the same principles that justify us to avoid use of beta-blockers in decompensated HFrEF – the negative inotropy conveyed by beta-blockers can easily precipitate cardiogenic shock in a patient with severe AS and/or severe HFrEF. Furthermore, up to 1% of hyperthyroidism may have undiagnosed cardiomyopathies with reduced LV function.
Rate control should be reserved for the patients with atrial fibrillation and RVR who have a preserved ejection fraction, or for those patients who are no longer in frank shock.
As the ED physician, it is therefore our role to evaluate the patient in shock in front of us, do a POCUS to assess LV function, and ascertain if it is safe to introduce the beta-blockers or not. Our local ICU/EM expert Dr. Ariel Hendin, also had the following to say:
“If a patient is hypotensive and tachy with thyroid storm, I would be most worried about cardiogenic shock. I would treat them as any other cardiogenic shock patient, and I would think carefully about antibiotics and steroids.I would not purse rate control, including propranolol, if in sinu. This is a patient who is potentially teetering on the edge of completely decompensating, and negative inotropy may precipitate that“
– Dr. Ariel Hendin, FRCPC Intensivist & FRCPC EM

When safe to do so, the following agents can be introduced for symptom management, and should be continued upon patient discharge, as they have a large positive impact on a patient’s overall quality of life.
IMPORTANT: Assess safety of beta-blockade in patients with “profound” shock
Block Enterohepatic Circulation
This is NOT a medication that would be expected to be started in the ED. Use of cholestyramine to reduce enterohepatic circulation and endogenous re-uptake, was shown in a study from 2005 by Tsai et al., to decrease serum T3/T4 measurement at 2 and 4 weeks more than use of PTU and propanolol alone. It is not required in the acute phase.
Conclusion
-
- Consider THYROID STORM as a potential Zebra in any of your “Hot and Crazy” presentations, especially when no alternative cause can be found.
-
- Recognition of Thyroid Storm is the most important.
-
- Thyroid storm is a CLINICAL DIAGNOSIS. Composed of a triad of pyrexia, AMS and tachycardia, with end-organ damage evidence on biochemical assays.
-
- In the ED, treatment should focus on early administration of MMI or PTU (Thyroid Peroxidase Inhibitors), to inhibit the synthesis of additional thyroid hormone. In addition to acute rescucitation of your ABCs.
-
- Be cautious of the use of beta-blockers in the severe thyroid storm with shock. Assess LV function and risk of cardiogenic shock before preceding with their administration.
References
- Albehair MA, Alagga AA, Ghulam WZ, Alomair AM, AlFaraj D. Thyroid Storm: Unusual Presentation and Complication. Cureus [Internet]. 2021 Jan 4 [cited 2022 Nov 30]; Available from: https://www.cureus.com/articles/48843-thyroid-storm-unusual-presentation-and-complication
- Ali H, Sarfraz S, Hassan L, Ali H. Atrial Fibrillation as an Initial Presentation of Apathetic Thyroid Storm. Cureus [Internet]. 2021 Sep 7 [cited 2022 Nov 30]; Available from: https://www.cureus.com/articles/70422-atrial-fibrillation-as-an-initial-presentation-of-apathetic-thyroid-storm
- Ali O, Truran P, Aspinall S. Thyrotoxicosis and thyroiditis. ENDOCRINE SURGERY. 2017;7.
- Almeida RD, McCalmon S, Cabandugama PK. Clinical Review and Update on the Management of Thyroid Storm. :6.
- Andrade Luz I, Pereira T, Catorze N. Thyroid storm: a case of haemodynamic failure promptly reversed by aggressive medical therapy with antithyroid agents and steroid pulse. BMJ Case Rep. 2018 Dec;11(1):e226669.
- Anfinsen OG, Lima K. Amiodarone-induced thyrotoxicosis. Tidsskrift for Den norske legeforening. :10.
- Angell TE, Lechner MG, Nguyen CT, Salvato VL, Nicoloff JT, LoPresti JS. Clinical Features and Hospital Outcomes in Thyroid Storm: A Retrospective Cohort Study. The Journal of Clinical Endocrinology & Metabolism. 2015 Feb;100(2):451–9.
- Ankireddypalli A, Vikraman PK, Mehta H. SURVIVING THE STORM: USE OF THERAPEUTIC PLASMA EXCHANGE IN THYROID STORM. Chest. 2020 Oct;158(4):A1000.
- Arens AM, Birmingham M, McHale E, Siegel-Richman Y, Driver BE. The utility of laboratory testing for suspected hyperthyroidism in the emergency department. The American Journal of Emergency Medicine. 2022 Apr;54:76–80.
- Azizi F, Amouzegar A. Management of thyrotoxicosis in children and adolescents: 35 years’ experience in 304 patients. Journal of Pediatric Endocrinology and Metabolism. 2018 Jan 26;31(2):159–65.
- Balde MC, Adrar EH, Bechara K, Prinseau J, Baglin A, Hanslik T. Hypokaliémie et paralysie : penser à la thyroïde. La Revue de Médecine Interne. 2008 Feb;29(2):155–7.
- Banerjee A, Bala R, Aggarwal R. Atypical presentation of thyroid storm: a diagnostic dilemma. BMJ Case Rep. 2019 Aug;12(8):e231090.
- Bartalena L, Wiersinga WM, Tanda ML, Bogazzi F, Piantanida E, Lai A, et al. Diagnosis and management of amiodarone-induced thyrotoxicosis in Europe: results of an international survey among members of the European Thyroid Association. Clin Endocrinol. 2004 Oct;61(4):494–502.
- Baskin HJack, Cobin RH, Duick DS, Gharib H, Guttler RB, Kaplan MM, et al. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the Evaluation and Treatment of Hyperthyroidism and Hypothyroidism. Endocrine Practice. 2002 Nov;8(6):457–69.
- Bernard Khoo, Tricia Tan, Sophie A Clarke, Edouard G Mills, Bijal Patel, Manish Modi, Maria Phylactou, Pei Chia Eng, Layla Thurston, Emma C Alexa nder, Karim Meeran, Alexander N Comninos, Ali Abbara, Waljit S Dhillo, Thyroid Function Before, During, and After COVID-19, The Journal of Clinical Endocrinology & Metabolism, Volume 106, Issue 2, February 2021, Pages e803–e811, https://doi.org/10.1210/clinem/dgaa830
- Bonucchi J, Hassan I, Policeni B, Kaboli P. Thyrotoxicosis Associated Wernicke’s Encephalopathy. J GEN INTERN MED. 2008 Jan;23(1):106–9.
- Bostan H, Sencar ME, Calapkulu M, Kayihan S, Hepsen S, Cimsir A, et al. Impact of the COVID-19 pandemic on the incidence, seasonal distribution, and characteristics of subacute thyroiditis. Endocrine [Internet]. 2022 Sep 21 [cited 2022 Nov 30]; Available from: https://link.springer.com/10.1007/s12020-022-03197-3
- Bourcier S, Coutrot M, Kimmoun A, Sonneville R, de Montmollin E, Persichini R, et al. Thyroid Storm in the ICU: A Retrospective Multicenter Study. Critical Care Medicine. 2020 Jan;48(1):83–90.
- Capezzone M, Tosti-Balducci M, Morabito EM, Caldarelli GP, Sagnella A, Cantara S, et al. Silent thyroiditis following vaccination against COVID-19: report of two cases. J Endocrinol Invest. 2022 May;45(5):1079–83.
- Carlé A, Andersen SL, Boelaert K, Laurberg P. MANAGEMENT OF ENDOCRINE DISEASE: Subclinical thyrotoxicosis: prevalence, causes and choice of therapy. European Journal of Endocrinology. 2017 Jun;176(6):R325–37.
- Carroll R, Matfin G. Review: Endocrine and metabolic emergencies: thyroid storm. Therapeutic Advances in Endocrinology. 2010 Aug;1(3):139–45.
- Chiha M, Samarasinghe S, Kabaker AS. Thyroid Storm: An Updated Review. J Intensive Care Med. 2015 Mar;30(3):131–40.
- Christensen J, O’Callaghan K, Sinclair H, Hawke K, Love A, Hajkowicz K, et al. Risk factors, treatment and outcomes of subacute thyroiditis secondary to COVID ‐19: a systematic review. Internal Medicine Journal. 2022 Apr;52(4):522–9.
- Conen D, Melly L, Kaufmann C, Bilz S, Ammann P, Schaer B, et al. Amiodarone-Induced Thyrotoxicosis. Journal of the American College of Cardiology. 2007 Jun;49(24):2350–5.
- Croce L, Gangemi D, Ancona G, Liboà F, Bendotti G, Minelli L, et al. The cytokine storm and thyroid hormone changes in COVID-19. J Endocrinol Invest. 2021 May;44(5):891–904.
- Davis S, Mcintyre R, Cribari C, Dunn J. Thyroid Storm Induced by Trauma: A Challenging Combination. The American Surgeon. 2018 Feb;84(2):44–6.
- Devereaux D, Tewelde SZ. Hyperthyroidism and Thyrotoxicosis. Emergency Medicine Clinics of North America. 2014 May;32(2):277–92.
- Dunne P, Mbbs NK, MacDonald J, Mbbs AAS. Iodinated contrast–induced thyrotoxicosis. :4.
- Gilbert J. Thyrotoxicosis – investigation and management. Clin Med. 2017 Jun;17(3):274–7.
- Goichot B, Caron Ph, Landron F, Bouée S. Clinical presentation of hyperthyroidism in a large representative sample of outpatients in France: relationships with age, aetiology and hormonal parameters. Clin Endocrinol. 2016 Mar;84(3):445–51.
- Grebe SKG, Kahaly GJ. Laboratory Testing in Hyperthyroidism. The American Journal of Medicine. 2012 Sep;125(9):S2.
- Gupta A, Arora S. ATRIOVENTRICULAR HEART BLOCKS IN THYROTOXICOSIS. Journal of the American College of Cardiology. 2015 Mar;65(10):A738.
- Gupta P, Chhabra L, Hiendlmayr B, Spodick DH. Thyrotoxic pericarditis: An underappreciated phenomenon. International Journal of Cardiology. 2015 Nov;198:32–3.
- Hampton J. Thyroid Gland Disorder Emergencies. AACN Advanced Critical Care. 2013 Jul 1;24(3):325–32.
- Harirforoosh S, Cohen G, Glovaci D, Patel PM. Right heart failure in the setting of thyrotoxic valvulopathy: the pathophysiology of an often neglected diagnosis: a case report. Eshtehardi P, Gohar A, Khalifa A, Bernstein BS, Vervaat F, editors. European Heart Journal – Case Reports. 2022 Sep 5;6(9):ytac305.
- Idrose AM. Acute and emergency care for thyrotoxicosis and thyroid storm: Management of thyroid storm. Acute Medicine & Surgery. 2015 Jul;2(3):147–57.
- Ishihara Y, Sugawa T, Kaneko H, Hiroshima-Hamanaka K, Amano A, Umakoshi H, et al. The Delayed Diagnosis of Thyroid Storm in Patients with Psychosis. Intern Med. 2019 Aug 1;58(15):2195–9.
- Jaber JA, Haque S, Noor H, Ibrahim B, Al Suwaidi J. Thyrotoxicosis and Coronary Artery Spasm: Case Report and Review of the Literature. Angiology. 2010 Nov;61(8):807–12.
- Kaddis A, Tellez T. Thyrotoxicosis: an unusual cause of syncope. The American Journal of Emergency Medicine. 2019 Apr;37(4):797.e5-797.e6.
- Kim J, Baek HS, Ha J, Kim MK, Kwon HS, Song KH, et al. Differential Diagnosis of Thyrotoxicosis by Machine Learning Models with Laboratory Findings. Diagnostics. 2022 Jun 15;12(6):1468.
- Kim Y, Gurung D, Sumbly V, Reich DM, Bashir T. Thyroid Storm-Induced Acute Liver Dysfunction and Disseminated Intravascular Coagulation. Cureus [Internet]. 2021 Jul 20 [cited 2022 Nov 30]; Available from: https://www.cureus.com/articles/59229-thyroid-storm-induced-acute-liver-dysfunction-and-disseminated-intravascular-coagulation
- Kiriyama H, Amiya E, Hatano M, Hosoya Y, Maki H, Nitta D, et al. Rapid Improvement of thyroid storm-related hemodynamic collapse by aggressive anti-thyroid therapy including steroid pulse: A case report. Medicine. 2017 Jun;96(22):e7053.
- Kornelius E, Chang KL, Yang YS, Huang JY, Ku MS, Lee KY, et al. Epidemiology and factors associated with mortality of thyroid storm in Taiwan: a nationwide population-based study. Intern Emerg Med. 2021 Apr;16(3):601–7.
- Lania, A., Sandri, M. T., Cellini, M., Mirani, M., Lavezzi, E., & Mazziotti, G. (2020). Thyrotoxicosis in patients with COVID-19: the THYRCOV study, European Journal of Endocrinology, 183(4), 381-387. Retrieved Dec 1, 2022, from https://eje.bioscientifica.com/view/journals/eje/183/4/EJE-20-0335.xml
- Lee KA, Kim YJ, Jin HY. Thyrotoxicosis after COVID-19 vaccination: seven case reports and a literature review. Endocrine. 2021 Dec;74(3):470-472. doi: 10.1007/s12020-021-02898-5. Epub 2021 Oct 12. PMID: 34637073; PMCID: PMC8507356.
- Lee SY, Yu CW, Choi YJ, Choi RK, Park JS, Lee HJ, et al. A comparison of clinical features of coronary artery spasm with and without thyrotoxicosis. Coronary Artery Disease. 2014 Mar;25(2):125–32.
- Levy MJ, Reddy N, Price D, Bhake R, Bremner E, Barrowcliffe M, et al. Audit of long‐term treatment outcomes of thyrotoxicosis in a single‐centre virtual clinic: The utility of long‐term antithyroid drugs. Clinical Endocrinology. 2022 Nov;97(5):643–53.
- Liang CM, Ho MH, Wu XY, Hong ZJ, Hsu SD, Chen CJ. Thyroid storm following trauma: A pitfall in the emergency department. Injury. 2015 Jan;46(1):169–71.
- Lin SH, Chu P, Cheng CJ, Chu SJ, Hung YJ, Lin YF. Early diagnosis of thyrotoxic periodic paralysis: Spot urine calcium to phosphate ratio*: Critical Care Medicine. 2006 Dec;34(12):2984–9.
- Maqdasy S, Benichou T, Dallel S, Roche B, Desbiez F, Montanier N, et al. Issues in amiodarone-induced thyrotoxicosis: Update and review of the literature. Annales d’Endocrinologie. 2019 Feb;80(1):54–60.
- McLean JRL, Allan K. Thyroid storm presenting with coma. Anaesthesia Reports [Internet]. 2021 Jul [cited 2022 Nov 30];9(2). Available from: https://onlinelibrary.wiley.com/doi/10.1002/anr3.12134
- Milani N, Najafpour M, Mohebbi M. Case series: Rare cases of thyroid storm in COVID‐19 patients. Clin Case Rep [Internet]. 2021 Sep [cited 2022 Nov 30];9(9). Available from: https://onlinelibrary.wiley.com/doi/10.1002/ccr3.4772
- Minch M, Moore W, Fineberg S, Agarwal M. Abstract #1110 Therapeutic Plasma Exchange in a Case of Thyroid Storm. Endocrine Practice. 2018 Apr;24:278–9.
- Muller C, Perrin P, Faller B, Richter S, Chantrel F. Role of Plasma Exchange in the Thyroid Storm: Role of PE in the Thyroid Storm. Therapeutic Apheresis and Dialysis. 2011 Dec;15(6):522–31.
- Narkar R, Mishra I, Baliarsinha A, Choudhury A. Rapid differential diagnosis of thyrotoxicosis using T3/T4 ratio, FT3/FT4 ratio and color doppler of thyroid gland. Indian J Endocr Metab. 2021;25(3):193.
- Nayak B, Burman K. Thyrotoxicosis and Thyroid Storm. Endocrinology and Metabolism Clinics of North America. 2006 Dec;35(4):663–86.
- Ono Y, Ono S, Yasunaga H, Matsui H, Fushimi K, Tanaka Y. Factors Associated With Mortality of Thyroid Storm: Analysis Using a National Inpatient Database in Japan. Medicine. 2016 Feb;95(7):e2848.
- Ortiz-Diaz EO. A 27-year-old woman presenting with refractory hypoxaemic respiratory failure, haemoptysis and thyrotoxicosis: a rare manifestation of propylthiouracil therapy. Case Reports. 2014 Aug 22;2014(aug22 1):bcr2014204915–bcr2014204915.
- Patel K, McCoy JV, Davis PM. Recognizing thyrotoxic hypokalemic periodic paralysis. Journal of the American Academy of Physician Assistants. 2018 Jan;31(1):31–4.
- Paz-Ibarra J, Benites R, Omoniyi E, Shin TH. PERSISTENT POSITIVE RADIOIODINE WHOLE-BODY SCAN IN A PATIENT WITH DIFFERENTIATED CANCER OF THYROID. :3.
- Peng X, Wu S, Bie C, Tang H, Xiong Z, Tang S. Mean peak systolic velocity of superior thyroid artery for the differential diagnosis of thyrotoxicosis: a diagnostic meta-analysis. BMC Endocr Disord. 2019 Dec;19(1):56.
- Petersen M, Knudsen N, Carlé A, Andersen S, Jørgensen T, Perrild H, et al. Thyrotoxicosis after iodine fortification. A 21-year Danish population-based study. Clin Endocrinol. 2018 Sep;89(3):360–6.
- Pimentel L, Hansen KN. Thyroid disease in the emergency department: A clinical and laboratory review. The Journal of Emergency Medicine. 2005 Feb;28(2):201–9.
- Pla Peris B, Merchante Alfaro AÁ, Maravall Royo FJ, Abellán Galiana P, Pérez Naranjo S, González Boillos M. Thyrotoxicosis following SARS-COV-2 vaccination: a case series and discussion. J Endocrinol Invest. 2022 May;45(5):1071–7.
- Portelli D, Mifsud S, Abela A, Fava S. Amiodarone-induced type 2 thyrotoxicosis. BMJ Case Rep. 2021 Jan;14(1):e238145.
- Pride W, Smith A, Joseph R. Thyroid storm following rapid sequence intubation. The American Journal of Emergency Medicine. 2018 Dec;36(12):2338.e5-2338.e6.
- Radhi MA, Natesh B, Stimpson P, Hughes J, Vaz F, C. Dwivedi R. Thyroid Storm in Head and Neck Emergency Patients. JCM. 2020 Nov 4;9(11):3548.
- Rivas AM, Thavaraputta S, Orellana-Barrios MA, Payne JD, Sotello D, Vinan-Vega M, et al. Thyrotoxic Periodic Paralysis and Complicated Thyrotoxicosis, Two Presentations of Hyperthyroidism with Notable Differences in their Clinical Manifestations: An Experience from a Tertiary Care Hospital in the United States. Endocrine Practice. 2020 Jul;26(7):699–706.
- Rosario PW, Carvalho M, Calsolari MR. Symptoms of thyrotoxicosis, bone metabolism and occult atrial fibrillation in older women with mild endogenous subclinical hyperthyroidism. Clin Endocrinol. 2016 Jul;85(1):132–6.
- Rosen’s Chapter 128 – 9th Edition
- Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid. 2016 Oct;26(10):1343–421.
- Satoh T, Isozaki O, Suzuki A, Wakino S, Iburi T, Tsuboi K, et al. 2016 Guidelines for the management of thyroid storm from The Japan Thyroid Association and Japan Endocrine Society (First edition): The Japan Thyroid Association and Japan Endocrine Society Taskforce Committee for the establishment of diagnostic criteria and nationwide surveys for thyroid storm [Opinion]. Endocr J. 2016;63(12):1025–64.
- Scappaticcio L, Trimboli P, Keller F, Imperiali M, Piccardo A, Giovanella L. Diagnostic testing for Graves’ or non‐Graves’ hyperthyroidism: A comparison of two thyrotropin receptor antibody immunoassays with thyroid scintigraphy and ultrasonography. Clin Endocrinol. 2020 Feb;92(2):169–78.
- Schubert L, Bricaire L, Groussin L. Amiodarone-induced thyrotoxicosis. Annales d’Endocrinologie. 2021 Jun;82(3–4):163–6.
- Senda A, Endo A, Tachimori H, Fushimi K, Otomo Y. Early administration of glucocorticoid for thyroid storm: analysis of a national administrative database. Crit Care. 2020 Dec;24(1):470.
- Shang W, Ma QB. Malignant Arrhythmias as the Unmasked Manifestation of Thyroid Storm. IJGM. 2020 Sep;Volume 13:693–8.
- Sharma A, Stan MN. Thyrotoxicosis: Diagnosis and Management. Mayo Clinic Proceedings. 2019 Jun;94(6):1048–64.
- Singh K, Duggal A, Dabra S, Kaur A, Singh RP, Rai P, et al. VARIED PRESENTATIONS OF THYROID STORM. :2.
- Singhi DRPK, Raju DRS, Kumar DRR. Thyroid storm an unusual postoperative complication – Can we evade it. Journal of Orthopaedics. 2020 Sep;21:481–2.
- Swee DS, Chng CL, Lim A. Clinical Characteristics and Outcome of Thyroid Storm: A Case Series and Review of Neuropsychiatric Derangements in Thyrotoxicosis. Endocrine Practice. 2015 Feb;21(2):182–9.
- Tan AWK, Lim BSP, Hoe JKM, Hoi WH, Leow MKS. Therapeutic plasma exchange for control of thyroid storm. J Clin Apher. 2021 Feb;36(1):189–95.
- Tanda ML, Piantanida E, Lai A, Liparulo L, Sassi L, Bogazzi F, et al. Diagnosis and management of amiodarone-induced thyrotoxicosis: similarities and differences between North American and European thyroidologists*. Clinical Endocrinology. 2008 Nov;69(5):812–8.
- The American Thyroid Association and American Association of Clinical Endocrinologists Taskforce on Hyperthyroidism and Other Causes of Thyrotoxicosis, Bahn RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, et al. Hyperthyroidism and Other Causes of Thyrotoxicosis: Management Guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011 Jun;21(6):593–646.
- Tsai MS, Yang CW, Chi CL, Hsieh CC, Chen WJ, Huang CH. Acute pericarditis: a rare complication of Graves’ thyrotoxicosis? The American Journal of Emergency Medicine. 2006 May;24(3):374–5.
- Tura Bahadır Ç, Yılmaz M, Kılıçkan E. Free triiodothyronine to free thyroxine ratio in the differential diagnosis of thyrotoxicosis and hyperthyroidism: A retrospective study. Int J Clin Pract [Internet]. 2021 May [cited 2022 Nov 30];75(5). Available from: https://onlinelibrary.wiley.com/doi/10.1111/ijcp.14003
- Vaidya B, Pearce SHS. Diagnosis and management of thyrotoxicosis. BMJ. 2014 Aug 21;349(aug21 7):g5128–g5128.
- Vennard K, Ng H, Nathan M, Schnure J. Abstract #1013 Thyroidectomy for the Treatment of Thyroid Storm. Endocrine Practice. 2018 Apr;24:224–5.
- Wang HI, Yiang GT, Hsu CW, Wang JC, Lee CH, Chen YL. Thyroid Storm in a Patient with Trauma – A Challenging Diagnosis for the Emergency Physician: Case Report and Literature Review. The Journal of Emergency Medicine. 2017 Mar;52(3):292–8.
- Wartofsky L. Clinical Criteria for the Diagnosis of Thyroid Storm. Thyroid. 2012 Jul;22(7):659–60.
- Winter T, Kraut E, Thompson K. Thyrotoxicosis and bilateral internal carotid artery dissections. The American Journal of Emergency Medicine. 2021 Jan;39:251.e1-251.e3.
Trackbacks/Pingbacks