We all know medications can help us feel better and stay healthy but as we are all familiar, sometimes drug interactions can be overlooked and cause significant adverse health outcomes. Drug interactions are common clinical problems that can occur in several different ways and in various settings. The estimated rate of drug interactions occurring in the emergency department is anywhere between 3% to 47%, unfortunately, heterogeneity in the literature makes it a challenging data point to capture.
But surely, you’ve been stopped by one of these alerts while working:

Studies have shown that adverse drug effects contribute to 1 in 9 emergency visits and often medication-related causes go unrecognized by physicians (ED or inpatient setting) up to half the time. This is concerning as the lack of timely recognition can lead to prolonged harmful exposure, contributing to morbidity, health care utilization, and increased costs.
This post aims to provide a framework for identifying drug interactions in the emergency department and highlight drugs and drug classes that should not be missed during our patient encounters. Remember, the dose and duration of medication is a significant variable in considering drug interactions.
Pharmacology Basics
In general, drug interactions can be split into pharmacokinetics and pharmacodynamic interactions
Pharmacokinetics: what our body does to the drug
- Example: how it’s absorbed, distributed, metabolized and excreted
Pharmacodynamics: how the drug effects our body
- Example: direct effect on receptors, interference with biological or physiological control processes, and additive or opposed pharmacological effects.
Types of Drug Interactions

There are many types of drug interactions, we’re primarily going to focus on the bottom 3 in this post
Drug – Food Interactions
Common drug-food interactions exist with fruits, dairy, vitamin K, tyramine foods & alcohol. A notable drug-food interaction to be aware of is grapefruit, with over 85 medication interactions.

(Vuong et al. 2023)
Drug – Disease Interactions
As you can imagine, susceptibility to drugs is at least partly explained by differences in multi-morbidity. Kidney disease makes individuals more susceptible to adverse drug reactions due to a reduction in renal elimination/clearance. Similarly, liver disease and cardiac disease affect hepatic blood flow which may affect drug metabolism.

Midlöv et al. 2020
Drug – Drug Interactions
There are countless out there, however, let’s focus on some clinically significant drug interactions in the ED.
Let’s break it down into 2 different approaches based on patient encounters:
- By presentation when undifferentiated, termed here as the “mimickers”
- By suspected culprit or drug agent referred to as “offending agents”
Mimickers
Here are some common presentations in the ED in which we should be wary of drug interactions, particularly if patients are on multiple medications, or recently had a change/addition of new medications:

Offending Agents
Let’s go over some offending agents to keep on our radar.
- QT Prolongation
Several classes of medications are well known to cause QT prolongation.
We can take different approaches, one is by drug class and recognizing the higher risk medications within those drug classes, such as what is seen in the table below. The other is by mnemonics such as the “Anti’s” that assist in recall of broad drug classes to consider in your differential.


Special Considerations
1. Ondansetron
Ondansetron is considered one of the most commonly used drugs in the ED. Studies have examined single-use IV Ondansetron in the ED and its effects on inducing QT prolongation. It has been shown that a single 4 mg IV ondansetron injection can increase the QTc interval in adult ED patients within a few minutes by 1.6 up to 30ms.
However, the findings across studies are conflicting and there is a lack of sufficient information in an ED setting to establish clear cutoffs & recommendations for IV Ondansetron use, especially with patients without known long QT risk factors.
In general, here are some considerations:
- Screening prior ECGs of patients particularly with the addition of a new medication
- Be mindful of the dose used for IV administration in patients with high-risk backgrounds/ Risk factors
- For non high-risk groups for QTc prolongation consider:
- If prior ECG QTc >460ms then repeat ECG for current visit prior to drug administration & consider optimizing electrolytes (K > 4, Mg > 1)
- If QTc interval < 400ms generally IV Ondansetron administration up to 8mg is safe
2. Trimethoprim/Sulfamethoxazole (TMP-SMX)
Septra/Bactrim deserves special attention for drug interactions as it really doesn’t play nice with others. In combination with certain medications, it can lead to a 7 to 12-fold increased risk of hospitalization due to hyperkalemia. It’s encouraged to consider the use of alternative antibiotics such as amoxicillin where possible, particularly in patients with existing comorbidities (e.g. renal disease).

3. Warfarin
Warfarin is one of those drugs that often set off warning bells in our minds when we see it on a patient’s medication list.
As the list of potential drug interactions seems endless, 2 ways we can approach drug interactions with warfarin in the ED that is less overwhelming is either by:
Mechanism of injury
- Platelet function (e.g. antiplatelet, SSRI)
- Gastrointestinal mucosal injury (e.g. NSAIDs)
- Reduced synthesis of vitamin K (e.g. antibiotics)
- Interference with warfarin metabolism (e.g. acetaminophen)
For those who enjoy lists and mnemonics as memory aids, another approach more easily digestible is the “8 A’s” mnemonic which if we distill it down even more to the most commonly occurring A’s that would be encountered in the ED, the “3 A’s”

Keep in mind it doesn’t necessarily contraindicate the use of these medications but to keep it on your differential as a cause for bleeding and recognize to counsel patients on appropriate follow-up for monitoring of their INR if they are taking these medications.
Additional Drug-Drug Interactions to know
The table below highlights a few more common drug-drug interactions encountered in the ED to keep in mind:

Though we may not commonly prescribe some of these medications (e.g. daptomycin), we may encounter patients who are on these medications with the unfortunate side effects when combining these drugs.
Analgesics
Analgesics, whether prescribed or OTC (e.g. acetaminophen, ibuprofen, ASA) are among the most frequently utilized medications. It’s hard for us to know whether patients are using them or if they are following the prescribed doses and timing.
The table highlights common drug interactions to keep in mind, some of which may not be as well-known such as combined use of NSAIDs and antidiabetics, particularly sulfonylureas leading to hypoglycemia.

Cardiovascular Drugs
A few drug-drug interactions to bear in mind as often these patients are at higher risk as they are typically multimorbid with multiple medication regimens.

Nirmatrelvir/Ritonavir: ‘Paxlovid’
The table below provides an overview of common drugs in the ED that may interact with Paxlovid (let’s ignore the lack of evidence for Paxlovid for the sake of discussion). In cases with contraindications, its suggested to either temporarily stop the home medication for the duration of the Paxlovid prescription (total 5days) or to choose an alternative treatment option during use (e.g. ticagrelor change to prasugrel).
Paxlovid is excreted renally, therefore is it not recommended for those with severe renal disease (e.g. decrease GFR <30ml/min).

Summary
Drug interactions are common and can often be missed in patients presenting to the ED, so a good history and review of medications is key.
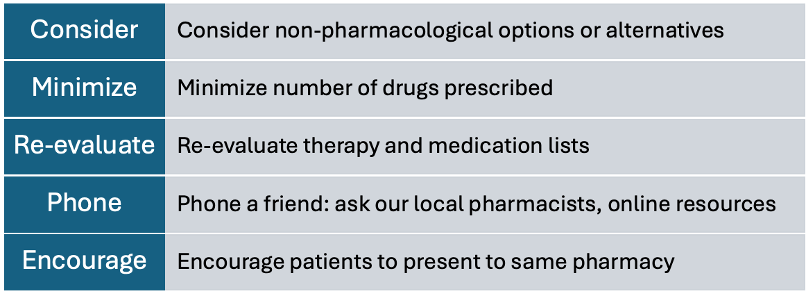
It’s easy to say that drug interactions should always be considered in any ED presentation, but this approach isn’t practical and extremely challenging given the fast-paced environment. It’s unrealistic to expect us to memorize every possible interaction for every medication, so strategies to keep in mind:
References
- Jawaro T, Bridgeman PJ, Mele J, Wei G. Descriptive study of drug-drug interac- tions attributed to prescriptions written upon discharge from the emergency department. Am J Emerg Med. 2019 May;37(5):924–7.
- Zed PJ, Abu-Laban RB, Balen RM, et al. Incidence, sever- ity and preventability of medication-related visits to the emergency department: a prospective study. Can Med Assoc J 2008;178:1563–9.
- Hohl CM, Badke K, Zhao A, Wickham ME, Woo SA, Sivilotti MLA, Perry JJ. Prospective Validation of Clinical Criteria to Identify Emergency Department Patients at High Risk for Adverse Drug Events. Acad Emerg Med. 2018 Sep;25(9):1015-1026. doi: 10.1111/acem.13407. PMID: 29517818; PMCID: PMC6175415.
- Classen D, Pestotnik S, Evans S, Lloyd J, Burke J. Adverse drug events in hospitalized patients. J Am Med Assoc 1997;277:301–6.
- Bates D, Spell N, Cullen D, et al. The costs of adverse drug events in hospitalized patients. JAMA 1997;277:307–11.
- Helman, A. (2024, April 3). EP 184 Must know Drug interactions in emergency medicine. Emergency Medicine Cases. https://emergencymedicinecases.com/drug-interactions-emergency-medicine/
- Gaddis GM, Holt TR, Woods M. Drug interactions in at-risk emergency department patients. Acad Emerg Med 2002;9(11):1162–7.
- Jawaro T, Bridgeman PJ, Mele J, Wei G. Descriptive study of drug-drug interactions attributed to prescriptions written upon discharge from the emergency department. Am J Emerg Med. 2019 May;37(5):924-927. doi: 10.1016/j.ajem.2019.01.049. Epub 2019 Jan 30. PMID: 30880039.
- De Paepe P, Petrovic M, Outtier L, Van Maele G, Buylaert W. Drug interactions and adverse drug reactions in the older patients admitted to the emergency department. Acta Clin Belg 2013;68(1):15–21.
- Pasina L, Djade CD, Nobili A, Tettamanti M, Franchi C, Salerno F, et al. Drug– drug interactions in a cohort of hospitalized elderly patients. Pharmacoepi- demiol Drug Saf. 2013;22(10):1054–60.
- What is a Drug Interaction? | NIH. (n.d.). https://hivinfo.nih.gov/understanding-hiv/fact-sheets/what-drug-interaction
- Vuong M, González Aragón C, Montarroyos SS. Common Food and Drug Interactions. Pediatr Rev. 2023 Feb 1;44(2):68-80. doi: 10.1542/pir.2022-005641. PMID: 36720679.
- Ased S, Wells J, Morrow LE, Malesker MA. Clinically Significant Food-Drug Interactions. Consult Pharm. 2018 Nov 1;33(11):649-657. doi: 10.4140/TCP.n.2018.649.. PMID: 30458907.
- Deng J, Zhu X, Chen Z, Fan CH, Kwan HS, Wong CH, Shek KY, Zuo Z, Lam TN. A Review of Food-Drug Interactions on Oral Drug Absorption. Drugs. 2017 Nov;77(17):1833-1855. doi: 10.1007/s40265-017-0832-z. PMID: 29076109.
- Barbhaiya RH, Welling PG. Influence of food on the absorption of hydrocortisone from the gastrointestinal tract. Drug Nutr Interact. 1981;1(2):103–12.
- Melander A, Brante G, Johansson O, Lindberg T, Wahlin-Boll E. Influence of food on the absorption of phenytoin in man. Eur J Clin Pharmacol. 1979;15(4):269–74.
- Stampfuss J, Kubitza D, Becka M, Mueck W. The effect of food on the absorption and pharmacokinetics of rivaroxaban. Int J Clin Pharmacol Ther. 2013;51(7):549–61.
- Rutgeerts Stead H, taglandin intestinal P, Vantrappen G, Hiele M, Choos Y, Thompson D, et al., editors. Postprandial administration of pros- (misoprostol) products less adverse-effects on transit than its preprandial administration Gastroen- terology. Philadelphia: WB Saunders Co-Elsevier Inc.; 1988.
- Heringa, M., Floor-Schreudering, A., Tromp, P. C., de Smet, P. A., and Bouvy, M. L. (2016). Nature and frequency of drug therapy alerts generated by clinical decision support in community pharmacy. Pharmacoepidemiol. Drug Saf. 25, 82–89. doi: 10.1002/pds.3915
- Midlöv P. Pharmacokinetics and pharmacodynamics in the elderly. OA Elderly Medicine 2013 Aug 01;1(1):1.
- Kerremans A, Kremers B, de Leeuw M, Olthoff MV, Pham TK, Valentijn-Robertz R, Tsoi K, Wichers I, de Wit M, Borgsteede SD. The Development of Practice Recommendations for Drug-Disease Interactions by Literature Review and Expert Opinion. Front Pharmacol. 2020 May 15;11:707. doi: 10.3389/fphar.2020.00707. PMID: 32499701; PMCID: PMC7243438.
- Bénard-Laribière A, Miremont-Salamé G, Pérault-Pochat M-C, Noize P, Haramburu F. The EMIR study group on behalf of the French network of pharmacovigilance centres. Incidence of hospital admissions due to adverse drug reactions in France: the EMIR study. Fundam Clin Pharmacol. 2015;29:106-111.
- Dechanont S, Maphanta S, Butthum B, Kongkaew C. Hospital admissions/visits associated with drug–drug interactions: a systematic review and meta-analysis. Pharmacoepidemiol Drug Saf. 2014;23:489-497.
- Becker ML, Kallewaard M, Caspers PWJ, Visser LE, Leufkens HGM, Stricker BHC. Hospitalisations and emergency depart- ment visits due to drug-drug interactions: a literature review. Pharmacoepidemiol Drug Saf. 2007;16:641-651.
- Olivier P, Bertrand L, Tubery M, Lauque D, Montastruc J-L, Lapeyre-Mestre M. Hospitalizations because of adverse drug re- actions in elderly patients admitted through the emergency department: a prospective survey. Drugs Aging. 2009;26:475-482.
- Jamie L. Thompson, P. C. P. C. R. H. S. C. (2007, February 20). Drug-induced qt prolongation. U.S. Pharmacist – The Leading Journal in Pharmacy. https://www.uspharmacist.com/article/drug-induced-qt-prolongation
- Jacobsen, S. (2022, August 17). The 6 Sulfamethoxazole / Trimethoprim (Bactrim) Interactions You Should Know About. GoodRx. https://www.goodrx.com/sulfamethoxazole-trimethoprim/interactions
- Juurlink D. Drug interactions with warfarin: what clinicians need to know. CMAJ. 2007;177(4):369-371. [PubMed]
- MD, D. H. (2015, March 5). Drug interactions with warfarin: Don’t bleed me out! ALiEM. https://www.aliem.com/drug-interactions-with-warfarin-dont-bleed-me-out/
- Greenblatt D, von M. Interaction of warfarin with drugs, natural substances, and foods. J Clin Pharmacol. 2005;45(2):127-132. [PubMed]
- Marino A, Capogrosso-Sansone A, Tuccori M, Bini G, Calsolaro V, Mantarro S, Convertino I, Pasqualetti G, Orsitto E, Santini M, Monzani F, Blandizzi C; ANCESTRAL-ED Study Group. Expected and actual adverse drug-drug interactions in elderly patients accessing the emergency department: data from the ANCESTRAL-ED study. Expert Opin Drug Saf. 2016 Dec;15(sup2):45-50. doi: 10.1080/14740338.2016.1221400. PMID: 27875918.
- Fendrick AM, Pan DE, Johnson GE. OTC analgesics and drug interactions: clinical implications. Osteopath Med Prim Care. 2008 Feb 7;2:2. doi: 10.1186/1750-4732-2-2. PMID: 18257920; PMCID: PMC2257951.
- Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA: Recent patterns of medication use in the ambulatory adult population of the United States: the Slone survey. JAMA 2002, 287:337-344.
- Krauss E, Cronin M, Dengler N, Segal A. Interaction Between Low-Dose Aspirin and Nonsteroidal Anti-Inflammatory Drugs Can Compromise Aspirin’s Efficacy in Preventing Venous Thrombosis Following Total Joint Arthroplasty. Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620920373. doi: 10.1177/1076029620920373. PMID: 32453611; PMCID: PMC7370567.
- Abraham S, Nohria A, Neilan TG, Asnani A, Saji AM, Shah J, Lech T, Grossman J, Abraham GM, McQuillen DP, Martin DT, Sax PE, Dani SS, Ganatra S. Cardiovascular Drug Interactions With Nirmatrelvir/Ritonavir in Patients With COVID-19: JACC Review Topic of the Week. J Am Coll Cardiol. 2022 Nov 15;80(20):1912-1924. doi: 10.1016/j.jacc.2022.08.800. Epub 2022 Oct 12. PMID: 36243540; PMCID: PMC9580069.
- Al Hamid A, Ghaleb M, Aljadhey H, Aslanpour Z. A systematic review of hospitalization resulting from medicine-related problems in adult patients. Br J Clin Pharmacol. 2014;78(2):202–217.
- Cheung JTK, Yu R, Woo J. Is polypharmacy beneficial or detrimental for older adults with cardiometabolic multimorbidity? Pooled analysis of studies from Hong Kong and Europe. Fam Pract. 2020;37(6):793–800.
- Carpenter M, Berry H, Pelletier AL. Clinically Relevant Drug-Drug Interactions in Primary Care. Am Fam Physician. 2019 May 1;99(9):558-564. PMID: 31038898.
- Leong D, Wu PE. Warfarin and acetaminophen interaction in a 47-year-old woman. CMAJ. 2020 May 11;192(19):E506-E508. doi: 10.1503/cmaj.191532. PMID: 32575041; PMCID: PMC7234266.
- Hohl CM, Zed PJ, Brubacher JR, Abu-Laban RB, Loewen PS, Purssell RA. Do emergency physicians attribute drug-related emergency department visits to medication-related problems? Ann Emerg Med. 2010 Jun;55(6):493-502.e4. doi: 10.1016/j.annemergmed.2009.10.008. Epub 2009 Dec 11. PMID: 20005010.
- Rezaei Zadeh Rukerd M, Shahrbabaki FR, Movahedi M, Honarmand A, Pourzand P, Mirafzal A. Single intravenous dose ondansetron induces QT prolongation in adult emergency department patients: a prospective observational study. Int J Emerg Med. 2024 Apr 2;17(1):49. doi: 10.1186/s12245-024-00621-5. PMID: 38566008; PMCID: PMC10988934.