
Blood tests (especially complete blood counts and coagulation markers) are some of the most commonly ordered investigations in both the emergency department and the hospital at large. It’s important for us as emergency physicians to have an excellent understanding of the various pathophysiologic abnormalities we may encounter when we see the results of these blood tests. We also need to understand when to act, prior to any results returning.
My hope is that this blog post will leave you with some new hematology pearls to inform your emergency medicine practice, regardless of whether you’re PGY-2 or PGY-20. Part 1 will cover Hemophilia, and Part 2 will cover Hemolytic Anemias and Thrombotic Microangiopathies (TMAs).
Objectives:
- Hemophilia:
- Approach to bleeding hemophilia patients
- Approach to the hemophilia patient with a non-bleeding chief complaint
- Hemolytic anemias:
- When to suspect them & optimal ED workup
- Thrombotic microangiopathies (TMAs)
- When to suspect them, optimal ED workup, & management considerations
Hemophilia Basics
- Hemophilia is an inherited bleeding disorder.
- Genetics: X-linked disease — the majority of affected patients are male.
- Female patients who are carriers can also be symptomatic.
- One-third of hemophilia cases are the result of spontaneous mutations without a prior family history.
Hemophilia Classification
- Hemophilia A
- Factor VIII (8) deficiency
- Five times more common than hemophilia B
- 1 in 5,000 live male births in Canada
- Hemophilia B
- Factor IX (9) deficiency
- 1 in 25,000 live male births in Canada
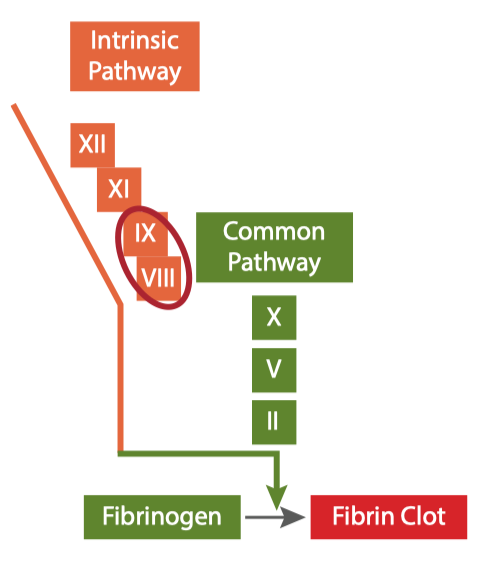
Image source: Bloody Easy Coagulation Simplified 2nd edition 2019
Factors VIII and IX are involved in the intrinsic pathway of the coagulation cascade, so the coagulation test we expect to see an abnormal result in is the activated partial thromboplastin time (APTT). A normal APTT, however, does not rule out milder forms of hemophilia.
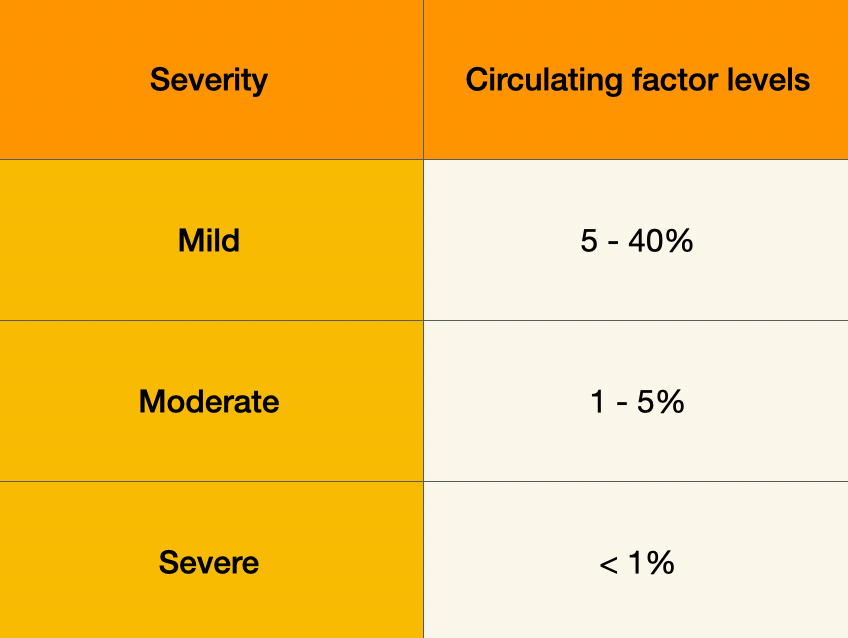
Hemophilia Severity
In addition to A and B, the disorder can be further classified by its severity. According to the International Society on Thrombosis and Hemostasis (ISTH), the severity is determined based on the plasma activity levels of either factor VIII or IX. In severe hemophilia, compared to the average person who does not have hemophilia, patients’ serum levels of factor VIII or IX are about 99% lower. Even in mild hemophilia, patients can have a reduction in circulating factor levels by almost 60% in the mildest cases.
Our approach to the hemophilia patient in the ED will be guided by guidelines from the:
- Canadian Hemophilia Society
- Ontario Regional Blood Coordinating Network (ORBCoN)
- World Federation of Hemophilia (WFH)
- National Bleeding Disorders Foundation (NBDF – USA)
Hemophilia History
For the ambulatory, non-critically ill hemophilia patient, there are a few key points we need to identify on history:
-
Hemophilia A or B
-
Mild, moderate, or severe
-
Hemophilia treatment plan
Many hemophilia patients will have an emergency plan documented by their hematologist in case of serious bleeding, often on a treatment card they carry or embedded within your hospital network’s electronic medical record. Some patients will already be on prophylaxis at home.
Typically, for a patient to present to the ED, this represents the potential for a serious bleed, as many minor bleeds are dealt with at home by patients.
Where is the Known or Suspected Bleed?
The cornerstone of emergency management of the hemophilia patient is that history determines treatment. In deciding whether or not to give factor replacement to a hemophilia patient, history is the only variable we need in the ED. There is no role for lab tests or imaging before factor replacement if a potential bleed is suspected. Physical exam can help confirm the objective presence of a bleed, but a normal physical exam cannot rule out potential major bleeding.
Canadian guidelines separate potential bleeds into two categories:
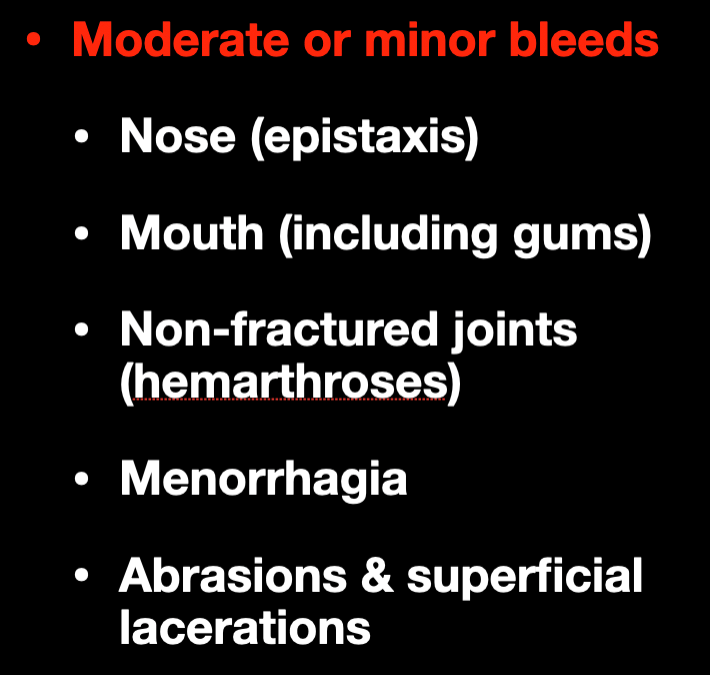
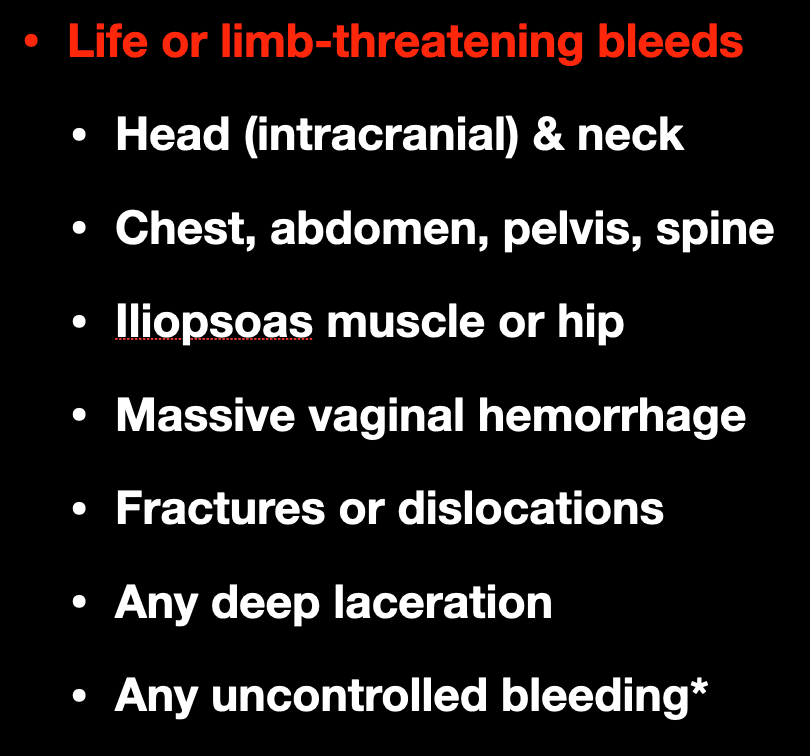
Life- or limb-threatening bleeds involve areas of the body in which bleeding would be catastrophic, either from mass effect, or from hemorrhagic shock and hemodynamic compromise from a massive amount of occult bleeding.
Any of the minor bleeds just listed on the previous slide can become a life- or limb-threatening bleed if not controlled, such as epistaxis in a hemophilia patient that doesn’t stop, or oral bleeding that compromises the airway.
Treatment of the Bleeding Hemophilia Patient
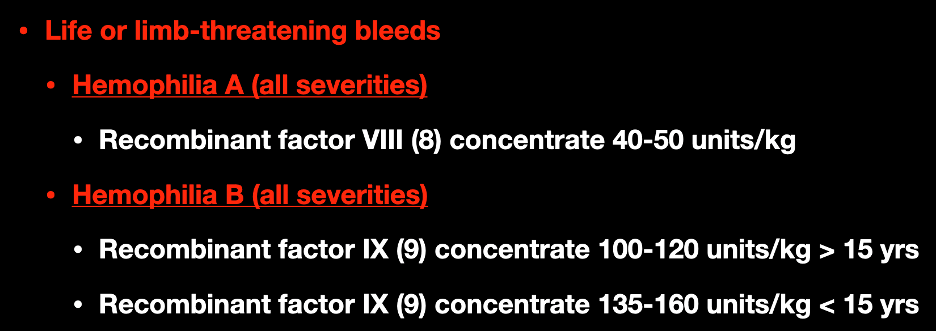
Bleed severity guides treatment, and the CHS dosing for both hemophilias is shown on this slide. Recall that in severe hemophilia, patients can have circulating factor levels that are 1% of the normal activity level. The goal in major bleeds is to raise this level to 100% as promptly as possible. One unit of factor VIII tends to increase serum factor activity levels by 2%, whereas one unit of factor IX tends to increase serum factor activity levels by 1%, which is why there is a dosing difference.
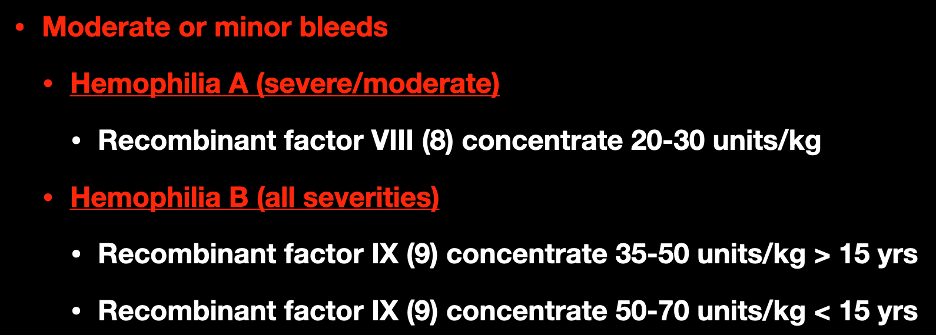
For moderate or minor bleeds, the doses of factors VIII and IX are correspondingly lower, as it is not necessary to raise serum factor levels to 100%. The American NBDF guidelines specifically support rounding up when dosing factor concentrates if half a vial remains after weight-based dosing. A higher dose of factor concentrate only increases the length of therapeutic effect and does not put the patient into a hypercoagulable state. Half-life of factor concentrate depends on age and BMI, but half-life for standard factor replacement is about 12 hours in adults. It’s shorter in younger children and increases with age.

The Canadian, American, and WFH guidelines also support DDAVP for mild-severity patients or carriers of hemophilia A. It is important to note that these patients should have a documented factor VIII response to DDAVP previously by their hematologist. They should not be receiving DDAVP for a minor bleed for the first time in the ED, without specialist consultation.
Hemophilia Patients with Massive Hemorrhage
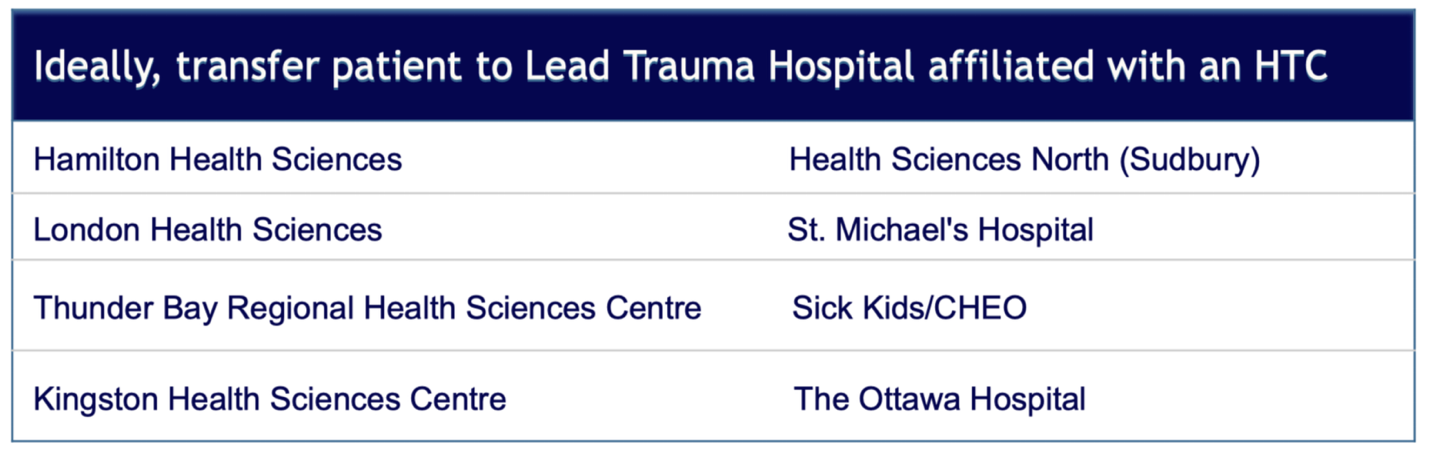
Image source: ORBCoN Provincial Massive Hemorrhage Toolkit v1 Jul 2020
In Ontario, for bleeding disorder patients with trauma and massive hemorrhage, ORBCoN recommends treating with major factor replacement and transferring to an HTC or Hemophilia Treatment Centre. In our province, functionally all the Level 1 Trauma Hospitals are also Hemophilia Treatment Centres.
For all of the scenarios mentioned, if you’ve given a dose or are thinking you may have to give a dose of factor replacement, you should be calling your local hematologist or nearest Hemophilia Treatment Centre. These patients will need personalized specialist guidance on how long they should be monitored if admitted, guidance on when to re-dose factors if necessary, and a solid discharge plan if being sent home.
For all of the scenarios I’ve just mentioned, if you’ve given a dose, or are thinking you may have to give a dose of factor replacement, you should be calling your local Hematologist or nearest Hematology Treatment Centre. These patients will need personalized specialist guidance on how long they should be monitored if admitted, guidance on when to re-dose factors if necessary, and a solid discharge plan if being sent home.
Other Hemostatic Agents
FFP & Cryoprecipitate
Broadly speaking, the WFH recommends against using FFP or cryoprecipitate for the treatment of hemophilia, as factors VIII and IX concentrates are much more effective. However, the WFH recognizes that not everywhere has access to factor concentrates. If you find yourself in a situation where you cannot order factor VIII or IX, and your patient doesn’t have factor concentrate from home, cryoprecipitate is preferable for hemophilia A, and FFP is preferable for hemophilia B, although it can be used for both.
TXA & 4-factor prothrombin complex concentrates (4F-PCC)
The WFH recommends TXA either alone or as an adjunct to other medications, particularly for controlling mucosal bleeding such as epistaxis, oral bleeds, GI bleeding, or vaginal bleeding.
Notably, the guidelines recommend against any use of PCC for hemophilia B, as it increases the risk of thrombosis and DIC in the setting of surgery, liver disease, or simultaneous TXA use. PCC is different from activated PCC, which can be used in patients known to have antibodies to traditional factor concentrates.
Case 1 – Hemophilia
- Tim, 40 M
- Severe hemophilia A
- Riding his bike, fell, hit his helmeted head on the pavement
- No external signs of trauma, but severe headache
- All vitals within normal limits
What should be our next step in management?
He’s a 70 kg man who, based on the history, you suspect may have an intracranial hemorrhage. You order a CT head but, at the same time, you appropriately order a major dose of factor VIII concentrate based on your suspicion of ICH. You diagnose Tim with a small SDH, and he gets admitted for further observation and management.
Case 2 – Hemophilia B
Tim’s friend Jim has severe hemophilia B. He was riding an electric scooter, helmeted, when he was hit by a car and landed on the ground, hitting his head. His physical exam is eerily similar to his friend Tim’s, with no signs of external trauma, just a severe headache. Because you’re now a master of hemophilia, you order some factor IX concentrate immediately after seeing him.
A few moments later, a nurse calls you over, as Jim is now hypotensive, having difficulty breathing, and has a new rash shortly after receiving his factor IX infusion. You quickly identify that he’s having an anaphylactic reaction, administer the appropriate dose of epinephrine, and stop the infusion.
The medical student working with you asks you what happened?
Inhibitors
Unfortunately, some hemophilia patients develop antibodies to the exogenous factors needed to replace their factor deficiency. These antibodies are referred to as inhibitors. They typically develop within the first 20 exposures to exogenous factor replacement. For patients with high levels of inhibition, they just won’t respond to appropriate doses of factor replacement
Hemophilia A Inhibitors
Hemophilia B inhibitors
Jim, unlike Tim, has severe hemophilia B. In contrast to hemophilia A, hemophilia B factor IX inhibitors are almost exclusively seen in severe hemophilia B. The incidence is about 5%, and previously undiagnosed factor IX inhibition can present with poor response to factor replacement, nephrotic syndrome, or, in Jim’s case, anaphylaxis.
The management of the bleeding hemophilia patient with inhibitors is complex and nuanced. It may include recombinant factor 7a, or activated PCC (FEIBA). For these patients, especially, we should be phoning Hematology early to guide management if no documented plan exists. Think about inhibitors in Hemophilia B patients who have an anaphylactic reaction to factor 9 concentrate, or in any hemophilia patient who doesn’t seem to be responding to appropriate doses of factors.
Case 3: The non-bleeding hemophilia patient
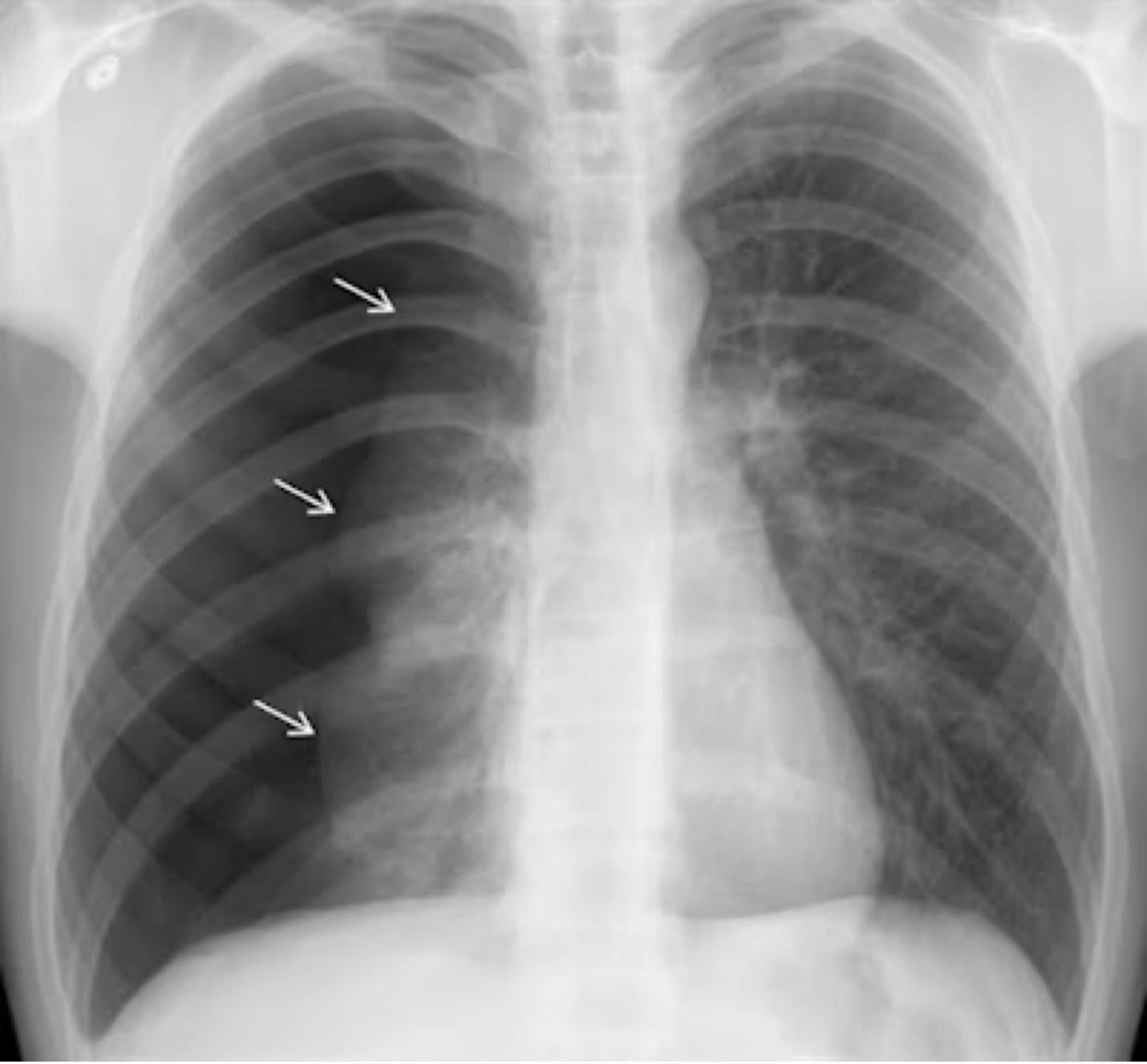
Image: Images courtesy of Dr. Paras Lakhani (https://www.auntminnie.com/imaging-informatics/artificial-intelligence/article/15619315/ai-can-spot-large-pneumothoraces-on-chest-x-ray)
Let’s say Tim came into your ED with atraumatic dyspnea and was found to have a large spontaneous pneumothorax. He’ll need a pigtail or a chest tube, but you’re not sure if there are guidelines around factor replacement in the hemophilia patient who isn’t bleeding yet but will be soon secondary to your procedure.
What is the approach?
Both the WFH and the American guidelines recommend treatment with factor concentrates before invasive diagnostic procedures such as arterial lines, central lines, lumbar punctures, chest tubes, and arthrocentesis. The dose given should be a major dose, enough to elevate their serum factor activity to 100%.
Hemophilia Take-Home Points
-
Immediate treatment is indicated based on history alone for hemophilia patients with a potential bleed.
-
Whenever possible, use pure factor concentrates and TXA if indicated for bleeding hemophilia patients. FFP or cryoprecipitate should be limited to resource-limited settings.
-
Replace factor levels to 100% before any invasive procedures.
-
Call your local hematologist for any hemophilia patients with potential bleeds.
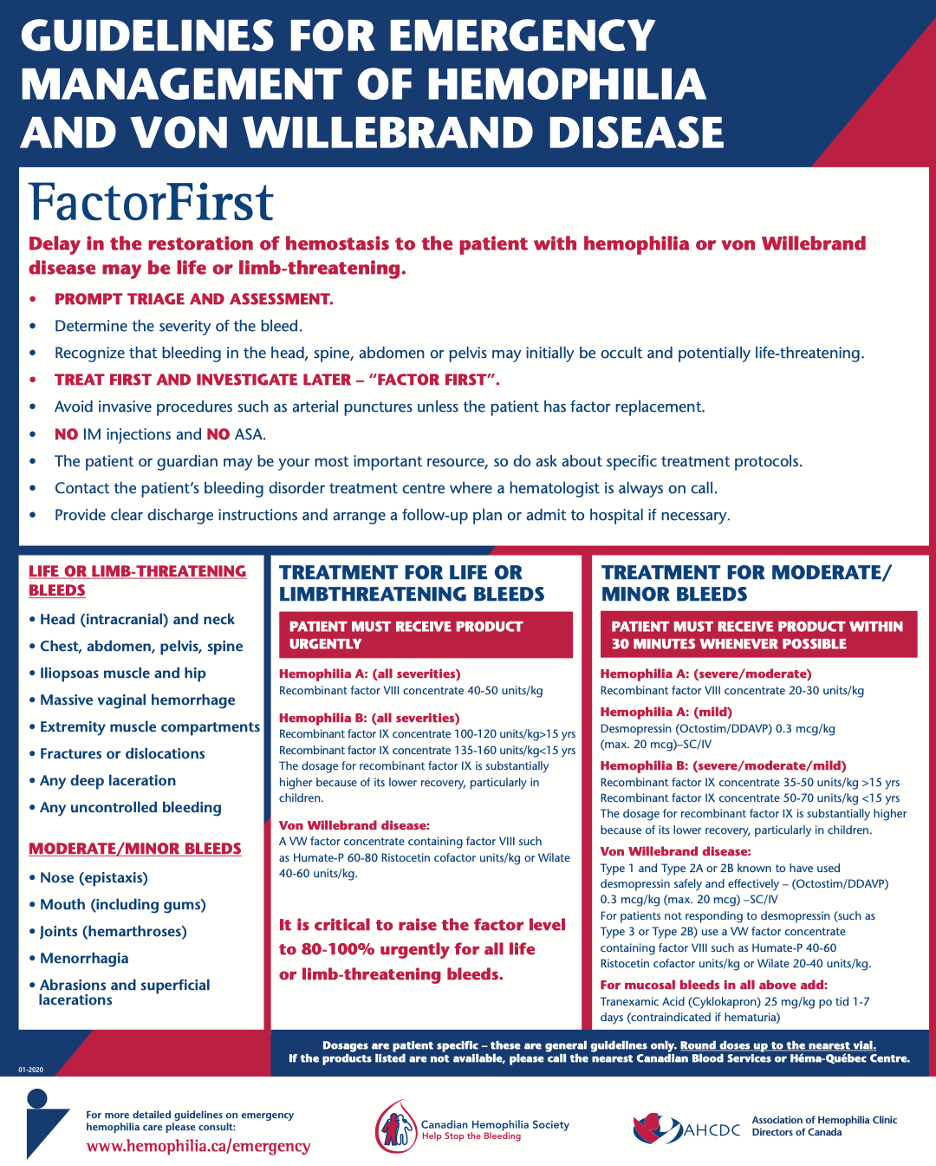
Image: Factor First poster – Canadian Hemophilia Society
Stay tuned for part 2 for more EM-focused pearls on hemolytic anemias and thrombotic microangiopathies.
References
- https://onlinelibrary.wiley.com/doi/10.1111/jth.12672
- https://www.acpjournals.org/doi/10.7326/M19-1208?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
- https://onlinelibrary.wiley.com/doi/10.1111/hae.14046
- https://www.hemophilia.ca/emergency/
- https://www.ahcdc.ca/
- https://transfusionontario.org/en/category/bloody-easy-e-tools-publications/bloody-easy-for-healthcare-professionals/
- https://www.bleeding.org/healthcare-professionals/guidelines-on-care/masac-documents/masac-document-257-guidelines-for-emergency-department-management-of-individuals-with-hemophilia-and-other-bleeding-disorders
- https://www.sciencedirect.com/science/article/abs/pii/S0735675722001309?via%3Dihub
- https://link.springer.com/article/10.1007/s43678-024-00780-7
