
It’s no secret that in Canada, family medicine is in crisis. 6.5 million Canadians are without a family doctor,¹ and in a recent Ontario survey, 65% of family physicians reported preparing to leave their profession or reduce hours over the next five years.² This is reflected in the patients we see: increasing volume, complexity, and burden of unmanaged chronic disease. Patients are struggling, and we in the ED are often unable to meet their needs.
So — what should we do?
In its original form, an emergency room was designed to manage and stabilize acute illness and decompensated chronic disease. Preventive and primary care were meant to occur in — well — primary care settings. But this isn’t our current reality. Emergency medicine has become an all-encompassing healthcare safety net, expanding beyond its original mission of acute care. While the debate continues about whether we should innovate or reaffirm our core mission, one thing holds true: these patients are still coming. At least for the short term, regardless of where you fall on that spectrum, we as emergency specialists are not well-equipped to manage many chronic issues.
With that in mind, in the first post of this 2-part series, let’s explore how we can safely intervene on two common primary-care presentations in the ED: non-emergent hypertension and COPD. Part 2 will focuses on the ED management to depression (stay tuned)!
Non-Emergent Hypertension
Hypertension is incredibly common,³ is the single most modifiable risk factor for death and disability,⁴ and places a huge economic burden on our healthcare system.⁵ ED visits for hypertension are also on the rise.⁶ ⁷Despite seeing these patients frequently, EM providers continue to debate the role of treatment. Much of this stems from uncertainty around whether ED blood-pressure readings reflect “real” hypertension. That said, studies show that high BP often remains elevated post-discharge and is not materially influenced by pain or anxiety. Although evidence quality was low (no RCTs, small studies), a systematic review found that 50% of patients with elevated ED BP had uncontrolled hypertension afterward.⁸
Take-Home Point #1: Elevated blood pressure in the ED often represents true hypertension. Don’t underplay it, especially in patients with risk factors.
Step 1: Making the Diagnosis
When should we intervene?
The 2020 Hypertension Canada guidelines base diagnosis on both office and out-of-office measurements. From an ED perspective, focus on:
-
In-“office” (ED) criteria: Mean office BP ≥ 180/110 mmHg.
-
Re-measure if the patient presents for hypertension.
-
In a prospective study following patients with BP > 160/100 mmHg, the best discrimination between hypertensive and normotensive occurred 60–80 minutes after arrival.⁹
-
-
“Out-of-office” criteria: Review home BP logs when available. Diagnostic cut-offs are > 135/85 mmHg, or > 130/80 mmHg for diabetes.
For patients with borderline ED pressures and no home readings, educate them on proper measurement and provide a BP log (two readings AM + PM for ≥ 7 days).

From the 2020 Hypertension Canada Guidelines
Step 2: Deciding to Treat
Once the diagnosis is made, should we start treatment in the ED?
There are no formal guidelines for ED management of non-emergent hypertension, except the 2013 ACEP consensus statement suggesting treatment in select populations (e.g., poor follow-up).¹⁰ Is there a benefit in starting therapy from the ED? Maybe.
Potential benefits:
-
A multicentre cohort of 93 512 ED patients found that antihypertensive prescriptions at discharge reduced 30-day severe adverse events, though absolute event rates were < 1%.¹¹
-
Another cohort (~300 000 patients) linked in-ED elevated BP with later cardiovascular events, estimating NNT = 71 to prevent one event in 3 years for SBP > 140.¹²
-
Conversely, a 10 000-patient study showed no significant difference at 2 years but trended toward higher risk in those with BP > 160/110.¹³
Potential harms:
Data are limited. A retrospective analysis of 217 patients found no short-term adverse differences between those prescribed vs not prescribed antihypertensives.¹⁴
Take-Home Point #2: For patients with persistent BP > 180/110 mmHg or meeting outpatient diagnostic criteria without other causes, consider diagnosis and treatment.
Step 3: Initiating Management
Let’s review how to manage these patients, once you have decided to diagnose and treat it. And while the guidelines are quite extensive, we will it down to 2 main components:
1. Health Behaviour Change
Recommended for all patients.
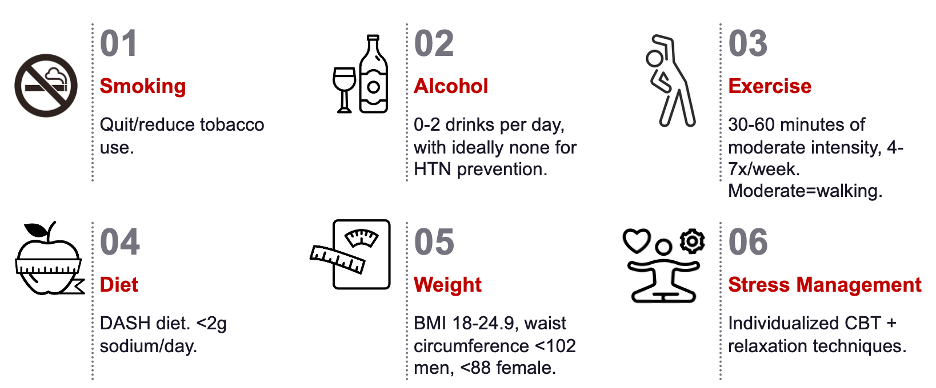
From the 2020 Hypertension Canada Guidelines
When it comes to deciding when behaviour change is enough, or deciding to start medication, it usually relies on a lot of discussion with patients, their numbers, comorbidities, and level of motivation. When we spoke to our local family medicine experts, they use the following approach:
- Always counsel on behaviour change.
- Consider behaviour change:
- Motivated patient
- 130-139/80-89 + low cardiovascular risk
- Consider pharmacological:
- Severe hypertension –180/110
BP >140/90, especially those with higher cardiovascular risk, diabetes or CKD
2. Pharmacological
From a medication standpoint, you have numerous first-line options for most patients, with some nuances based on their comorbidities and medical history.
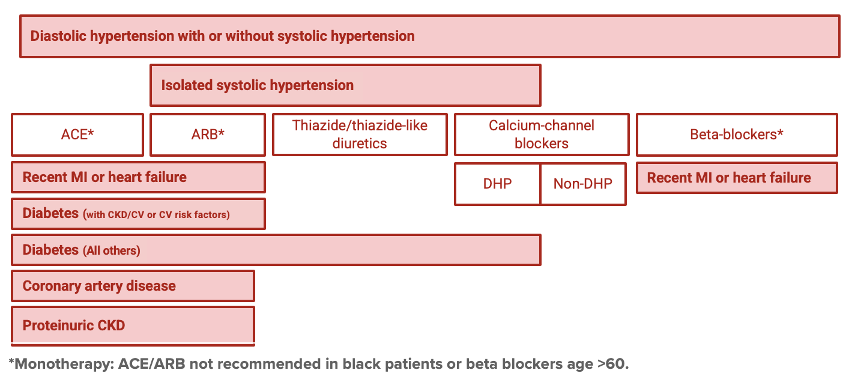
From the 2020 Hypertension Canada Guidelines
For the purposes of simplicity and a starting point for us in the emergency room, amlodipine and candesartan are 2 common first-line medications that you can consider:
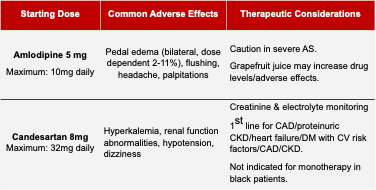
From the 2020 Hypertension Canada Guidelines
Summary: Hypertension
- In-ED hypertension is associated with “true” hypertension.
- Consider treatment if blood pressure is persistently >180/110, or other outpatient criteria is met.
- Health behaviour change for all.
- Amlodipine 5mg is a reasonable safe medication option for most patients.
- Follow-up is needed for medication adjustments, electrolyte & creatinine management (in the case of ACE/ARB)
- Educate patients on how to take their blood pressure and give them a logbook with resources.
For more information, there is a newly released primary-care focused 2025 Hypertension Canada guideline15 .
COPD
Let’s wrap up with COPD. It is another one of the most common chronic diseases in Canada, affecting 10% of Canadians, 1 in 5 over 70, and has an associated high morbidity and mortality28.
For a complete review of outpatient COPD exacerbations, check out Dr. Mungham’s 2019 blog post on this topic.
A large driver of this morbidity and mortality stems from the exacerbations themselves. We know that following an exacerbation of COPD, the rate of re-exacerbations increases, there is increased risk of cardiovascular events, there is associated loss of lung function, physical deconditioning, and all-cause mortality29,30. Therefore, an ED exacerbation itself represents a critical moment to intervene and reduce the risk of COPD-related mortality.
Until recently, only non-pharmaceutical interventions of smoking cessation and home oxygen showed a mortality benefit for these patients. However, in 2023, newly released Canadian Thoracic Society COPD guidelines had some important changes relevant for the ED provider with mortality benefit.’
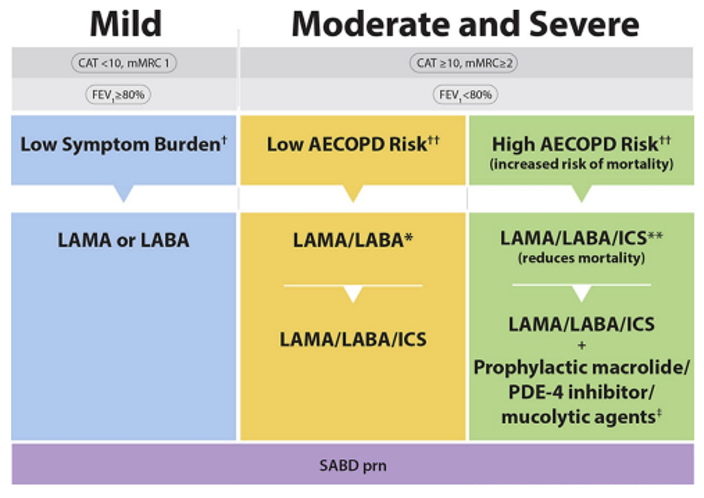
From the Canadian Thoracic Society COPD Guidelines
- All symptomatic patients with COPD should now be on at least a monotherapy. For diagnosed COPD patients with some element of symptom burden, there is now a recommendation for at minimum a monotherapy, with preference for LAMA over LABA (e.g. Tiotropium Spiriva).
- And the second, and most significant for us, is that for any individual we see in the ED with an exacerbation, there is a now an indication for escalation to triple inhaler ICS/LABA/LAMA. It is also recommended for patients who have 2 “moderate exacerbations” – in which they had requires antibiotics and or systemic steroids but did not come to the ED or hospitalized.
In these patients, once escalated, in general, the recommendation is to remain on triple inhaler therapy given the risks of removal of ICS in worsening lung function.
Finally, although not in the guidelines, a specific recommendation we know from prior research that timing matters. Delays in initiation of maintenance therapy beyond 30 days following exacerbations found an increased risk of exacerbation and subsequent link to worse outcomes31, so we as ED providers can play a huge role in the care of these patients.
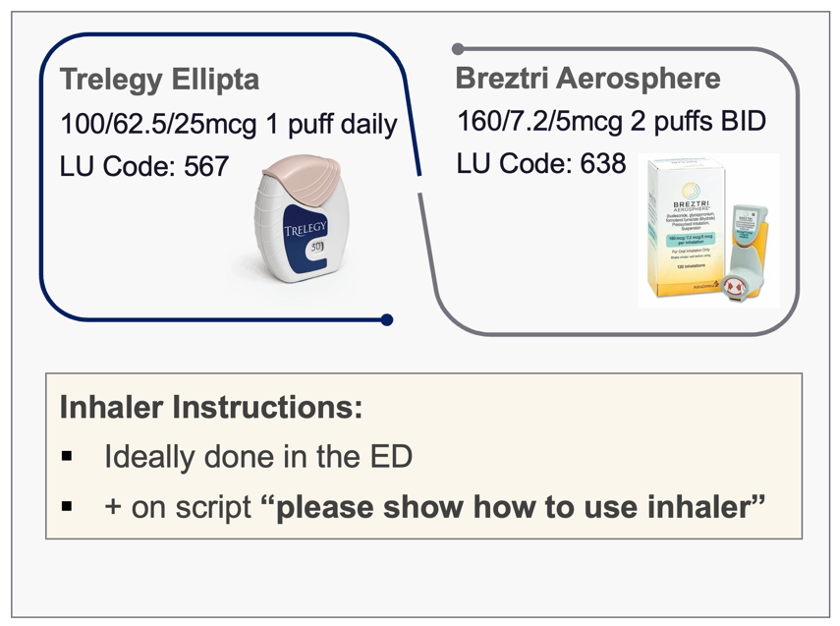
Triple Inhaler Therapy
There are currently 2 triple inhaler therapy options – Trelegy Ellipta, a dry powder inhaler (1 puff daily) and Breztri, a soft mist meter dose inhaler (2 puffs BID). Top tips from our local experts include making sure patients know how to use the inhaler, especially if switching between device classes, and to write on your prescriptions to ask the pharmacist to review inhaler technique when being discharged.
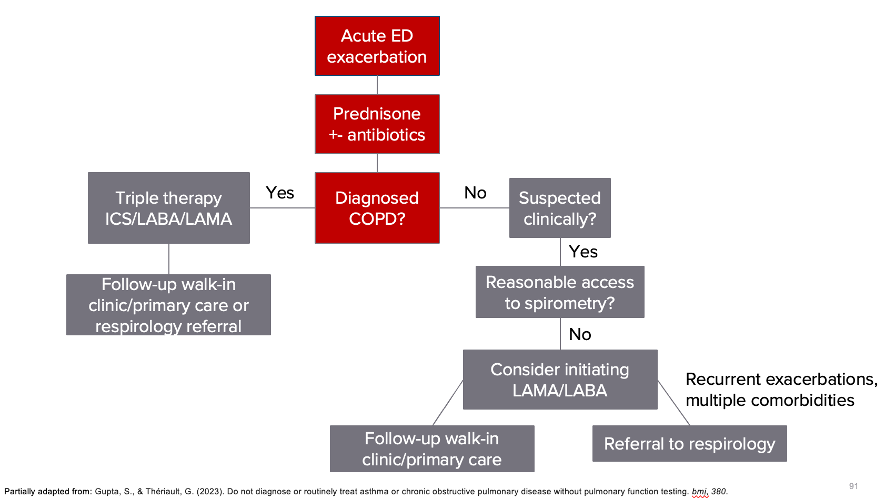
What about patients without a formal diagnosis?
These recommendations are quite streamlined for patients with a pre-existing COPD diagnosis. But we are not working in a perfect world. And I’m sure you have all seen that patient who has risk factors for COPD, you suspect they have COPD clinically, and they come in with a suspected exacerbation. Only they are good enough to go home. Do we offer triple therapy in these cases?
The dilemma: COPD is simultaneously underdiagnosed and overdiagnosed.
This is a common situation we see not only in COPD but also in other respiratory diseases in Canada. Spirometry is required for diagnosis, yet in reality, it is difficult to obtain, driven by (a) lack of primary care and (b) long wait times.
We have data to suggest that COPD is underdiagnosed and undertreated in certain patients, with population-based studies showing that approximately 30–60% of patients with a physician diagnosis do not actually have the disease.³²
So, what we are left with is a strong body of evidence that tells us starting therapy on COPD patients presenting to us in the ED is life-altering, yet must be balanced against the risks of treating and escalating unnecessarily.
In speaking with our practice experts, they too have adapted a revised approach for these tricky clinical scenarios, recognizing the barriers to accessing timely spirometry in an era of resource scarcity. In our local centre, one of our experts highlighted their approach to these patients when they see them as inpatients:
“Even though they may meet ‘guideline criteria’ for triple therapy, we will often start them on LABA/LAMA instead. We ask ourselves — are they just so severe because they are untreated?
The same approach can be applied to the ED. For those with a strong suspicion of a new diagnosis of COPD with an exacerbation, you can consider starting a LAMA/LABA with recommendations for follow-up for spirometry, referral to respirology if recurrent exacerbations or comorbidities.
I would be hesitant to start triple therapy up front [without spirometry], given the theoretical risk of pneumonia and the fact that de-escalation is not recommended.”
So, taken together, this brings us to my personal “real-world” summary:
What becomes critical for you is to counsel these patients on the importance of follow-up (in the ED, with a primary care provider, respirologist) as these patients still need confirmatory spirometry.
For LABA/LAMA combinations, there are many options to choose from, but our local expert recommended their go-to puffers of either Inspiloto Respimat or Anora Ellipta:

Summary: COPD
- A single ED exacerbation is an indication for triple therapy inhaler with mortality benefit (Trelegy Ellipta or Breztri Aerosphere)
- All patients with COPD are recommended to be on maintenance therapy, with LAMA > LABA preference.
- Consider initiating LAMA/LABA in undiagnosed, yet high clinical suspicion COPD patients presenting with an exacerbation. Consider: Inspiolto Respimat or Anoro Ellipta.
- All patients need spirometry confirmation. The timing of which will depend on your local referral pathways.
What about Follow Up?
We’ve just reviewed some practical, ED-focused management tips for primary care conditions. But the issue remains that a lot of these treatments we are considering starting, or escalating provide benefit, and still require some kind of follow-up. And for many of our patients, our current state system is not set-up in a way to support them.
The also real concern that many of us are faced with and are thinking about, is the medicolegal risk in the event the patient is lost to follow-up after starting therapies from the ER. We are trying to act in the best interests of the patient, but we know that in general, the ED is not the place for longitudinal chronic disease management. So how do we navigate this?
I spoke with a local CMPA practice expert who put it simply:
“You are doing what you can with the best of your abilities, in the circumstances and resources you are working within, and in the best interests of the patient….”
And in these circumstances, recommended the following:
- Explain your thought process
- Document a shared decision-making (risks of not prescribing vs. prescribing with no confirmed follow-up), including information about the current healthcare context (such as the lack of primary care)
And where can patients go for this follow-up?
This will depend on where you practice and follow-up availability in your area. In our local region of Ottawa, approximately 1 in 10 patients are unattached to primary care providers33. Through this process of creating this talk and post, I developed a comprehensive Ottawa-specific guide to help patients access care in our region which you can access here.
And finally, I encourage you to reflect on the ways you can improve the care for these patients in your region, both on an individual care level and a systems level. It is incredibly challenging to navigate our current healthcare climate, and patients are struggling to get the care they deserve.
References
- Duong D, Vogel National survey highlights worsening primary care access. CMAJ. 2023 Apr 24;195(16):E592–E593. Available from: https://www.cmaj.ca/content/195/16/E592
- Ontario College of Family Physicians. New survey shows full‑blown crisis in family medicine [Internet]. May 30, 2023 [cited 2025 Jan 24]. Available from: https://ontariofamilyphysicians.ca/news/new-survey-shows-full-blown-crisis-in-family-medicine/
- Statistics Canada. (2019). Primary health care providers, 2017. Health Reports, 30(2), 3–11. Retrieved January 24, 2025, from https://www150.statcan.gc.ca/n1/pub/82-003-x/2019002/article/00001-eng.htm
- Tobe, S., Harvey, P., Mabaya, G., & Summers, D. (2024). A NEW QUALITY STANDARD FOR HYPERTENSION: GUIDING EVIDENCE-BASED, HIGH-QUALITY CARE IN ONTARIO. Canadian Journal of Cardiology, 40(10), S132.
- Weaver CG, Clement F, Campbell N et al. Health Care Costs Attributable to Hypertension: a Canadian Population-Based Cohort Study. Hypertension. 2015;66:00-00. DOI: 10.1161/HYPERTENSIONAHA.115.05702.
- Masood S, Austin PC, Atzema CL. A population-based analysis of outcomes in patients with a primary diagnosis of hypertension in the emergency department. Annals of emergency medicine. 2016 Sep 1;68(3):258-67.
- Hypertension Canada. (2024). Hypertension: Introducing a new standard for high-quality care in Ontario. Retrieved January 24, 2025, from https://hypertension.ca/news/hypertension-introducing-a-new-standard-for-high-quality-care-in-ontario/#:~:text=Patient%20outcomes%20for%20hypertension%20can,home%20and%20community%20care%20settings
- Michaud, A., Lamarre-Cliche, M., Vadeboncoeur, A., & Cloutier, L. (2020). Screening for hypertension in adults during emergency department consultation: a systematic review. European Journal of Emergency Medicine, 27(3), 178-185
- Dieterle, T., Schuurmans, M. M., Strobel, W., Battegay, E. J., & Martina, B. (2005). Moderate-to-severe blood pressure elevation at ED entry: hypertension or normotension?. The American journal of emergency medicine, 23(4), 474-479.
- Wolf, S. J., Lo, B., Shih, R. D., Smith, M. D., & Fesmire, F. M. (2013). Clinical policy: critical issues in the evaluation and management of adult patients in the emergency department with asymptomatic elevated blood pressure. Annals of emergency medicine, 62(1), 59-68.
- Todd, B. R., Xing, Y., Zhao, L., Nguyen, A., Swor, R., Eberhardt, L., & Bahl, A. (2024). Antihypertensive prescription is associated with improved 30‐day outcomes for discharged hypertensive emergency department patients. Journal of the American College of Emergency Physicians Open, 5(2), e13138.
- Oras, P., Häbel, H., Skoglund, P. H., & Svensson, P. (2020). Elevated blood pressure in the emergency department: a risk factor for incident cardiovascular disease. Hypertension, 75(1), 229-236.
- McAlister, F. A., Youngson, E., & Rowe, B. H. (2021). Elevated blood pressures are common in the emergency department but are they important? A retrospective cohort study of 30,278 adults. Annals of Emergency Medicine, 77(4), 425-432.
- Brody, A., Rahman, T., Reed, B., Millis, S., Ference, B., Flack, J. M., & Levy, P. D. (2015). Safety and efficacy of antihypertensive prescription at emergency department discharge. Academic Emergency Medicine, 22(5), 632-635.
- Goupil, R., Tsuyuki, R. T., Santesso, N., Terenzi, K. A., Habert, J., Cheng, G., … & Hundemer, G. L. (2025). Hypertension Canada guideline for the diagnosis and treatment of hypertension in adults in primary care. CMAJ, 197(20), E549-E564.
- Ontario Health. (2021). Summary report. https://www.ontariohealth.ca/sites/ontariohealth/files/2021-02/Summary.pdf
- 1 in 3 unmet care needs – Statistics Canada. (2023). Who are the gig workers in Canada? Retrieved January 24, 2025, from https://www150.statcan.gc.ca/n1/pub/11-627-m/11-627-m2023053-eng.htm
- Lam, RW, Kennedy, SH, Adams, C., Bahji, A., Beaulieu, S., Bhat, V., … & Milev, RV (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults. The Canadian Journal of Psychiatry , 07067437241245384.
- Heissel, A., Heinen, D., Brokmeier, L. L., Skarabis, N., Kangas, M., Vancampfort, D., … & Schuch, F. (2023). Exercise as medicine for depressive symptoms? A systematic review and meta-analysis with meta-regression. British journal of sports medicine, 57(16), 1049-1057.
- Fabiano, N., Gupta, A., Fiedorowicz, J. G., Firth, J., Stubbs, B., Vancampfort, D., … & Solmi, M. (2023). The effect of exercise on suicidal ideation and behaviors: A systematic review and meta-analysis of randomized controlled trials. Journal of affective disorders, 330, 355-366.
- Noetel, M., Sanders, T., Gallardo-Gómez, D., Taylor, P., del Pozo Cruz, B., Van Den Hoek, D., … & Lonsdale, C. (2024). Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. bmj, 384.
- Zhou, C., Puder, D., & Fabiano, N. (2024). How to prescribe physical activity for depression. Sports Psychiatry: Journal of Sports and Exercise Psychiatry.
- Hammad, T. A., Laughren, T., & Racoosin, J. (2006). Suicidality in pediatric patients treated with antidepressant drugs. Archives of general psychiatry, 63(3), 332-339.
- Stone, M., Laughren, T., Jones, M. L., Levenson, M., Holland, P. C., Hughes, A. ….. & Rochester, G. (2009). Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration. Bmj, 339.
- Friedman, R. A. (2014). Antidepressants’ black-box warning—10 years later. New England Journal of Medicine, 371(18), 1666-1668.
- Centre for Clinical Interventions. Looking After Yourself: Self‑help resources for mental health problems [Internet]. Perth (Australia): CCI; 2024 Jan 16 [cited 2025 Jun 24]. Available from: https://www.cci.health.wa.gov.au/resources/looking-after-yourself
- Lam, RW, Kennedy, SH, Adams, C., Bahji, A., Beaulieu, S., Bhat, V., … & Milev, RV (2024). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2023 Update on Clinical Guidelines for Management of Major Depressive Disorder in Adults. The Canadian Journal of Psychiatry , 07067437241245384.
- Blazer, A. J., & Stanbrook, M. B. (2023). How can Canada’s health systems improve care for people with chronic obstructive pulmonary disease?. CMAJ, 195(35), E1182-E1183.
- Bourbeau, J., Bhutani, M., Hernandez, P., Aaron, S. D., Beauchesne, M. F., Kermelly, S. B., … & Marciniuk, D. D. (2023). 2023 Canadian Thoracic Society guideline on pharmacotherapy in patients with stable COPD. Chest.
- Papaioannou AI, Hillas G, Loukides S, Vassilakopoulos T. Mortality prevention as the centre of COPD management. ERJ Open Res. 2024 Jun 17;10(3):00850-2023. doi: 10.1183/23120541.00850-2023. PMID: 38887682; PMCID: PMC11181087.
- Coutinho, A. D., Lokhandwala, T., Boggs, R. L., Dalal, A. A., Landsman-Blumberg, P. B., Priest, J., & Stempel, D. A. (2016). Prompt initiation of maintenance treatment following a COPD exacerbation: outcomes in a large insured population. International Journal of Chronic Obstructive Pulmonary Disease, 1223-1231.
- Diab, N., Gershon, A. S., Sin, D. D., Tan, W. C., Bourbeau, J., Boulet, L. P., & Aaron, S. D. (2018). Underdiagnosis and overdiagnosis of chronic obstructive pulmonary disease. American journal of respiratory and critical care medicine, 198(9), 1130-1139.
- University of Ottawa. (n.d.). Confronting the crisis: DFMS comprehensive strategy lays out a path to primary care for all. Retrieved January 24, 2025, from https://www.uottawa.ca/en/news-all/confronting-crisis-dfms-comprehensive-strategy-lays-out-path-primary-care-all
Thank you for your efforts and for taking the time. That was a nice topic and very common to see both in the ED and the Urgent care setting.
I referred to your topic later, and it was very useful! Please continue doing the great work. Primcare In the ED! Awesome: Title and topics!. Thanks