

“Don’t put it in your mouth!” – a quote from every parent at some point when raising their child, or a classic 80s Canadian commercial. Sometimes, though, this warning comes too late or goes unheeded. What do we do in the ED when we see a patient who has ingested something? The goal of this Grand Rounds summary is to review both caustic and button battery ingestions, their mechanism of injury, and what to do when this patient presents to the ED. For other toxicology-related reading, see the attached articles by Dr. Seliga, Dr. Endres, and Dr. Berliant.
By the end of this blog post, you should be able to:
1. Understand the chemistry and pathophysiology that leads to injury in caustic ingestions.
2. Know where to find information regarding caustic substances.
3. Have an approach to patients who present to the ED with intentional and unintentional caustic ingestions.
4. Understand the mechanism of injury in button battery ingestion.
5. Have an approach to initial treatment and management of patients who present with button battery ingestion
Caustic Ingestions
What Are Caustic Substances?
These are substances that produce tissue damage on contact. They can be classified as acidic or alkaline.
- Alkaline Substances: these substances are proton acceptors, which means dissociated hydroxide ions penetrate the tissue surface, therefore resulting in liquefactive necrosis (Wightman & Fulton, 2019) (Hoffman et al., 2020)
- Acidic Substances: these substances are proton donors – when they come into tissue contact hydrogen ions react with epithelial cells causing injury and formation of an eschar in a process known as coagulation necrosis (Wightman & Fulton, 2019) (Hoffman et al., 2020)
The extent of injury is variable, wth many contributing factors such as concentration, volume, pH, duration of contact, and titratable alkaline/acidic reserve (TAR).
- TAR: amount of neutralization needed to bring the pH to physiologic levels
- There is an increased likelihood of injury at the extremes of pH, namely acids with pH less than 2 and alkalis with pH greater than 10; however, it should not be relied on as we know based on the TAR some substances with near neutral pH can still cause significant injury
Evaluating Caustic Ingestions
Caustic ingestions may be either unintentional or intentional. Unintentional substances are typically pediatric and explorative in nature, while intentional ingestions are often of suicidal intent (Hall et al., 2018). When evaluating a patient presenting after a caustic ingestion, consider the following:
- Type and amount of substance; can search for specifics in Material Safety Data Sheets
- Involve poison control centre to aid in this process(Bonavina et al., 2015)
- Prioritize airway evaluation (these patients present with a potentially dynamic airway with swelling secondary to edema)
- If one needs to intubate, there may be difficulty passing the tube with risk of iatrogenic injury (Bonavina et al., 2015). For more information on difficult airway management, see our blog post here
- Presence of any airway distress secondary to injury/edema of upper airways vs aspiration and subsequent pneumonitis to lower airways (Hall et al., 2019)
- Using bedside adjuncts, including chest and abdominal radiographs (Bonavina et al., 2015)
- GI Injuries: acutely, there is concern for a GI injury; chronically, strictures may occur (Hall et al., 2019) (Hoffman et al., 2020)
- Although oral mucosal lesions are common (seen in up to 60% of presentations with severe injury in one review), their absence should not be reassuring. In one study up to 12% of patients were found to have significant esophageal or gastric injury had no visible oral mucosal lesions. (Hall et al., 2019) (Temiz et al., 2022)
For investigations, we recommend the following:
- Labs: CBC, lytes, extended lytes, VBG, Cr, Urea, Glucose, LFTs as well as acetaminophen, ASA and EtOH to assess for treatable co-ingestions. (Hoffman et al., 2020) (Wightman & Fulton, 2019) (Chen at al., 2022)
- These patients can also have systemic decompensation and metabolic derangements, for example metabolic acidosis secondary to acidic ingestion.
- They may have a raised anion gap or not depending on the dissociated anion in the acid. (Hoffman et al., 2020)
- Imaging: Standard evaluation for these patients has relied on EGD to assist with grading and staging and to determine need for emergent surgical intervention; however, studies have demonstrated that CT scan can accurately assess patients and aid in the decision for patients with significant injury on who might benefit from surgery. (Bonavina et al., 2015) (Betalli et al., 2008) (Ryu et al., 2009)
Managing Caustic Ingestions in the ED
The PADIS Caustic Ingestion Guideline divides management into high and low risk ingestions:
- High risk ingestions: require GI consult and scope within 24 hours of presentation
- An ingestion is considered high risk based on the following characteristics:
- Symptomatic intentional ingestions
- Unintentional ingestions with stridor or gastrointestinal bleeding
- Unintentional ingestions with 2 or more of the following: vomiting, drooling, refusal to drink fluids, dysphagia, odynophagia, abdominal pain
- An ingestion is considered high risk based on the following characteristics:
- Low Risk Ingestions: require 6 hours observation and trial po intake – if pass trial of P.O. they can be discharged home, if not then patients require a GI consult
- An ingestion is considered low risk based on the following characteristics:
- Asymptomatic unintentional ingestions
- Ingestions without stridor, gastrointestinal bleeding, or abdominal pain
- Ingestions with 1 of the following: vomiting, drooling, refusal to drink fluids, dysphagia, odynophagia
- An ingestion is considered low risk based on the following characteristics:
- General treatment for caustic ingestions:
- From the ED perspective, routine antibiotics are NOT recommended (in the absence of perforation or mediastinitis), nor are routine steroids (Bonavina et al., 2015) (Hall et al., 2019)
- There is equivocal evidence for pantoprazole 80 mg IV bolus. The goal is GI protection (Bonavina et al., 2015) (Levine et al., 2024) (Hoffman et al., 2020)
- Anti-emetics to avoid secondary injury (Bonavina et al., 2015)
- There is no role for decontamination
- No charcoal as can obscure scope findings (Hoffman et al., 2020)
- Avoid NG tubes as can increase risk of perforation (Bonavina et al., 2015)
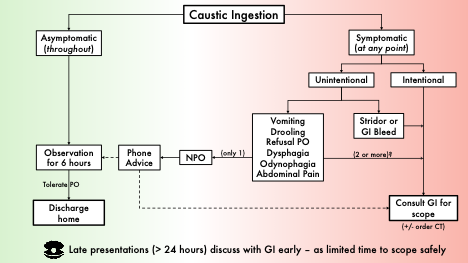
Assessment algorithm for caustic ingestions
Button Battery Ingestions

https://www.aboutkidshealth.ca/button-battery-injuries
Button Batteries: The Basics
Button batteries are becoming increasingly common. They are found in coin-shaped batteries in toys, watches, and remote controls. When ingestions occur, it is important for ED physicians to know how to manage them due to the injuries they cause.
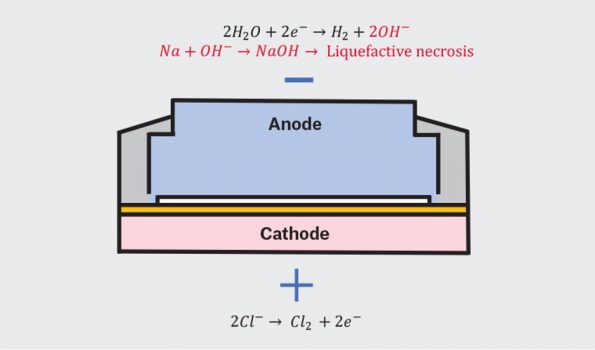
- Injury is not caused by leakage of the contents inside the battery, but rather the local reaction that occurs when the negative (anode) and positive (cathode) ends of the battery contact the esophageal tissue and the circuit is completed. This then results in rapid hydroxide accumulation at the level of the tissue producing an alkaline caustic injury (Jatana et al., 2013)
- Injury is still possible with spent battery, still contains residual power (Jatana et al., 2013)
- Injury is mediated by: size, voltage, tissue contact, fluid environment (Jatana et al., 2013)
- Possible injuries include: esophageal perforation, trachea-esophageal fistula, aorto-esophageal fistula and pneumothorax (Jatana et al., 2013) (Kramer et al., 2015) (Park & Burns, 2022)
- Possible complications include: vocal cord paralysis, esophageal stricture, spondylodiscitis, mediastinitis, and abscess formation (Jatana et al., 2013) (Park & Burns, 2022)
https://www1.racgp.org.au/ajgp/2022/july/button-battery-injury
Assessment of Button Battery Ingestions
In terms of imaging, plain radiograph is a rapid and safe imaging modality that typically provides sufficient detail to identify button batteries (Voelker et al., 2021) (Whelan et al., 2019).
- The features that are pertinent are the double halo or ring sign seen on the AP view, or a stepped appearance on lateral view.
- Note that small, thin batteries on lateral view may lose their stepped or beveled appearance. (Voelker et al., 2021) (Whelan et al., 2019) (Tokar et al., 2004)
- There are no reliable imaging features to distinguish stacked coins from button batteries, if unknown have to treat as button battery ingestion until proven otherwise (Torrecillas & Meier 2020) (Rossi et al., 2023)
Managing Button Battery Ingestions
NASPGHAN Society outlines the treatment of button battery ingestions below:
- Button batteries that are identified above the LES (either symptomatic or asymptomatic) require urgent specialist involvement for retrieval, given their risk for high mortality acute complications, and high morbidity chronic complications
- Asymptomatic patients with button batteries identified in the stomach (ie before the gastric outlet), require 24 h x-ray follow up to ensure the battery has moved out of the stomach
- Asymptomatic patients with button batteries past the gastric outlet do not require specific follow up, but instruct parents to monitor bowel movements to ensure passage, and strict return to care instructions for any symptoms
- Caveat: patients <5 years, and battery >20mm require endoscopic removal
- Symptomatic patients with button battery ingestion at any point in their GI tract require specialist involvement (ie GI or General Surgery)
Oral honey is recommended by the National Capital Poison Control Centre (in the US) and the European Society of Pediatric Gastroenterology, Hepatology And Nutrition position paper in Europe. Research has shown that honey may be helpful in neutralizing the pH change, as well as providing a viscous barrier (Schmidt et al., 2023) (Soto et al., 2019). However, it still remains a difficult entity to study.
- It is recommended that oral honey should follow timing of physiologic saliva production, therefore administer 10 ml of honey every 10 minutes for 6 doses. (Schmidt et al.,2023) (Soto et al., 2019)
- Incidence of esophageal perforation is incredibly rare (less than 2%) before 12 hours. This is based on review from 2019, which studied 290 cases of severe or fatal ingestions with 189 having esophageal perforation, so, within this 12-hour timeline administration is considered safe. If timing is unclear, we would recommend making the patient NPO and would avoid honey administration. (Soto et al., 2019)
- We would recommend avoiding oral honey in infants <1 year old given the risk of botulism. An alternative is sucralfate1g (5ml) q 10 minutes for a maximum of 3 doses (Schmidt et al., 2023)
References
Caustic Ingestion
Bonavina L, Chirica M, Skrobic O, Kluger Y, Andreollo NA, Contini S, Simic A, Ansaloni L, Catena F, Fraga GP, Locatelli C. Foregut caustic injuries: results of the world society of emergency surgery consensus conference. World Journal of Emergency Surgery. 2015 Sep 26;10(1):44.
Levine M, Finkelstein Y, Trautman WJ, Cao D, Schwarz E, Filip A, Cook L, Pathan SA, Obilom C, Liu J, Yanta J. Is EGD Needed in all Patients after Suicidal or Exploratory Caustic Ingestions?. Journal of Medical Toxicology. 2024 Jul;20(3):256-62.
Hall AH, Jacquemin D, Henny D, Mathieu L, Josset P, Meyer B. Corrosive substances ingestion: a review. Critical reviews in toxicology. 2019 Sep 14;49(8):637-69.
Ryu HH, Jeung KW, Lee BK, Uhm JH, Park YH, Shin MH, Kim HL, Heo T, Min YI. Caustic injury: can CT grading system enable prediction of esophageal stricture?. Clinical Toxicology. 2010 Feb 1;48(2):137-42.
Chen RJ, O’Malley RN, Salzman M. Updates on the evaluation and management of caustic exposures. Emergency Medicine Clinics. 2022 May 1;40(2):343-64
Hoffman RS, Burns MM, Gosselin S. Ingestion of caustic substances. New England Journal of Medicine. 2020 Apr 30;382(18):1739-48
Betalli P, Falchetti D, Giuliani S, Pane A, Dall’Oglio L, de’Angelis GL, Caldore M, Romano C, Gamba P, Baldo V, Caustic Ingestion Italian Study Group. Caustic ingestion in children: is endoscopy always indicated? The results of an Italian multicenter observational study. Gastrointestinal endoscopy. 2008 Sep 1;68(3):434-9.
Temiz A, Oguzkurt P, Ezer SS, Ince E, Hicsonmez A. Predictability of outcome of caustic ingestion by esophagogastroduodenoscopy in children. World journal of gastroenterology: WJG. 2012 Mar 14;18(10):1098.
Wightman R.S., & Fulton J.A. (2019). Caustics. Nelson L.S., & Howland M, & Lewin N.A., & Smith S.W., & Goldfrank L.R., & Hoffman R.S.(Eds.), Goldfrank’s Toxicologic Emergencies, 11e. McGraw-Hill Education. https://accesspharmacy.mhmedical.com/content.aspx?bookid=2569§ionid=210275165
Button Batteries
Jatana KR, Litovitz T, Reilly JS, Koltai PJ, Rider G, Jacobs IN. Pediatric button battery injuries: 2013 task force update. International journal of pediatric otorhinolaryngology. 2013 Sep 1;77(9):1392-9.
Whelan R, Shaffer A, Dohar JE. Button battery versus stacked coin ingestion: a conundrum for radiographic diagnosis. International journal of pediatric otorhinolaryngology. 2019 Nov 1;126:109627.
Schmidt YM, Muensterer O, Wendling-Keim D. The use of honey in button battery ingestions: a systematic review. Frontiers in pediatrics. 2023 Sep 28;11:1259780.
Rossi N, Reddy D, Coggins J, Watley DC, Pine HS, Daram S, Reddy DN, Whatley DC. Two Stacked Coins Mimicking an Esophageal Button Battery: A Case Presentation and Review of the Literature. Cureus. 2023 May 9;15(5).
Voelker J, Voelker C, Voelker J, Engert J, Schendzielorz P, Hagen R, Rak K. Button batteries and typical swallowed foreign bodies can be differentiated in high-resolution X-Rays. International journal of pediatric otorhinolaryngology. 2021 Mar 1;142:110604.
Tokar BA, Ozkan R, Ilhan HÜ. Tracheobronchial foreign bodies in children: importance of accurate history and plain chest radiography in delayed presentation. Clinical radiology. 2004 Jul 1;59(7):609-15.
Torrecillas V, Meier JD. History and radiographic findings as predictors for esophageal coins versus button batteries. International Journal of Pediatric Otorhinolaryngology. 2020 Oct 1;137:110208.
Jatana KR, Litovitz T, Reilly JS, Koltai PJ, Rider G, Jacobs IN. Pediatric button battery injuries: 2013 task force update. International journal of pediatric otorhinolaryngology. 2013 Sep 1;77(9):1392-9.
Soto PH, Reid NE, Litovitz TL. Time to perforation for button batteries lodged in the esophagus. The American Journal of Emergency Medicine. 2019 May 1;37(5):805-9.
Kramer, R. E., Lerner, D. G., Lin, T., Manfredi, M., Shah, M., Stephen, T. C., … & Mamula, P. (2015). Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. Journal of pediatric gastroenterology and nutrition, 60(4), 562-574.
Park, S. J., & Burns, H. (2022). Button battery injury: An update. Australian journal of general practice, 51(7), 471–475. https://doi.org/10.31128/AJGP-03-21-5873

