

In this month’s Journal Club, we explored the highly debated topic of video laryngoscopy versus direct laryngoscopy and its application in the prehospital setting.
Background
There exists a breadth of research which compares video laryngoscopy (VL) to direct laryngoscopy (DL) in the hospital setting. It is known that multiple attempts at tracheal intubation is associated with increased harm such as hypoventilation, airway trauma and esophageal intubations. A common method of assessing efficacy and safety of intubation includes quantification of first pass success during intubation. Although in-hospital studies generally demonstrate increased first pass success in VL over DL, there is a lack of evidence in the pre-hospital setting.
Objectives
The objective of this study is to compare first-pass intubation success rates between VL and DL in critically ill patients undergoing pre-hospital tracheal intubation.
Methods
- Design: Single-center, retrospective service evaluation.
- Setting: Hampshire & Isle of Wight Air Ambulance (UK) – HEMS.
- Period: 1 Nov 2018 – 22 Apr 2024.
|
Research Question:
|
Key Results
Overall, 1,279 patients were included in the study where 799 underwent DL and 480 underwent VL. Demographics were comparable across the groups. Notably, the patient indication for intubation of ‘cardiac arrest’ had an increase in number of VL intubations compared to DL which may speak to the anatomically more reassuring intubations.
Table 1.0: Primary and secondary outcomes comparing VL to DL including all professional trainings.
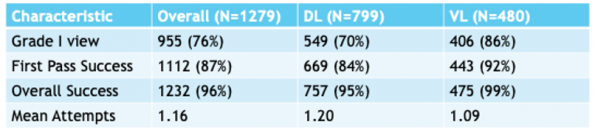
First-pass success was greater in the VL group (92%) compared to the DL group (84%). There was also an increase in overall successful ETT intubation in the VL group compared to DL (99% and 95%, respectively). Finally, VL was associated with better glottic views and fewer intubation attempts than DL. All values were statistically significant with p < 0.001. Cohort sub-analysis demonstrated that there was global improvement in first pass success and overall successful intubation regardless of professional background (anesthetist vs EM physician vs paramedic).
Strengths
This study is one of the largest real-world studies in this topic in the prehospital setting. Given its long timeframe including patients from 2018 to 2024, it also reflects the evolving clinical practice over multiple years.
Limitations
The biggest limitation of this study is the retrospective design which can result in possible documentation or selection bias. Furthermore, the selection of VL versus DL was left to operator choice allowing for clinician preference to possibly influence results. However, this allowance of choice my be more realistic in clinical settings when conditions are not suitable for VL use. Finally, there is no patient-centered outcome data (ie., survival, neurologic outcome) given the basis of using surrogate outcomes (ie., first-pass success).
Bottom Line
It is clear from this large retrospective study that VL outperforms DL for pre-hospital intubations that are performed by critical care teams. Given the large push towards VL in hospital settings, it appears that VL is now becoming more of a standard of care emphasizing the need for evaluation of pre-hospital airway protocols and quality improvement efforts. Further, these findings support routine adoption of VL as the primary airway management tool in pre-hospital settings as long as there are appropriate training frameworks in place.