
In case you missed it, in part 1 of this series, Dr. Zworth discussed the increasing prevalence of invasive Group A Strep (iGAS), the mounting public health concern, recognition, and diagnosis. In this post, we focus on management, the treatment of (strep) pharyngitis, and post-exposure prophylaxis.
Take home #5: The four pillars of iGAS management include:
- Usual sepsis care
- Specific antibiotic therapy
- Source control
- Consider IVIG
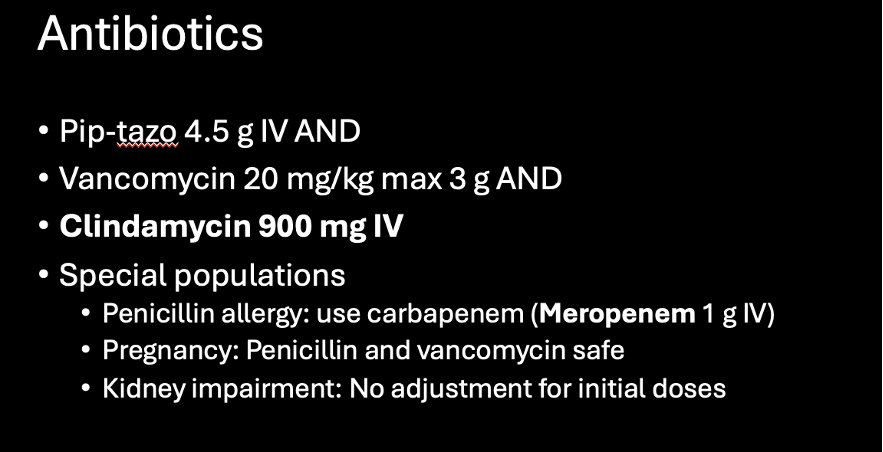
Interestingly, iGAS remains universally susceptible to penicillins. So even for invasive disease, penicillins are the mainstay of therapy. In patients who are penicillin allergic, a carbapenem is recommended as another beta-lactam agent.1
Secondly, remember that in the emergency department, we actually won’t have a diagnosis of invasive group A strep on our assessment. So vancomycin is included as part of your cocktail for the shocky septic patient, empirically covering against MRSA. Particularly in necrotizing SSTI, s. aureus is also implicated, so it’s important we include MRSA coverage.
Clindamycin is a critical component of our management of iGAS infections for a few reasons. Firstly, its effectiveness is not affected by bacterial loads. While penicillins work very well against GAS, its efficacy is limited by something called the “inoculum effect” where large bacterial loads reduce its effectiveness. This is not true for clindamycin. Secondly, clindamycin inhibits bacterial toxin production, which is a major component of the toxic shock syndrome that develops in iGAS infections.1,5
Finally, there is evidence that clindamycin significantly reduces mortality. In one retrospective study of 2000 iGAS infections in the US from 2000 to 2015, mortality was 6.5% in patients who received clindamycin compared to 11% in patients who received a beta-lactam alone.13
It’s worth pointing out that we have begun to see some resistance of GAS to clindamycin. Resistance rates have increased from 1% in 2000 to 15% in 2015 in the US.14 In China up to 97% of isolates are resistant to clindamycin.15 For now, clindamycin remains a mainstay of therapy here in North America.
Next, as we know source control is critical in the patient with iGAS. In the case of necrotizing soft tissue infections, this means urgent surgical consultation.
I recommend referring to your hospital’s policy regarding necrotizing fasciitis, as the appropriate surgical service will depend on the body part involved. In some cases, you may have a consulting service ask you to obtain a CT scan to further assess for necrotizing fasciitis. If this happens, we need to be collegial. As we discussed, imaging may be helpful to the surgeon. I would say something like: “Absolutely I can order a CT and speak to radiology but I also need you to see this patient to offer your opinion.”
I asked Dr. Jacob Hardy, a Plastic Surgery resident at the University of Ottawa, for his perspective on getting our surgeons involved when we suspect necrotizing fasciitis. And he had this to say:
“Nec fasc is a surgical disease. It requires prompt identification and prompt surgical debridement to avoid amputation and death. Whenever we see cellulitis in an unstable patient, nec fasc must be assumed. In order to not miss nec fasc, I think I must be willing to examine some patients who don’t end up having nec fasc and sometimes even taking patients to the OR who don’t end up having nec fasc. A trigger happy approach is reasonable in these cases as while OR is not benign, the implications of missing nec fasc are so severe that they easily outweigh these.”
I want to underline this point – it’s ok to have over-calls / false positives on necrotizing fasciitis. There should be instances where you ask your consultant to come assess the patient, and it does not end up being necrotizing fasciitis. If your hit rate is 100%, you are likely missing cases.
Finally, let’s talk about IVIG in iGAS infections. In 2018, Parks and colleagues conducted a systematic review and meta-analysis of prospective studies comparing IVIG to no IVIG in patients being treated with clindamycin for streptococcal toxic shock syndrome. Their primary outcome was 30-day mortality. They found that in every study, there was lower overall mortality in the IVIG group. However, due to low case numbers, none of the studies reached statistical significance in isolation. But when they conducted a pooled analysis, they did find that IVIG reduced mortality from 33.7 to 15.7 percent. 16
Due to limited available data, IDSA currently says that further research is needed before a recommendation can be made. However, you should consider it in patients with signs of severe disease.
Note that if you are giving IVIG in Ontario, you are required to fill out a Ministry of Health form. It is recommended to use a dose calculator for the patient, based on their height and weight, which is linked to in the form. This form is sent to transfusion medicine.
Take home #6: Despite rising cases of iGAS, the management of pharyngitis remains unchanged (for now).
There is no great evidence about the association between GAS pharyngitis and iGAS infections – so this section is going to have a lot of caveats. Probably the best summary of evidence regarding risk factors for iGAS infections in children comes from a scoping review performed by Mariani et al and published in 2023. They performed a scoping review according to PRISMA guidelines. They included 209 studies in total, and found only 5 studies that had performed multivariate analyses of risk factors of iGAS cases. There were no studies that reported a positive Group A strep test prior to the onset of iGAS (in the source patient).17
They concluded: “In 2023, we are still unaware if a diagnosis of iGAS is preceded by a non-invasive infection (or colonization) with GAS… It is completely unknown if low thresholds for testing and treating GAS may have any effect on reducing iGAS incidence”.17
There are some important limitations to point out in this study. Only 5 studies included multivariate analyses of iGAS. These 5 studies ranged from 2000-2015, so none really captured the new M1UK strain that emerged in 2015. This study is only in pediatric patients. As we’ve said, the group with the highest incidence of iGAS are those over the age of 60.
So should we approach pharyngitis any differently in an age of increasing iGAS rates?
As a reminder, the majority (80%) of pharyngitis will be viral. Additionally, we are already prescribing too many antibiotics. Antibiotics for sore throats make up 5% of all antibiotic prescriptions in Canada. In Canada, on average 7 antibiotic prescriptions are written for pharyngitis every 100 adults per year, and only 50% of these are for confirmed GAS.18 Moreover, distinguishing GAS from viral pharyngitis is not easy!
The best tool we have to assist us with making the diagnosis is the McIsaac Criteria (or Modified Centor score), which most of us will remember learning in medical school.
Large-scale validation of the modified criteria was done in 200,000 patients in the US as recently as 2012 and this score is still recommended for use in guidelines from the Canadian Pediatric Society and by the UK’s National Institute for Health Care Excellence guidelines in evaluation of sore throat.19 BUT, we should also qualify this and point out that the McIsaac / Centor criteria were based on data of older variants of GAS, and have not been validated on more recent data.

As you can see below even a McIsaac score of 4 (adult with fever, no cough, anterior cervical lymphadenopathy and tonsillar exudate) will still only be GAS positive 57% of the time – barely better than half!19

Even if we can make the diagnosis, the question remains, do we actually need to treat GAS pharyngitis? We know that up to 15% of children who test positive for GAS are asymptomatic carriers. So we will be treating viral pharyngitis in many patients, which then risks only the side effects of antibiotics.20 We also know from a recent Cochrane review that 80% of patients with sore throat will be asymptomatic by 1 week even without treatment.21 So what we really think we are treating is complications of strep pharyngitis. Antibiotics have been shown in prospective studies and in Cochrane reviews to reduce the risk of suppurative complications (ex otitis media, peritonsillar abscess). However, the risk of these complications is low (about 1%) and the NNT is accordingly in the range of 1 in 200.20,21
The rates of post-Strep GN and rheumatic fever are so low that in more recent studies, it is not possible to evaluate whether antibiotics reduce the risk of complications. Rheumatic fever rates were reduced with antibiotics, but this was primarily in older studies and in a cohort (i.e. military) where the rates of rheumatic fever were high. But again another caveat – the data we have on the natural history of GAS is based on older variants of GAS – so we’re applying pre-surge data to our current situation.
I asked Dr. Chowdhury about the potential association with GAS pharyngitis and iGAS, and he had the following to say”
“I don’t think [GAS pharyngitis] is a major player in iGAS infections. Anecdotally it seems like one could lead to the other, but statistics-wise wise we’re just not seeing this yet. The spike we have seen in scarlet fever does suggest an increase in virulence. And there are some anecdotes about increased rates of rheumatic fever, but we’re not seeing this yet in the data… I wouldn’t do anything differently for pharyngitis workup and management”.
Dr. Yadav took a similar approach:
“We have to be careful. There is no clear association, let alone established causation between [GAS pharyngitis and iGAS]. But let’s pretend there were. What would this change clinically? Does this mean anyone with a sore throat should get antibiotics? If we dramatically increase our antibiotic prescribing, we are going to get resistance. I don’t think we should be changing our practice.”
We have two approaches to choose from for pharyngitis in adults. The first is that recommended by the Infectious Disease Society of America (IDSA) in 2012. IDSA doesn’t recommend any score or clinical decision tool. They suggest that if clinical features alone are not enough, (which they usually aren’t), then we use a throat swab or RADT, and treat if this is positive. As you can see below, the accuracy of these tests is quite good.22

The alternative approach, and the guideline that probably mirrors our practice pattern in Canada, is the National Institute of Health Care Excellence Guideline, published in the UK in 2018. This approach recommends using either the Centor criteria or a very similar score called Fever Pain, and recommends that in patients with a high probability of GAS, it is reasonable to prescribe antibiotics without swabbing.
Approach – Nice 201823

Take home #7: Only close contacts require chemoprophylaxis for iGAS exposure. First line treatment for prophylaxis is cephalexin 500 mg po QID for 10 days.
We’ve learned when to expect iGAS infections, and we know how to manage them. But what do we do about patients or healthcare workers who were in contact with confirmed iGAS cases?
Let’s talk briefly about why to consider prophylaxis in iGAS. There is evidence that the rate of iGAS in household contacts is way higher than in the general population. The attack rate of iGAS in household contacts is estimated to be 66 – 294 / 100,000
(4 cases out of 1360 exposed people) compared with ~ 4 / 100,000 in the general population.24,25 These numbers are based on 2 studies with very limited case numbers – for example, an Ontario study of 1360 people who were household contacts of iGAS found only 4 people actually developed an iGAS infection.24 But they still inform the PHAC guideline and CPS statement on chemoprophylaxis.
It’s also worth giving the caveat that we have very little data on the effectiveness of prophylaxis. There is a signal that prophylaxis decreases the risk of infection. But the studies we have are based on large sample sizes with fairly weak methodology.
The current PHAC guideline recommendations are that prophylaxis only be given to people who are considered ‘close contacts’. Prophylaxis is not needed for school classmates, work colleagues, or sports contacts.20

Two special situations warrant mentioning:
- Child Care Centres
- Home Daycare: Prophylaxis is needed for all staff and attendees if 1 severe case
- Institutional: Prophylaxis is indicated for all if > 1 case of confirmed iGAS
- Long Term Care facilities
- All residents and staff require screening
- All staff interacting with patients without PPE require prophylaxis
Occupational Exposures
Transmission of GAS is through large droplets. An occupational exposure of a HCW is defined as secretions from the nose, mouth, wound, or skin infection of the infected case coming into contact with the mucous membranes or non-intact skin of the HCW from within 7 days before the onset of GAS until 24 hours of effective antibiotic therapy. So just being in the same room as a patient without PPE does not count as an exposure. If in doubt, talk with your occupational health department to determine if you require prophylaxis.
Recommended protocols for chemoprophylaxis are shown below. First line treatment for prophylaxis is Keflex at a dose of 500 mg QID for a total of 10 days.

References
- Waddington CS, Snelling TL, Carapetis JR. Management of invasive group A streptococcal infections. J Infect. 2014;69 Suppl 1:S63-69. doi:10.1016/j.jinf.2014.08.005
- Streptococcal Toxic Shock Syndrome (STSS) (Streptococcus pyogenes) 2010 Case Definition | CDC. Published June 11, 2021. Accessed June 29, 2024. https://ndc.services.cdc.gov/case-definitions/streptococcal-toxic-shock-syndrome-2010/
- Kaul R, McGeer A, Low DE, Green K, Schwartz B. Population-based surveillance for group A streptococcal necrotizing fasciitis: Clinical features, prognostic indicators, and microbiologic analysis of seventy-seven cases. Ontario Group A Streptococcal Study. Am J Med. 1997;103(1):18-24. doi:10.1016/s0002-9343(97)00160-5
- Stevens DL, Tanner MH, Winship J, et al. Severe group A streptococcal infections associated with a toxic shock-like syndrome and scarlet fever toxin A. N Engl J Med. 1989;321(1):1-7. doi:10.1056/NEJM198907063210101
- Carapetis JR, Jacoby P, Carville K, Ang SJJ, Curtis N, Andrews R. Effectiveness of clindamycin and intravenous immunoglobulin, and risk of disease in contacts, in invasive group a streptococcal infections. Clin Infect Dis Off Publ Infect Dis Soc Am. 2014;59(3):358-365. doi:10.1093/cid/ciu304
- Nelson GE, Pondo T, Toews KA, et al. Epidemiology of Invasive Group A Streptococcal Infections in the United States, 2005-2012. Clin Infect Dis Off Publ Infect Dis Soc Am. 2016;63(4):478-486. doi:10.1093/cid/ciw248
- Miller LG, Eisenberg DF, Liu H, et al. Incidence of skin and soft tissue infections in ambulatory and inpatient settings, 2005-2010. BMC Infect Dis. 2015;15:362. doi:10.1186/s12879-015-1071-0
- Walker MJ, Barnett TC, McArthur JD, et al. Disease Manifestations and Pathogenic Mechanisms of Group A Streptococcus. Clin Microbiol Rev. 2014;27(2):264-301. doi:10.1128/CMR.00101-13
- Lynskey NN, Jauneikaite E, Li HK, et al. Emergence of dominant toxigenic M1T1 Streptococcus pyogenes clone during increased scarlet fever activity in England: a population-based molecular epidemiological study. Lancet Infect Dis. 2019;19(11):1209-1218. doi:10.1016/S1473-3099(19)30446-3
- Alcolea-Medina A, Snell LB, Alder C, et al. The ongoing Streptococcus pyogenes (Group A Streptococcus) outbreak in London, United Kingdom, in December 2022: a molecular epidemiology study. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. 2023;29(7):887-890. doi:10.1016/j.cmi.2023.03.001
- Peetermans M, Matheeussen V, Moerman C, et al. Clinical and molecular epidemiological features of critically ill patients with invasive group A Streptococcus infections: a Belgian multicenter case-series. Ann Intensive Care. 2024;14(1):19. doi:10.1186/s13613-024-01249-7
- Fernando SM, Tran A, Cheng W, et al. Necrotizing Soft Tissue Infection: Diagnostic Accuracy of Physical Examination, Imaging, and LRINEC Score: A Systematic Review and Meta-Analysis. Ann Surg. 2019;269(1):58. doi:10.1097/SLA.0000000000002774
- Babiker A, Li X, Lai YL, et al. Effectiveness of adjunctive clindamycin in β-lactam antibiotic-treated patients with invasive β-haemolytic streptococcal infections in US hospitals: a retrospective multicentre cohort study. Lancet Infect Dis. 2021;21(5):697-710. doi:10.1016/S1473-3099(20)30523-5
- DeMuri GP, Sterkel AK, Kubica PA, Duster MN, Reed KD, Wald ER. Macrolide and Clindamycin Resistance in Group a Streptococci Isolated From Children With Pharyngitis. Pediatr Infect Dis J. 2017;36(3):342-344. doi:10.1097/INF.0000000000001442
- Lu B, Fang Y, Fan Y, et al. High Prevalence of Macrolide-resistance and Molecular Characterization of Streptococcus pyogenes Isolates Circulating in China from 2009 to 2016. Front Microbiol. 2017;8:1052. doi:10.3389/fmicb.2017.01052
- Parks T, Wilson C, Curtis N, Norrby-Teglund A, Sriskandan S. Polyspecific Intravenous Immunoglobulin in Clindamycin-treated Patients With Streptococcal Toxic Shock Syndrome: A Systematic Review and Meta-analysis. Clin Infect Dis Off Publ Infect Dis Soc Am. 2018;67(9):1434-1436. doi:10.1093/cid/ciy401
- Mariani F, Gentili C, Pulcinelli V, Martino L, Valentini P, Buonsenso D. State of the Art of Invasive Group A Streptococcus Infection in Children: A Scoping Review of the Literature with a Focus on Predictors of Invasive Infection. Child Basel Switz. 2023;10(9):1472. doi:10.3390/children10091472
- Miller KM, Barnett TC, Cadarette D, Bloom DE, Carapetis JR, Cannon JW. Antibiotic consumption for sore throat and the potential effect of a vaccine against group A Streptococcus: a systematic review and modelling study. EBioMedicine. 2023;98:104864. doi:10.1016/j.ebiom.2023.104864
- Fine AM, Nizet V, Mandl KD. Large-scale validation of the Centor and McIsaac scores to predict group A streptococcal pharyngitis. Arch Intern Med. 2012;172(11):847-852. doi:10.1001/archinternmed.2012.950
- Sauve L, Forrester AM, Top KA. Group A streptococcal pharyngitis: A practical guide to diagnosis and treatment. Paediatr Child Health. 2021;26(5):319-320. doi:10.1093/pch/pxab025
- Spinks A, Glasziou PP, Del Mar CB. Antibiotics for treatment of sore throat in children and adults. Cochrane Database Syst Rev. 2021;12(12):CD000023. doi:10.1002/14651858.CD000023.pub5
- Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis Off Publ Infect Dis Soc Am. 2012;55(10):e86-102. doi:10.1093/cid/cis629
- Overview | Sore throat (acute): antimicrobial prescribing | Guidance | NICE. Published January 26, 2018. Accessed April 30, 2024. https://www.nice.org.uk/guidance/ng84
- Khan F, Bai Z, Kelly S, et al. Effectiveness and Safety of Antibiotic Prophylaxis for Persons Exposed to Cases of Invasive Group A Streptococcal Disease: A Systematic Review. Open Forum Infect Dis. 2022;9(8):ofac244. doi:10.1093/ofid/ofac244
- The Prevention of Invasive Group A Streptococcal Infections Workshop Participants. Prevention of Invasive Group A Streptococcal Disease among Household Contacts of Case Patients and among Postpartum and Postsurgical Patients: Recommendations from the Centers for Disease Control and Prevention. Clin Infect Dis. 2002;35(8):950-959. doi:10.1086/342692
