
“Medicine is not only a science, it is also an art. It does not consist of compounding pills and plasters, it deals with the very processes of life, which must be understood before they may be guided.”– Paracelsus
We often hear about the art of medicine throughout our training. It refers to the humanistic and sometimes intangible aspects of caring for others. For some though, the art of medicine extends beyond a holistic clinical approach.
“The art of medicine consists of amusing the patient while nature cures the disease.” – Voltaire
The view of medicine as a form of performance is gaining in popularity. We can all agree that who we are with our patients will differ from who we are with our friends and loved ones. The question is – who are we in front of our patients and when are we acting? In a survey of my colleagues, many felt that their clinical practice incorporated elements of performance for a variety of reasons.
With many of us using performance as part of our practice, I believe that viewing these performances as a skill can fundamentally change our practice of medicine for the better. The evidence would support this statement; including concepts of performance art in medical education makes more empathetic, more adaptable, and more resilient doctors. (Case & Brauner, 2010; Gao et al., 2019; Smith et al., 2021)
If medicine contains performance, we must train it as an important skill of our profession. We must also recognize that performance is not faking but rather a choice to display a purposeful behaviour grounded in real emotional experience.
By purposefully incorporating lessons from performance art, we can enhance medical education, patient care, and physician wellbeing.
The structure for this summary is as follows:
- Act 1- discuss the elements of emergency medicine that create a space for the application of concepts from theatre.
- Act 2- discuss the role of the physician through a performance lens and use theatrical techniques to improve the delivery of this role.
- Act 3- review the importance of de-roling and discuss techniques for resiliency as utilized in theatre.
This summary will have input from the following guests:
Dr. Aaron Penciner- neurology resident physician and theatre actor. Dr. Mel Herbert – ER physician, and a medical consultant for the show The Pitt. Professor Hartley Jafine – professor at McMaster University who specializes in applied theatre, and an internationally recognized medical improv specialist.
Like every good theatre production, emergency medicine relies on an all-star cast of healthcare professionals working toward a shared goal of patient care. This cast includes physicians, nurses, respiratory therapists, social workers, porters, and many others, each with a distinct and essential role.
Once you have a cast, every performer needs a script. In emergency medicine, we use scripts often. This includes breaking bad news with the SPIKES protocol, handing over patients using SBAR, and delivering concise one-liners when consulting colleagues.
Choreography is another vital element. Emergency medicine requires the coordination of complex tasks that rely on both muscle memory and situational awareness, from rare procedures like Blakemore tube insertions to everyday practices such as point-of-care ultrasound.
Costuming also plays an important role. Scrubs and the Patagonia sweater are classic costuming choices for the emergency physician.
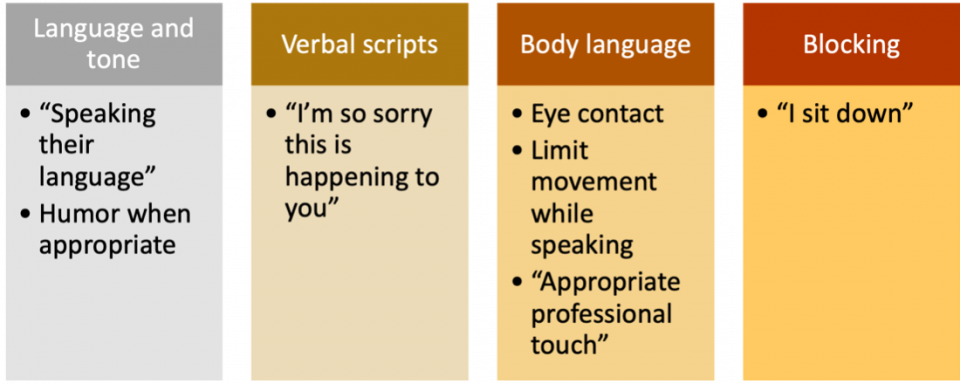
Blocking, or the intentional use of space, shapes how we communicate. Standing at the foot of the bed during a resuscitation or sitting beside a patient to discuss test results can influence both understanding and connection.
Every production needs a stage. Here, patients are the audience, the front stage includes patient-facing spaces, and the backstage includes areas like break rooms where team members step out of role.
Finally, no performance comes together without rehearsal. Medical education provides opportunities to practice through OSCEs, simulation, and clinical feedback.
When viewing doctors as performers, I thought it might be helpful to gain perspective from the other side of the coin, performers who play doctors. I met with Dr. Mel Herbert, an emergency physician and one of the medical consultants for the hit show The Pitt and previously ER. He possesses a unique perspective on the performance of medicine as someone who trains professional actors on how to portray it.
There are many reasons why physicians perform but the majority focus on building rapport, addressing patient expectations, and the desire to portray oneself as a “good doctor”.
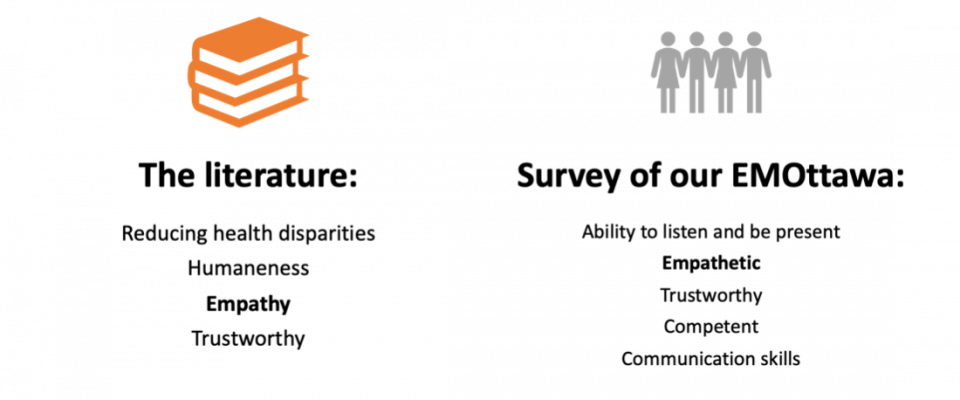
There is extensive research on the patient, public, and physician perceptions of qualities of good physicians (Dopelt et al, 2022).
When the patient expectations of a “good doctor” are not met, physicians are faced with complaints, with the top three areas of complaints being care and treatment, communication, and attitude (based on a regional survey of patients in Ottawa). Care and treatment often relates to physician competence, resource limitations, and patient discrimination. While this is an extremely important topic- we will focus on the communication and attitude issues as these are more modifiable on a personal level using theatrical techniques.
When patients complain about a physician’s attitude, they primarily refer to the physician’s ability to express empathy.
Empathy
Empathy is a key skill in the patient-physician relationship, which leads to better rapport, improved treatment plan compliance, and overall better patient outcomes. Research points towards empathy as a teachable skill that can be improved upon, often using techniques from theatre (Neufeld & Malin, 2024).
We can use elements from theatre including tone, scripts, body language, and blocking to portray higher empathy towards our patients.
Howe et al. 2019, Bendapudi et al. 2006
Communication
In addition to empathy, communication skills were also regarded as an important part of being a good physician. Once again, we can employ techniques from performance art to further grow this skill.
Communication is not a one size fits all approach and adaptability is key.
“Sometimes you have a patient and they’re making jokes about this incredibly unfortunate crisis and you need to make jokes back to them. Sometimes they are having a really hard time and you just need to echo that and be candid with them. Being able to recognize all types of emotions and language and mirror them is a really good tool for building rapport.”
– Dr. Aaron Penciner
“You have to look them in the eye. You have to speak clearly. You need to get out into the world to have a broad experience and bring that to work. You need to understand how old people talk, how kids talk, how teenagers talk. It’s about being a good actor. It’s about understanding patients and reflecting back to them.”
– Dr. Mel Herbert
Both Dr. Penciner and Dr. Herbert refer to the concept of mirroring, which is a key skill in improvisation theatre that is deeply transferrable to medicine.
Medical Improv
I spoke with Prof. Hartley Jafine about the direct applications of improv to emergency medicine.
Professor Jafine also highlighted to me the importance of informal improv such as meeting with peers to practice how we can respond to different patient scenarios and receiving feedback on our performance. For more information on the use of medical improv – please see the video here.
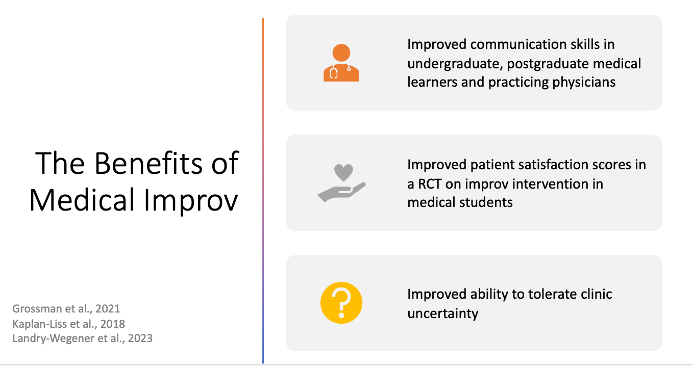
With its benefits towards improving communication skills and ability to manage uncertainty, medical improv is a powerful tool that we should consider implementing within formal medical education.
Professional Identity Formation
In addition to the benefits to patient care, the performance art of medicine can also benefit physicians in their professional identity formation. Professional identity formation is a process whereby the characteristics, values and norms of the medical profession are internalized, resulting in an individual thinking, acting, and feeling like a physician (Cruess et al., 2019).
In theatre, actors use character work to inhabit a role. They study and form the character’s identity which can include their backstory, motivations, values, and objectives until they can be that person while on stage. Medicine is similar: through professional identity formation, over time we shift from ‘acting like’ a physician to being one.
If being a physician is a role, then professional identity formation is a form of character work.
There are many benefits to the process of professional identity formation, or what we might think of as medical character work. First, it can foster a sense of belonging within the profession of medicine. It has also been shown to improve job satisfaction and fulfillment across different stages of practice (Sarraf-Yadzi et al., 2024).
This process also provides a framework for future career decisions. It helps answer questions such as: What kind of environment do I want to work in? What academic or research interests do I want to pursue? More broadly, where do I see my future as a physician? Finally, professional identity formation is associated with lower rates of burnout in medical learners and appears to be a protective factor for physician mental health (Monti et al., 2025).
As we’ve seen, a performance art perspective to medicine can be helpful for both patients and physicians. But just as important as it is to perform, it is equally important to be able to leave the stage.
There are shifts where the performance becomes exhausting. I often think of emergency medicine as a profession of emotional labor, with so much of our work involving being present with people on their worst days. The most challenging shifts are not always the busiest ones, but the ones where we give the most of ourselves emotionally.
Caring for people in these moments can take a toll on the physician and many emergency physicians will experience vicarious trauma. This repeated exposure to suffering can lead to compassion fatigue and burnout, which is associated with higher levels of depression, anxiety, substance use, and leaving the profession. (Jeanmonod et al., 2024; Garnett et al., 2023).
In fact, a study from Turkey found that 22% of emergency physicians met the diagnostic criteria for PTSD in the DSM5 (Bahadirli & Sagaltici, 2021).
Worst of all, we have a job that forces us to just keep going when we experience immense second-hand and sometimes first hand loss.
In the case of the Pitt, art imitates life, but perhaps there is room for life to also imitate art.
In the performing arts, actors regularly perform scenes that are emotionally distressing. For actors to perform distress over and over again, the performance art world now places high importance on psychological safety and exiting their on-stage role- also known as de-roling. When actors are unable to de-role, they can suffer significant mental health challenges.
In the world of medicine, we also suffer greatly when we don’t de-role.
There are multiple techniques for de-roling that you can try on your next shift.
- Alba step out technique
- This is a technique used as part of the Alba Emotion Technique developed by Susana Bloch and Patricia Angelin. The technique is taught in the performing arts and is a form of grounding that uses deep breathing, arm movement, and eye contact to release tension in the body. (Bailey & Dickinson, 2022)
- The dress shop
- This technique involves miming taking off a costume at the end of their performance. This can also be done with a real costume or prop, for example the act of removing the stethoscope from your neck at the end of a shift. (Bailey & Dickinson, 2022)
- Closing ritual
- This technique involves something you do after a performance to signal to your brain that it is completed. For example, listening to certain music on the drive home or exercising after work. (Bailey & Dickinson, 2022)
Of course, there are times when this is not enough and we need to lean on others for support, whether that is a friend, a peer support group, or a therapist or counsellor. Even so, much of the support we rely on comes from those working alongside us. Like in theatre, these backstage connections with peers and colleagues can be essential in helping us process and recover from challenging experiences.
Conclusions
- Emergency medicine is a career filled with performance.
- Recognizing the opportunities for performance within our jobs can help us be better in those moments and not leave it up to chance.
- We are performing for good reasons and we can use multiple techniques from theatre to convey the empathy and compassion we want our patients to feel from us.
- However, it is important to understand when and how to de-role so we can continue to do the challenging work that we do day in and day out.
References
Bahadirli, S., & Sagaltici, E. (2021). Post-traumatic stress disorder in healthcare workers of emergency departments during the pandemic: A cross-sectional study. The American journal of emergency medicine, 50, 251–255. https://doi.org/10.1016/j.ajem.2021.08.027
Bailey, S. & Dickinson, P. (2022). The Importance of Safely De-roling. https://www.researchgate.net/publication/361379066_The_Importance_of_Safely_De-roling
Bendapudi, N. M., Berry, L. L., Frey, K. A., Turner Parish, J., & Rayburn, W. L. (2006). Retrieved from https://www.mayoclinicproceedings.org/article/S0025-6196(11)61463-8/fulltext
Case, G. A., & Brauner, D. J. (2010). Perspective: The doctor as performer: a proposal for change based on a performance studies paradigm. Academic medicine : journal of the Association of American Medical Colleges, 85(1), 159–163. https://doi.org/10.1097/ACM.0b013e3181c427eb
Cruess, S. R., Cruess, R. L., & Steinert, Y. (2019). Supporting the development of a professional identity: General principles. Medical Teacher, 41(6), 641–649. https://doi.org/10.1080/0142159X.2018.1536260
Dopelt, K., Bachner, Y. G., Urkin, J., Yahav, Z., Davidovitch, N., & Barach, P. (2022). Perceptions of Practicing Physicians and Members of the Public on the Attributes of a “Good Doctor”. Healthcare, 10(1), 73. https://doi.org/10.3390/healthcare10010073
Gao, L., Peranson, J., Nyhof-Young, J., Kapoor, E., & Rezmovitz, J. (2019). The role of “improv” in health professional learning: A scoping review. Medical Teacher, 41(5), 561–568. https://doi.org/10.1080/0142159X.2018.1505033
Garnett, A., Hui, L., Oleynikov, C., & Boamah, S. (2023). Compassion fatigue in healthcare providers: a scoping review. BMC health services research, 23(1), 1336. https://doi.org/10.1186/s12913-023-10356-3
Grossman CE, Lemay M, Kang L, et al. Improv to improve medical student communication. Clin Teach. 2021;18:301–306. https://doi.org/10.1111/tct.13336
Howe LC, Leibowitz KA and Crum AJ (2019) When Your Doctor “Gets It” and “Gets You”: The Critical Role of Competence and Warmth in the Patient–Provider Interaction. Front. Psychiatry 10:475. doi: 10.3389/fpsyt.2019.00475
Jeanmonod, D., Irick, J., Munday, A. R., Awosika, A. O., & Jeanmonod, R. (2024). Compassion Fatigue in Emergency Medicine: Current Perspectives. Open access emergency medicine : OAEM, 16, 167–181. https://doi.org/10.2147/OAEM.S418935
Kaplan-Liss, Evonne & Lantz-Gefroh, Valeri & Bass, Elizabeth & Killebrew, Deirdre & Ponzio, Nicholas & Savi, Christine & O’Connell, Christine. (2017). Teaching Medical Students to Communicate With Empathy and Clarity Using Improvisation. Academic Medicine. 93. 1. 10.1097/ACM.0000000000002031.
Landry-Wegener, B. A., Kaniecki, T., Gips, J., Lebo, R., & Levine, R. B. (2023). Drama Training as a Tool to Teach Medical Trainees Communication Skills: A Scoping Review. Academic medicine : journal of the Association of American Medical Colleges, 98(7), 851–860. https://doi.org/10.1097/ACM.0000000000005121
Monti, M., Carrard, V., Bourquin, C., & Berney, A. (2025). Association Among Professional Identity, Burnout, and Mental Health in Medical Students: A Cross-Sectional Study. Academic medicine : journal of the Association of American Medical Colleges, 100(11), 1298–1306. https://doi.org/10.1097/ACM.0000000000006175
Neufeld, A., & Malin, G. (2024). Cultivating physician empathy: a person-centered study based in self-determination theory. Medical education online, 29(1), 2335739. https://doi.org/10.1080/10872981.2024.2335739
Sarraf-Yazdi, S., Goh, S., & Krishna, L. (2024). Conceptualizing Professional Identity Formation in Medicine. Academic medicine : journal of the Association of American Medical Colleges, 99(3), 343. https://doi.org/10.1097/ACM.0000000000005559
Smith, A., Kemp, O., & Christie, S. (2021). Creating empathetic doctors through art: art-based teaching as a tool for understanding the patient experience, such as miscarriage. Korean journal of medical education, 33(4), 431–434. https://doi.org/10.3946/kjme.2021.203
