Rib fractures are a common traumatic injury seen in the ED, and are diagnosed in over 30% blunt trauma patients (Liman et al., 2003).
The traditional approach to rib fracture analgesia in the ED relies heavily on systemic medications, like opioids. While this strategy is familiar and easy to deploy, it is frequently insufficient. Opioids provide inconsistent analgesia for movement-related chest wall pain, do little to improve inspiratory effort, and are limited by dose-dependent adverse effects including sedation, delirium, nausea, and respiratory depression, particularly in older or frail patients.
PoCUS-guided regional anesthesia offers a powerful tool to standard systemic therapy. When used early as an adjunct, regional anesthesia in the ED can meaningfully reduce opioid requirements, improve respiratory mechanics, and change the trajectory of rib fracture patients in a way that systemic analgesia alone often cannot (Ho et al., 2019).
This month’s PoCUS Pearl focuses on two ultrasound-guided regional techniques that are safe, ED-appropriate, and highly effective:
- The Serratus Anterior Plane (SAP) Block
- The Erector Spinae Plane (ESP) Block
Both are fascial plane blocks and well within your scope as an emergency physician. Let’s break down these tools you can use to dramatically alter the trajectory of your next rib fracture patient!
Why Bother?
- Each additional rib fracture increases mortality by ~19% in older adults (Bulger, 2000).
- Inadequate analgesia is a major driver of:
- Hypoventilation
- Atelectasis
- Pneumonia
- ICU admission
- Thoracic epidurals and paravertebral blocks work—but are not feasible in the ED.
PoCUS-guided fascial plane blocks offer:
- Rapid analgesia
- Opioid sparing
- Minimal hemodynamic impact
- Low complication rates
- No need to visualize or contact nerves directly
Block #1: Serratus Anterior Plane (SAP) Block
This block is a lateral chest wall fascial plane block that deposits local anesthetic (LA) superficial or deep to the serratus anterior muscle, anesthetizing the lateral cutaneous branches of the thoracic intercostal nerves.
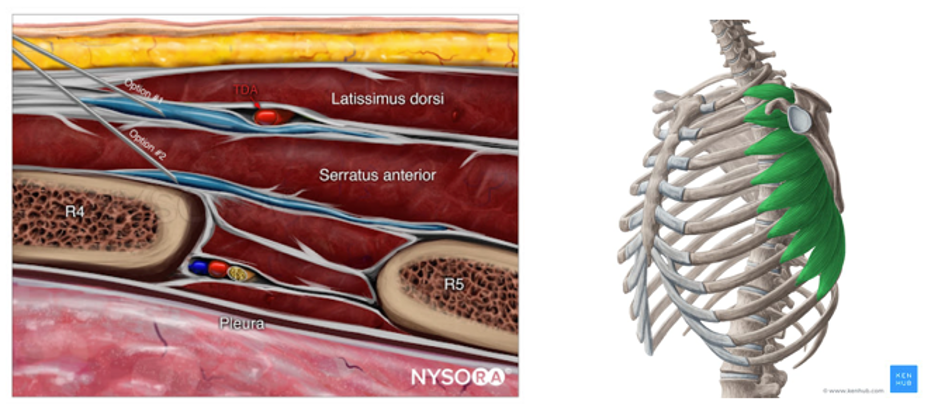
Image source: https://www.nysora.com/topics/regional-anesthesia-for-specific-surgical-procedures/thorax/pectoralis-serratus-plane-blocks/
ED Indications:
- Anterolateral rib fractures (approximately T2–T9)
- Patients who cannot sit forward or tolerate prone positioning
What Does it Block?
- Lateral cutaneous branches of the intercostal nerves between T2-T9
- Sensory analgesia to Anterolateral chest wall

Image source from Core Ultrasound: https://coreultrasound.com/serratus/
Levels of Anesthesia
- Typically covers 2–6 rib levels
- Dermatomal spread depends on volume and plane chosen
Equipment
- High-frequency linear probe
- Nerve block or echogenic needle (or 20–22G spinal needle)
- 20–40 mL local anesthetic (e.g., ropivacaine 0.5% or bupivacaine 0.25%)
- Sterile probe cover, gel, gloves
- Extension tubing and syringe
- Skin prep (chlorhexidine)
Patient Positioning
- Supine or slight lateral decubitus
- Ipsilateral arm abducted if tolerated
Ultrasound Landmarking
- Place the probe in the mid-axillary line, transverse orientation at the level of the 4th and 5th ribs.
- Identify (superficial → deep):
- Subcutaneous tissue
- Latissimus dorsi
- Serratus anterior muscle
- Ribs and pleural line (deep)
- Your target plane:
- Between latissimus dorsi and serratus anterior (superficial SAP)
- OR between serratus anterior and rib/pleura (deep SAP)
- Deep SAP may offer broader spread but is closer to pleura and comes with increased risk of pneumothorax.
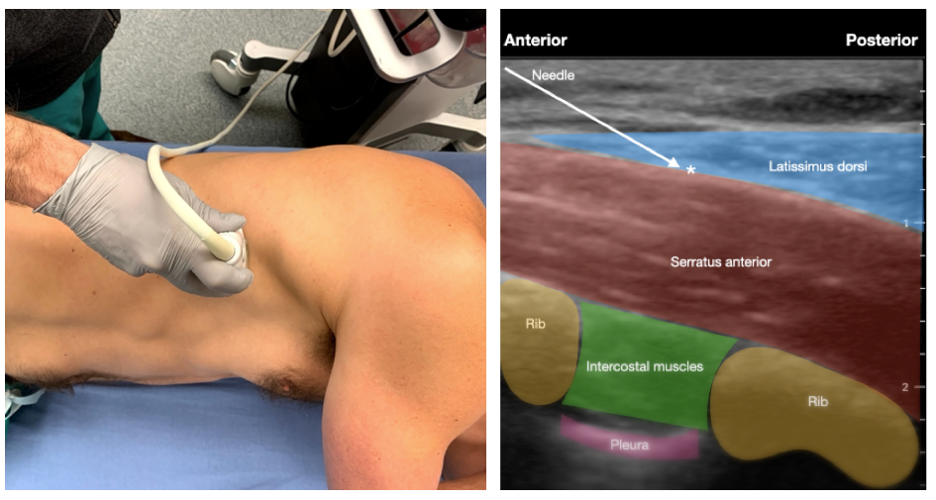
Image source: https://emdaily.cooperhealth.org/2024/10/16/rib-fractures-part-2-serratus-anterior-nerve-block-by-dr-demarzo/
How to Perform the Block
- In-plane needle approach, anterior to posterior
- Advance needle into the chosen fascial plane (i.e., superficial or deep SAP)
- Inject a small test aliquot
- Confirm linear hydrodissection
- Inject remaining volume slowly
- Continuously visualize needle tip
Note: although this block can be performed by injecting LA either superficial or deep to the serratus anterior muscle, we encourage a superficial injection to reduce the risk of pneumothorax
Pearls and Pitfalls
- Always keep the pleural line in view
- If LA spreads within muscle → you’re too superficial
- Use color Doppler to avoid thoracic vessels
- Aim trajectory of needle towards rib. This helps prevent possible pleural puncture in event of patient coughing or moving unexpectedly.
Block #2: Erector Spinae Plane (ESP) Block
A posterior thoracic fascial plane block where local anesthetic is injected deep to the erector spinae muscle but superficial to the transverse process (TP), allowing spread to dorsal and ventral rami.
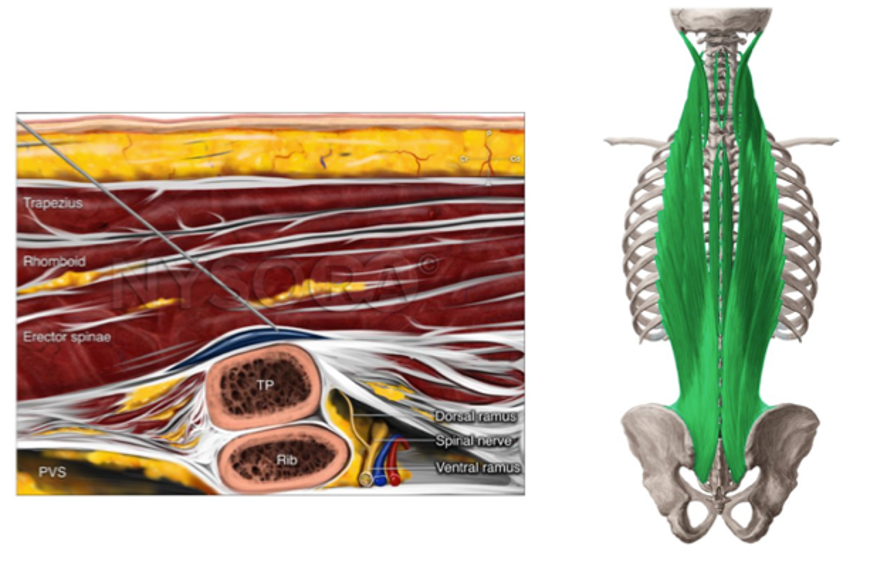
Image Source: NYSORA
https://www.nysora.com/education-news/comparing-programmed-intermittent-bolus-and-continuous-infusion-for-erector-spinae-plane-block-in-thoracic-surgery/
ED Indications
- Posterior or posterolateral rib fractures
What Does it Block?
- Dorsal and ventral rami of thoracic spinal nerves
- LA spreads cranio-caudally over several spinal levels and variably extends anteriorly toward the paravertebral space and laterally to involve the intercostal nerves, typically covering three to four levels above and below the injection site.
- Provides posterior + lateral ± anterior chest wall analgesia
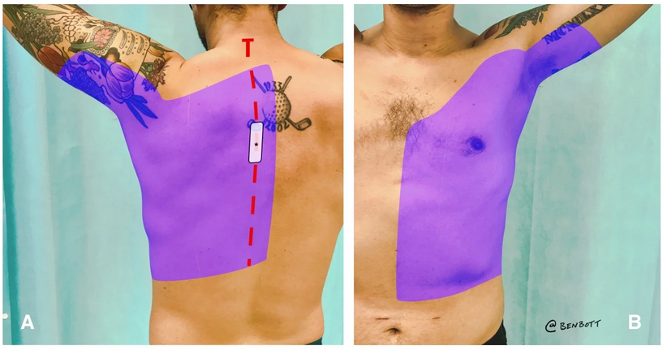
Image source:
https://www.sciencedirect.com/science/article/abs/pii/S0735675717310628
Level of Anesthesia
- Typically covers 3–5 vertebral levels above and below injection site
Equipment
- Same setup as SAP block – see above
Patient Positioning
- Sitting, lateral decubitus, or prone
- Sitting is often easiest in the ED
Ultrasound Landmarking
- Start with your probe on the posterolateral chest wall then slide medially. You should see the rounded off appearance of the rib (image C, below), laterally, transition into the TP that “lifts” into view as you move the probe medially (image B, below). If too medial with your probe, you will see the concave stepdown appearance of the lamina (image A, below).
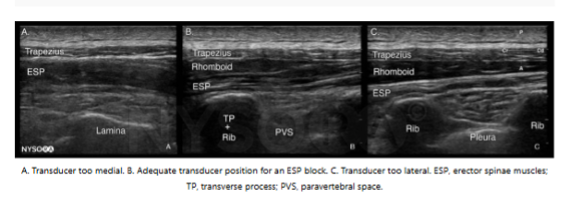
Image source: NYSORA
- Identify (superficial → deep):
- Skin/subcutaneous tissue
- Trapezius
- Rhomboid major (upper thoracic)
- Erector spinae muscle (ESM)
- Transverse process (square, hyperechoic with acoustic shadow)
- Your target:
- Fascial plane between erector spinae muscle and transverse process (figure b, below)
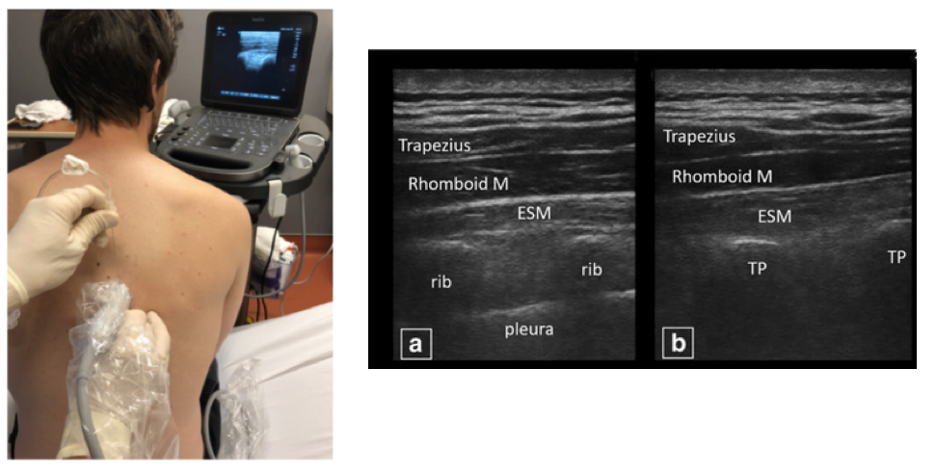
Image source: NYSORA
How to Perform the Block
- In-plane, cranial-to-caudal or caudal-to-cranial
- Advance needle until contacting transverse process (you will feel hard end-point from the transverse process)
- Withdraw slightly
- Inject test dose
- Look for lifting of erector spinae muscle off the transverse process
- Inject remaining volume slowly
Pearls and Pitfalls
- Scan laterally to medially to identify surrounding structures (ie. Spinous process, transverse process, ribs) and give yourself a better appreciation of the appearance of the transverse process vs the ribs
- The transverse process provides a hard end-point for your needle and increases the safety of this block
- If you see pleura → you’re too lateral
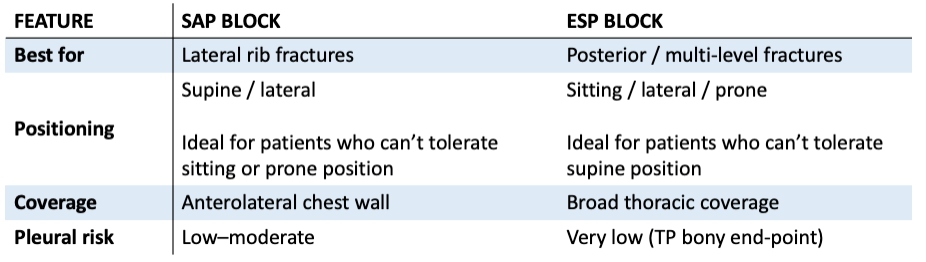
SAP vs ESP: What Should I Use?
Complications and Safety
- Local anesthetic systemic toxicity (LAST)
- Infection (rare)
- Hematoma (anticoagulation is not an absolute contraindication)
- Pneumothorax (rare; minimized with continuous visualization)
Take Home Points
- Rib fracture pain is dangerous when undertreated
- SAP and ESP blocks are:
- ED-appropriate
- Ultrasound-guided
- High-impact
- SAP = anterolateral chest wall coverage
- ESP = broader, posterior-predominant coverage
- Choose block based on your comfort level with each, location of fractures, and most comfortable patient position.
References
- Bulger, E. M., Arneson, M. A., Mock, C. N., & Jurkovich, G. J. (2000). Rib fractures in the elderly. The Journal of Trauma, 48(6), 1040–1047. https://doi.org/10.1097/00005373-200006000-00007
- Core Ultrasound. (n.d.). Serratus anterior plane block. https://coreultrasound.com/serratus/
- Ho, A. M.-H., Ho, A. K., Mizubuti, G. B., Klar, G., & Karmakar, M. K. (2019). Regional analgesia for patients with traumatic rib fractures: A narrative review. Journal of Trauma and Acute Care Surgery, 88(1), e22–e30. https://doi.org/10.1097/TA.0000000000002524
- Life in the Fast Lane. (n.d.). Serratus anterior plane block. https://litfl.com/serratus-anterior-plane-block/
- Liman, S. T., Kuzucu, A., Tastepe, A. I., Ulasan, G. N., & Topcu, S. (2003). Chest injury due to blunt trauma. European Journal of Cardio-Thoracic Surgery, 23(3), 374–378. https://doi.org/10.1016/S1010-7940(02)00813-8
- (n.d.). Pectoralis and serratus plane blocks. https://www.nysora.com/topics/regional-anesthesia-for-specific-surgical-procedures/thorax/pectoralis-serratus-plane-blocks/
- The PoCUS Atlas. (n.d.). Thoracoabdominal blocks. https://www.thepocusatlas.com/thoracoabdominal-blocks