

While the term ‘God Squad’ reflects a real committee from the 1960s, we use it here critically to examine the risks of unchecked decision-making power in emergency care.
This is a photo of the Admissions and Policy Committee of the Seattle Artificial Kidney Centre, also known as The God Squad. Starting in 1962 and continuing for four years, this group met monthly to decide which one or two out of a dozen patients would receive a groundbreaking, lifesaving invention: dialysis.
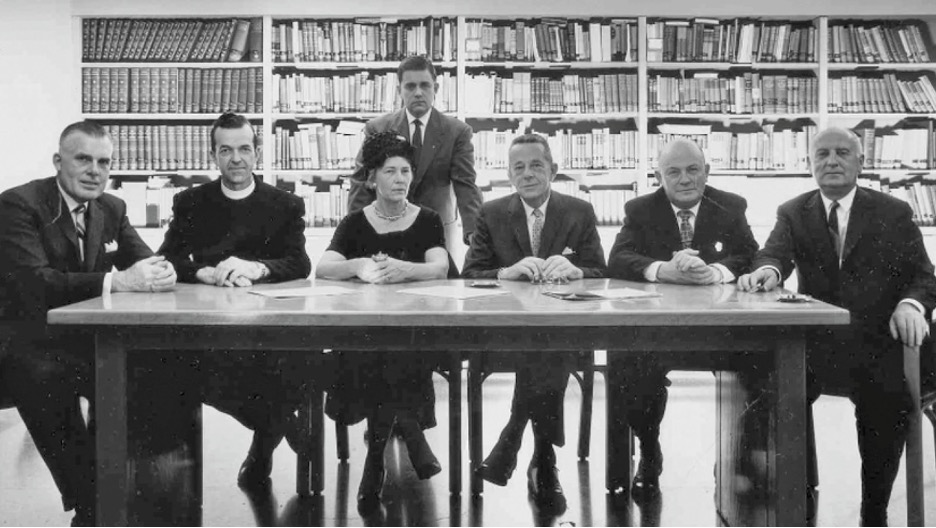
The “God Committee” selecting patients for dialysis. West of the Rotunda—Difficult choices. Available online: http://danschmidtforsenate.com/blog/?p=291 (accessed on August 4, 2025).
They summarized their role as deciding which patient was “worth saving.” Although no formal criteria were laid out, the patients they chose shared strikingly similar characteristics. They were men, under the age of 45, white, with loving wives and young children, regular church attendance, and no underlying mental health concerns. In other words, middle-aged, middle-class white men — people who looked and acted very much like the committee members themselves.
The God Squad was, in essence, doing what we as emergency medicine doctors do every day: triaging. They faced limited resources and an overwhelming need. In our world, the limited resources are physical spaces, monitors, investigations, imaging, and at times, lifesaving interventions. The question is: how are we making these decisions? And are we doing any better than the God Squad?
Why Triage Matters
Triage is one of the most essential and consequential parts of emergency medicine. Without a systemized and evaluated approach, we risk basing our decisions on unconscious biases that make care unfair.
When most people hear “triage,” they picture patients entering the ED, being given a score, and assigned to a zone. But triage is much more than that. It’s how we decide which patient to see first, who needs scans, who requires monitoring, and all the micro-decisions we make throughout a shift.
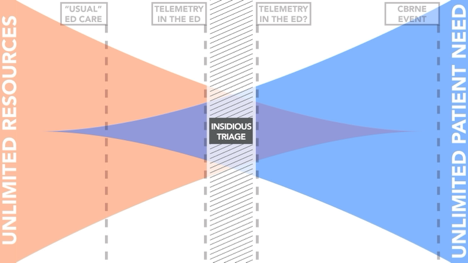
Triage exists on a resource-to-patient continuum:
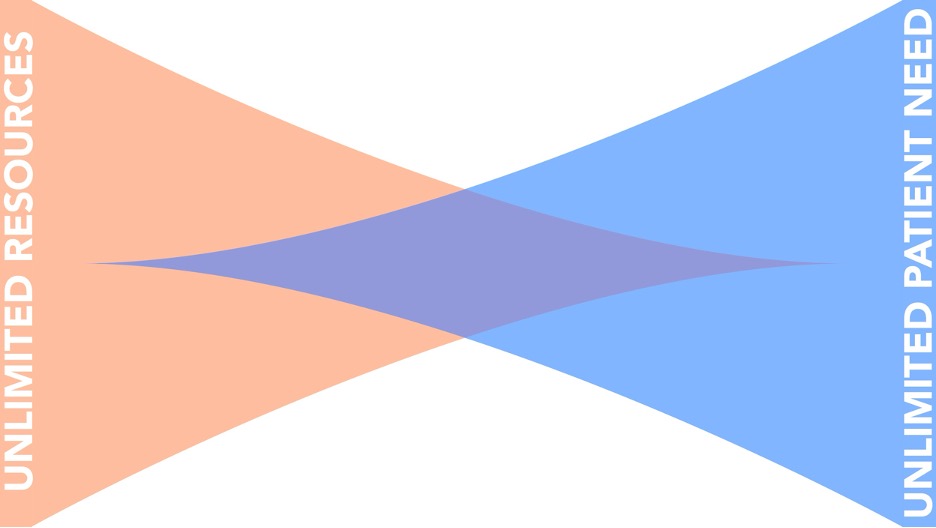
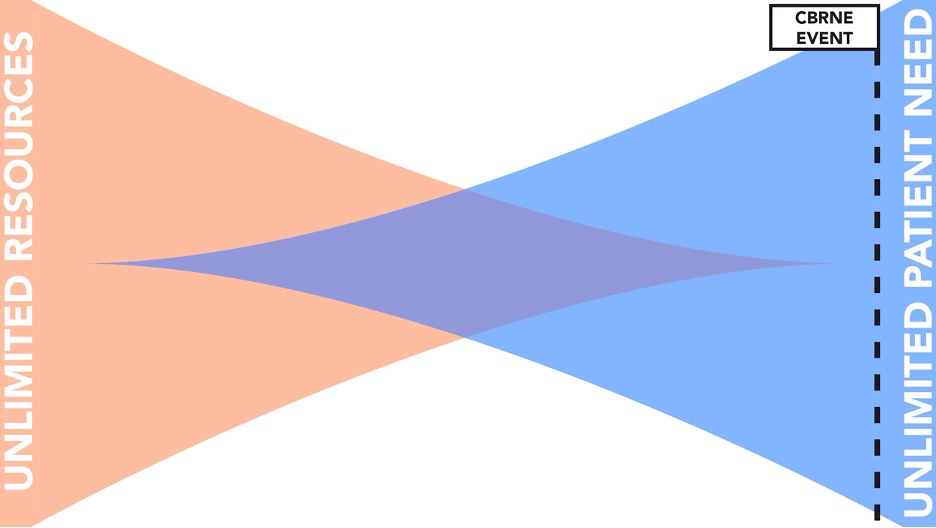
On the far left, resources are plentiful and patient need is low. On the far right, resources are scarce and patient need is extreme. An example of this would be a massive CBRNE event, where for an extended period all our resources have been depleted.
Triage becomes futile at both extremes: when resources are unlimited, or when resources are nonexistent. Since it’s inception in the 1950s, emergency department triage in North America has been seen as being very close to the left end of the spectrum. Resources are thought to be plentiful, and triage is designed to decide when patients are seen, however all patients will be seen and will have their needs taken care of.
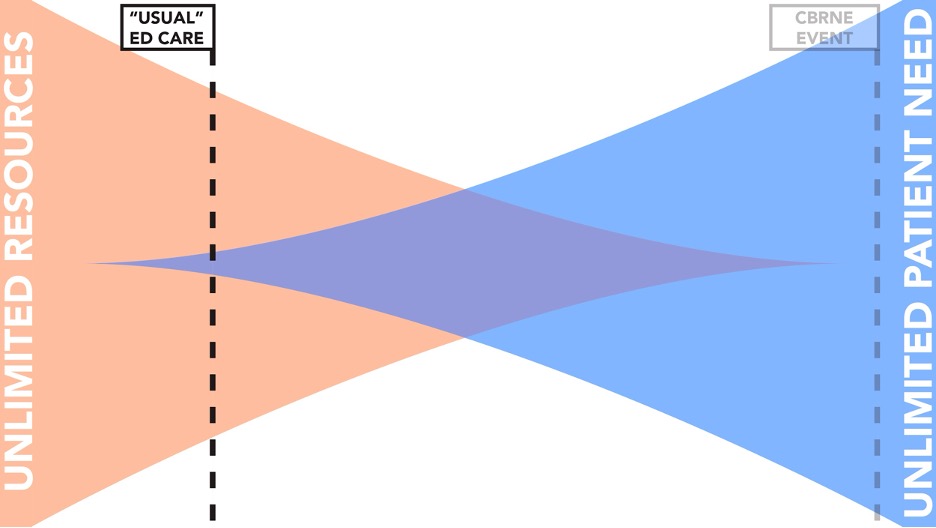
Today, with increasing volumes and shrinking resources, we must ask whether that assumption still holds.
The Monkey-God Spectrum
Another way to look at this spectrum is the monkey god spectrum. We’re teased as emergency room physicians that we are just triage monkeys. Not performing real medicine, but instead managing logistics, and referring to consultants. Which, to be frank, if we are at the left end of the spectrum, is a plausible conclusion. But at the other end of the spectrum, when resources are low and triage decisions have life or death consequences, we can be seen like the Seattle god squad. So where do we fall? And how are we making these decisions?
In speaking with colleagues, I heard a wide variety of answers to questions like: Who do you see first? Who can safely come off monitors? Who needs inpatient scans? Again and again, the word I heard was gestalt.
Gestalt is valuable, but it’s difficult to teach and almost impossible to systematize. My goal is to convince you that triage should move from the subconscious into the deliberate. To be neither apes nor deities, we must be systematic and purposeful — or risk decisions driven by haphazard, emotional, and unfair factors.
When Triage Fails: The Case of Brian Sinclair
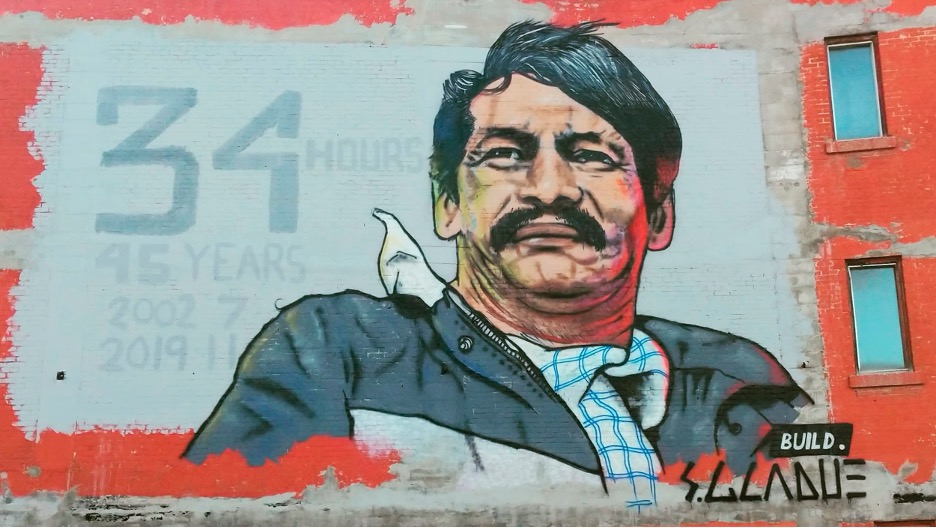
Brian was an Indigenous man living in Winnipeg. In 2008, he presented to Health Sciences Centre with a blocked catheter and died of urosepsis after waiting 34 hours in the ED waiting room. Staff assumed he was intoxicated and “sleeping it off.” By the time he was discovered dead, rigor mortis had already set in. He was just 45 years old.
At the inquiry, the Brian Sinclair Working Group argued that racism led to his preventable death.
CTAS: Strengths and Shortcomings
When we hear the word “triage” what comes to mind is probably the type of triage that failed Brian Sinclair. The type of triage where people enter the emergency department and line up, getting a score and waiting based on their acuity level.
As explained previously, this kind of triage is intended for the far left of our Monkey-God spectrum, where the resource to patient ratio is high. It’s the type of triage that involves more type 1 thinking and algorithms, and is not designed to triage life or death decisions. But what happens when CTAS falls short?
CTAS, introduced in 1999 and used widely across Canada, assigns patients a score based on presenting complaint, vital signs, pain, and other modifiers. While studies show it performs comparably to other systems, it is far from perfect.
Research has shown CTAS often under-triages seniors, women, people of colour, Indigenous patients, and those experiencing homelessness or poverty. For example:
- Older adults are admitted at high rates despite low CTAS scores.
- Women and racialized patients are triaged to lower acuity scores, even when controlling for comorbidities.
- Indigenous patients in Canada are less likely to receive higher acuity scores and wait longer for care.
In other words, CTAS systematically disadvantages the very populations most at risk. Based on the literature, we know that Brian Sinclair is the type of patient that CTAS fails. These studies allow us to state with confidence, that racism and bias led to his death.
Brian Sinclair’s death was not an anomaly — it was part of a broader, documented pattern.
So how can we do better? Following the inquiry, The Brian Sinclair Working Group provided four recommendations. In short, they are that all stakeholders in medicine: the federal government, the provincial health authorities, unions and medical professional groups, as well as universities and medical schools implement anti racism training, cultural safety training, and implicit bias training. These recommendations align with the calls to action from the Truth and Reconciliation Committee.
These are system changes that need to happen on a larger level, but there’s a lot of things we can do as individual partitioners. After reading these studies, my takeaway is that next time I see someone who belongs to one of these demographic groups, I’ll pause and consider if their wait time, and triage score feels appropriate, and reflect on how it might be contributing to my own implicit bias and impacting my decisions for workup and treatment.
Who Needs a Monitor?
Triage isn’t just about who is seen first. It’s also about resource allocation within the ED. One hot-button issue: who should remain on cardiac monitors?
Before answering the question, let’s consider the case of Myron Cybriwski.
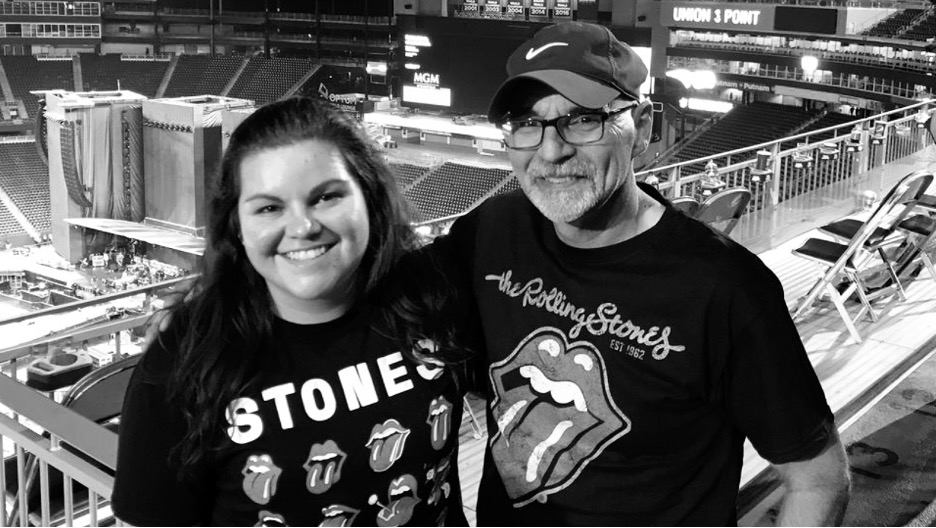
Stephanie Cybriwski (left) and her late father Myron. (Photo courtesy of Stephanie Cybriwski). Taken from: https://www.thelastambulance.com/myron-cybriwskis-legacy/ on August 4, 2025
On May 14, 2022, 65-year-old Myron Cybriwski, recently retired, called 911 from his home in Laval complaining of a headache after a fall. He was told ambulances were backed up and the wait would be long. Eleven hours later, paramedics arrived to find him dead in his bed.
The local health authorities cited too few ambulances and paramedics held up at hospitals. But for Myron, the consequence of delayed care was fatal.
As emergency physicians, we may not control ambulance availability, but our decisions within the department — including who remains on monitors and how we manage flow — have ripple effects that impact patients like Myron waiting for care in the community.
Cardiac monitors influence flow, ambulance offloads, and nursing workload. But they are not benign. Studies show telemetry can increase anxiety, disturb sleep, and contribute to alarm fatigue and even misdiagnosis.
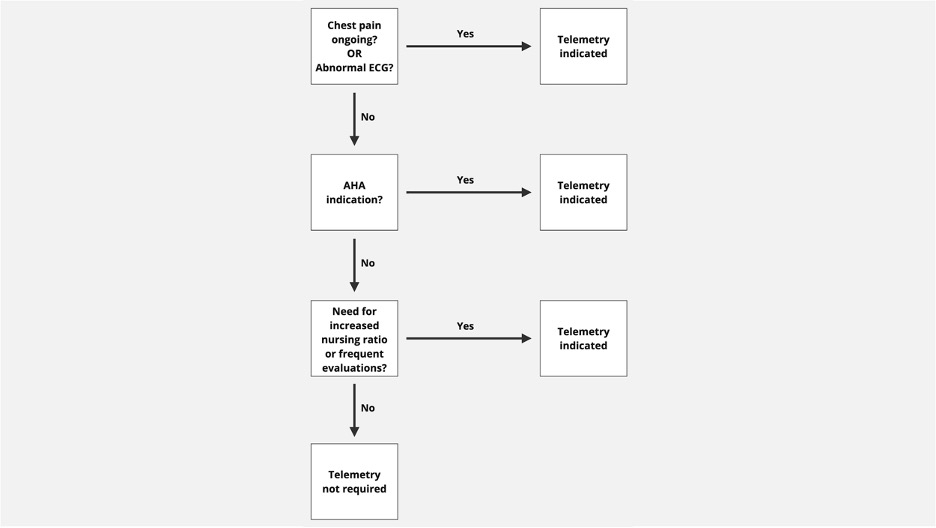
Guidelines recommend telemetry only for specific conditions such as ACS, cardiac syncope, vasoactive medications, or severe electrolyte disturbances. But in practice, monitors are often used more broadly.
A study from our own department (Drs. Syed and Venk) showed that chest pain patients who are pain-free with a normal ECG can safely be managed without telemetry, with 100% sensitivity for detecting arrhythmias in the ED or within eight hours. Implementing this rule could free up monitors and allow paramedics to return to the community more quickly, preventing tragedies like Myron’s.
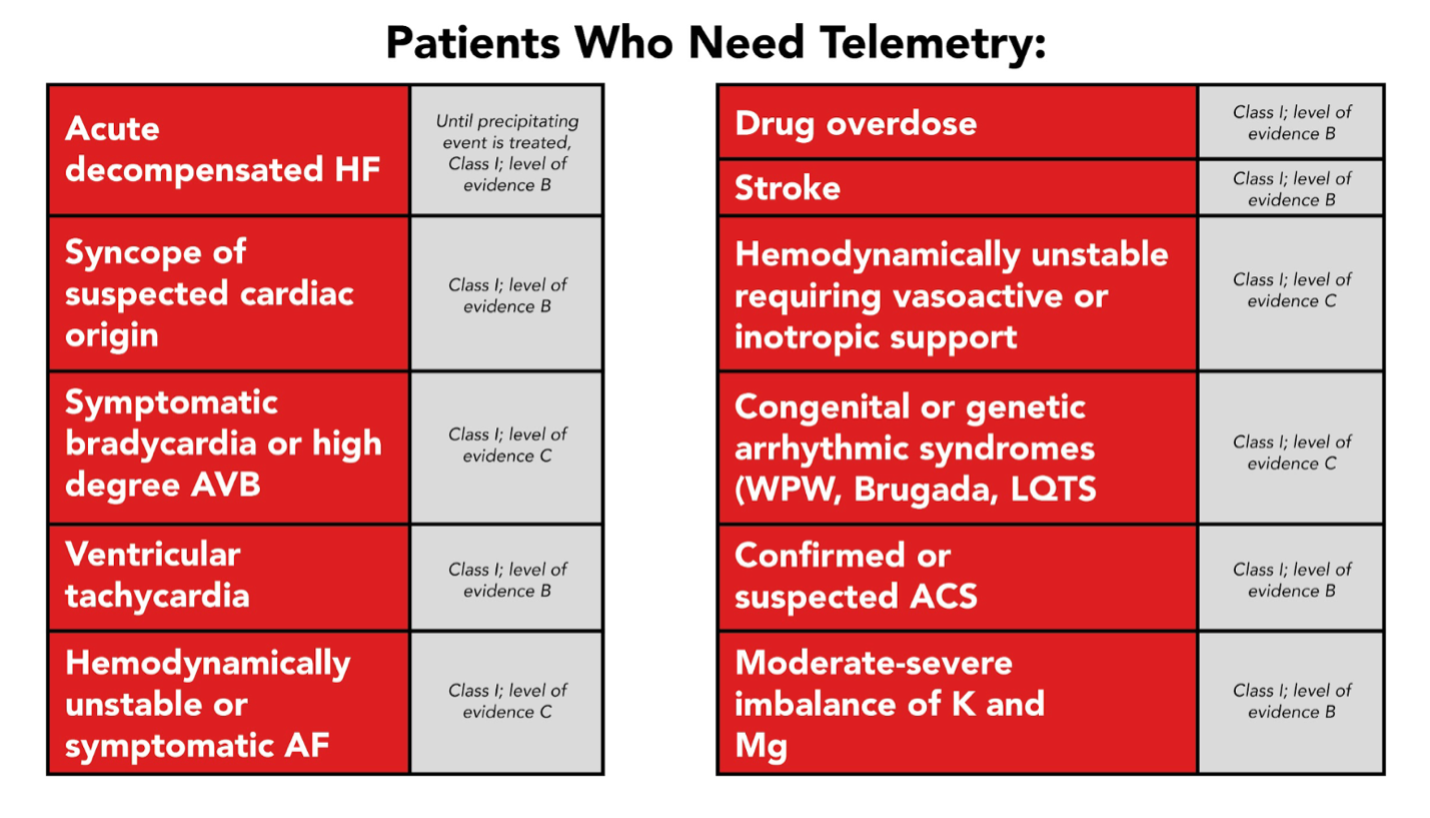
I recognize for us in the emergency department this list is not exhaustive. And that’s because in the ED “monitors” don’t just mean telemetry, but also higher-level nursing care and increased assessments. Given that consideration, I propose the following flowchart:
The Far End of the Spectrum: Emmett Everett and Hurricaine Katrina
In extreme cases, triage becomes life or death. After Hurricane Katrina, Dr. Anna Pou and her colleagues at Memorial Hospital faced unbearable conditions: no power, failing supplies, and temperatures of 43°C. Forced to create an ad hoc triage system, they prioritized healthier patients for evacuation.
Among those left behind was Emmett Everett, a 61-year-old paraplegic man awaiting surgery for chronic bowel obstruction. Weighing 380 pounds and unable to walk, he would have required a group to carry him up the stairs to the helipad in sweltering heat. Reports later suggested he was among those given morphine and midazolam to “make them comfortable” — decisions that remain highly controversial.
Dr. Pou and her colleagues were accused of “playing God.” Their improvised triage model was criticized as ableist, fatphobic, and arbitrary. The case highlights the dangers of insidious triage — decisions made without transparency, protocol, or public involvement.
Dr. Lee Daugherty Biddison, a critical care physician in Marlyand, argues that the best way to mitigate the “doctors as god” complex is via public involvement in triage. She states that “The best plans will fail if the public has not been involved and is unprepared. No system will work if patients and their families reject as unjust life-or-death decisions that seem arbitrary, imposed on them by experts without justification.”
From 2012-2014 Dr. Daugherty Biddison and colleagues conducted community engagement forums in the state of Maryland to gather the public’s opinion related to the allocation of scarce, lifesaving resources. Based off of 15 day long forums involving over 300 people, they came up with a triage system. The nitty gritty of this protocol is beyond the scope of this blog post (but find it linked in the sources if you are curious). In short, patients are given scores based off their short term survival likelihood, long term survival likelihood, and then age is used as a tiebreaker, if needed. [1]
Dr. Daughtery Biddison and her colleagues also emphasized the importance of a triage officer, [2]who makes these decisions and is a separate entity from the care team, to alleviate personal biases, decisions based off emotion, and provider trauma. Dr. Daughtery Biddison said “Our participants were adamant that politicians, and health officials, be transparent and honest about the prospect of and plans for the rationing of ventilators and other equipment. In health emergencies, experts often ask the public to heed the advice of public health professionals; in the case of planning for situations involving scarcity, it is equally important that the experts heed the advice of the public”[3]
Dr. Daughtery Biddison emphasizes the importance of transparency and systematization in triage. Without labeling and identifying triage, we fall into a sort of insidious triage, that is happening on the individual level, by the provider, and is adhoc.
Where we Stand Now
COVID-19 showed us that insidious triage is not just theoretical. In a study published in the Canadian Journal of Anesthesia, the authors point out how ICU demand during the pandemic strongly correlated with ICU mortality. For instance, a study published in Annals of Internal Medicine looked at 558 hospitals across the United States during COVID 19 and found that mortality increased for patients presenting during COVID-19 surges. In fact, they found that one in four deaths from COVID 19 were potentially attributable to surge caseloads.[1]
Another study, published in JAMA that looked at COVID deaths at VA hospitals in the United states found that the hazard ratio for death was 1.94 when COVID-19 ICU demand was between 75-100% in comparison with <25% demand. [2] Despite these numbers, only nine states in the US formally declared they were implementing triage protocols.
In Canada, no province or territory implemented triage protocols. But was triage still happening? Was it insidious triage? Was it the emergency room physicians, intensivists and internists that were making decisions? What factors were they considering? Were they playing God?
So where are we today? Where do our daily decisions fall on the spectrum? And how can we apply what we’ve learned to make our practice more systematic and less biased.
Probably somewhere in the middle of the spectrum — beyond the original purpose of CTAS, but not yet at full-blown crisis triage. In many ways, we are already practicing insidious triage. The question is whether we will continue to let it happen unacknowledged — or whether we will demand systematization and transparency.
Summary
- Recognize where you are on the triage spectrum. Pause if you feel you’re crossing into life-or-death decision-making.
- Systematize where possible. Use evidence-based tools for decisions like who needs monitors.
- Address bias. Reflect when caring for patients from marginalized groups.
- Speak up. If the ED is unsafe, alert administrators and document your concerns.
- Involve the public. True fairness in triage requires transparency and community engagement.
The stories of Brian Sinclair, Myron Cybriwski, and Emmett Everett remind us that triage is not just logistics — it is life and death. If we fail to systematize and evaluate it, we risk repeating the errors of the God Squad.
References
Benishek, Lauren E., et al. “Mitigating Health-Care Worker Distress from Scarce Medical Resource Allocation during a Public Health Crisis.” Chest, vol. 158, no. 6, Dec. 2020, pp. 2285–2287, https://doi.org/10.1016/j.chest.2020.07.073.
Biddison, Lee Daugherty, et al. “Perspective | U.S. Hospitals May Have to Ration Care during the Pandemic. Here’s One Approach.” Washington Post, www.washingtonpost.com/outlook/2020/03/12/us-hospitals-may-have-ration-care-during-pandemic-heres-one-approach/.
Bravata, Dawn M., et al. “Association of Intensive Care Unit Patient Load and Demand with Mortality Rates in US Department of Veterans Affairs Hospitals during the COVID-19 Pandemic.” JAMA Network Open, vol. 4, no. 1, 19 Jan. 2021, pp. e2034266–e2034266, jamanetwork.com/journals/jamanetworkopen/article-abstract/2775236, https://doi.org/10.1001/jamanetworkopen.2020.34266.
Bullard, Michael J., et al. “Revisions to the Canadian Emergency Department Triage and Acuity Scale (CTAS) Guidelines 2016.” CJEM, vol. 19, no. S2, July 2017, pp. S18–S27, https://doi.org/10.1017/cem.2017.365.
Calder, Lisa A., et al. “Mapping out the Emergency Department Disposition Decision for High-Acuity Patients.” Annals of Emergency Medicine, vol. 60, no. 5, Nov. 2012, pp. 567-576.e4, https://doi.org/10.1016/j.annemergmed.2012.04.013. Accessed 13 July 2020.
Chen, Esther H., and Judd E. Hollander. “When Do Patients Need Admission to a Telemetry Bed?” The Journal of Emergency Medicine, vol. 33, no. 1, July 2007, pp. 53–60, https://doi.org/10.1016/j.jemermed.2007.01.017.
Chen, Stephanie, and Sammy Zakaria. “Behind the Monitor—the Trouble with Telemetry.” JAMA Internal Medicine, vol. 175, no. 6, 1 June 2015, p. 894, https://doi.org/10.1001/jamainternmed.2015.0837. Accessed 29 Mar. 2020.
Daugherty Biddison, E. Lee, et al. “Too Many Patients…a Framework to Guide Statewide Allocation of Scarce Mechanical Ventilation during Disasters.” Chest, vol. 155, no. 4, Apr. 2019, pp. 848–854, https://doi.org/10.1016/j.chest.2018.09.025.
Fink, Sheri. “The Deadly Choices at Memorial.” The New York Times, 25 Aug. 2009, www.nytimes.com/2009/08/30/magazine/30doctors.html.
Gatien, Mathieu, et al. “A Clinical Decision Rule to Identify Which Chest Pain Patients Can Safely Be Removed from Cardiac Monitoring in the Emergency Department.” Annals of Emergency Medicine, vol. 50, no. 2, Aug. 2007, pp. 136–143, https://doi.org/10.1016/j.annemergmed.2007.02.004. Accessed 10 Oct. 2019.
Government of Canada. “Health.” Www.rcaanc-Cirnac.gc.ca, 23 Apr. 2018, www.rcaanc-cirnac.gc.ca/eng/1524499024614/1557512659251.
Grafstein, Eric, et al. “Revision of the Canadian Emergency Department Information System (CEDIS) Presenting Complaint List Version 1.1.” CJEM, vol. 10, no. 02, Mar. 2008, pp. 151–161, https://doi.org/10.1017/s1481803500009878.
Gunn, Brenda. “Ignored to Death: Systemic Racism in the Canadian Healthcare System” Submission to EMRIP the Study on Health. 2016.
Hinson, Jeremiah S., et al. “Triage Performance in Emergency Medicine: A Systematic Review.” Annals of Emergency Medicine, vol. 74, no. 1, July 2019, pp. 140–152, https://doi.org/10.1016/j.annemergmed.2018.09.022. Accessed 5 July 2020.
Iserson, Kenneth V., and John C. Moskop. “Triage in Medicine, Part I: Concept, History, and Types.” Annals of Emergency Medicine, vol. 49, no. 3, Mar. 2007, pp. 275–281, https://doi.org/10.1016/j.annemergmed.2006.05.019. Accessed 13 Oct. 2019.
Kadri, Sameer S., et al. “Association between Caseload Surge and COVID-19 Survival in 558 U.S. Hospitals, March to August 2020.” Annals of Internal Medicine, 6 July 2021, https://doi.org/10.7326/m21-1213.
Lett, Dan. “Emergency Department Problems Raised at Sinclair Inquest.” Canadian Medical Association Journal, vol. 185, no. 17, 21 Oct. 2013, pp. 1483–1483, www.cmaj.ca/content/cmaj/185/17/1483.full.pdf, https://doi.org/10.1503/cmaj.109-4633.
McLane, Patrick, et al. “First Nations Status and Emergency Department Triage Scores in Alberta: A Retrospective Cohort Study.” Canadian Medical Association Journal, vol. 194, no. 2, 16 Jan. 2022, pp. E37–E45, https://doi.org/10.1503/cmaj.210779.
“Memorial Medical Center and Hurricane Katrina.” Wikipedia, 1 Sept. 2021, en.wikipedia.org/wiki/Memorial_Medical_Center_and_Hurricane_Katrina.
Mitka, Mike. “Joint Commission Warns of Alarm Fatigue.” JAMA, vol. 309, no. 22, 12 June 2013, p. 2315, https://doi.org/10.1001/jama.2013.6032. Accessed 13 Feb. 2020.
“Montreal Woman Demands Change after 65-Year-Old Father Dies Waiting for Ambulance.” CBC, 29 July 2022, www.cbc.ca/news/canada/montreal/woman-montreal-man-dies-ambulance-1.6536857. Accessed 14 Oct. 2024.
Moynihan, Ray, et al. “Impact of COVID-19 Pandemic on Utilisation of Healthcare Services: A Systematic Review.” BMJ Open, vol. 11, no. 3, 1 Mar. 2021, p. e045343, bmjopen.bmj.com/content/11/3/e045343, https://doi.org/10.1136/bmjopen-2020-045343.
National Inquiry into Missing and Murdered Indigenous Women and Girls. “Home Page – Final Report | MMIWG.” Www.mmiwg-Ffada.ca, 29 May 2019, www.mmiwg-ffada.ca/.
Out of Sight. 2017.
Owens, Allison, et al. “Patient Race, Ethnicity, and Care in the Emergency Department: A Scoping Review.” CJEM, vol. 22, no. 2, 17 Feb. 2020, pp. 245–253, https://doi.org/10.1017/cem.2019.458.
Patel, Mehul D, et al. “Patient Sex, Racial and Ethnic Disparities in Emergency Department Triage: A Multi-Site Retrospective Study.” American Journal of Emergency Medicine, 1 Nov. 2023, https://doi.org/10.1016/j.ajem.2023.11.008. Accessed 18 Dec. 2023.
Perkins, Jack, et al. “Telemetry Bed Usage for Patients with Low-Risk Chest Pain: Review of the Literature for the Clinician.” The Journal of Emergency Medicine, vol. 46, no. 2, 1 Feb. 2014, pp. 273–277, https://doi.org/10.1016/j.jemermed.2013.08.098. Accessed 26 Feb. 2024.
Sandau, Kristin E., et al. “Update to Practice Standards for Electrocardiographic Monitoring in Hospital Settings: A Scientific Statement from the American Heart Association.” Circulation, vol. 136, no. 19, 7 Nov. 2017, www.ahajournals.org/doi/abs/10.1161/CIR.0000000000000527, https://doi.org/10.1161/cir.0000000000000527.
Schaffer, Amanda. “The Moral Dilemmas of Doctors during Disaster.” The New Yorker, 12 Sept. 2013, www.newyorker.com/tech/annals-of-technology/the-moral-dilemmas-of-doctors-during-disaster.
Segall, Noa, et al. “Patient Load Effects on Response Time to Critical Arrhythmias in Cardiac Telemetry.” Critical Care Medicine, vol. 43, no. 5, May 2015, pp. 1036–1042, https://doi.org/10.1097/ccm.0000000000000923.
Staff, News. “Montreal Man Dies Waiting Nearly 12 Hours for Ambulance | CityNews Montreal.” CityNews Montreal, 3 Aug. 2022, montreal.citynews.ca/2022/08/03/montreal-man-dies-waiting-12-hours-ambulance/. Accessed 14 Oct. 2024.
Standards for Continuous Cardiac Monitoring In-Hospital (Telemetry).
Syed, Shahbaz, et al. “Prospective Validation of a Clinical Decision Rule to Identify Patients Presenting to the Emergency Department with Chest Pain Who Can Safely Be Removed from Cardiac Monitoring.” Canadian Medical Association Journal, vol. 189, no. 4, 30 Jan. 2017, pp. E139–E145, https://doi.org/10.1503/cmaj.160742. Accessed 10 Oct. 2019.
Zachariasse, Joany M, et al. “Performance of Triage Systems in Emergency Care: A Systematic Review and Meta-Analysis.” BMJ Open, vol. 9, no. 5, May 2019, p. e026471, bmjopen.bmj.com/content/9/5/e026471, https://doi.org/10.1136/bmjopen-2018-026471. Accessed 6 Dec. 2019.
Thank you for this thoughtful exploration of triage decision-making. One notable omission, however, is the role of nurses. In most emergency departments, it is nurses who perform the vast majority of triage – assessing patients on arrival, assigning CTAS scores, managing patient flow, and re-triaging as conditions evolve.
Importantly, nurses also initiate medical directives at triage (blood work, ECGs, imaging, or medications), which provide physicians with critical data to more accurately determine who requires immediate attention. While the post references gestalt, it is worth noting that there is evidence supporting the value of clinical intuition, particularly when grounded in years of experience – something most triage nurses bring to their role (Melin-Johansson et al., 2017; Gorik et al., 2023).
Finally, triage today is predominantly conducted using electronic software. Any meaningful attempt to systematically reduce bias, therefore, must also involve consultation with IT and software design, not solely the individuals making bedside decisions.
Any discussion of triage feels incomplete without acknowledging the central, skilled, and experience-driven role that nurses play in the process.