
Blood pressure management in trauma is one of the most deceptively complex decisions we make in the emergency department. In the first hour of resuscitation, competing physiologic priorities collide: permissive hypotension may protect clot integrity in hemorrhagic shock, while the brain and spinal cord demand higher perfusion pressures to prevent irreversible secondary injury. Add to this the reality of polytrauma, variable guideline recommendations, and a heterogeneous evidence base, and it becomes clear that there is no single “correct” target. In this post, we synthesize the available literature and expert opinion to provide a pragmatic, bedside approach to blood pressure targets across hemorrhagic shock, traumatic brain injury, and spinal cord injury, with a focus on how to navigate these competing priorities in real-world ED practice.
The TL/DR; summary
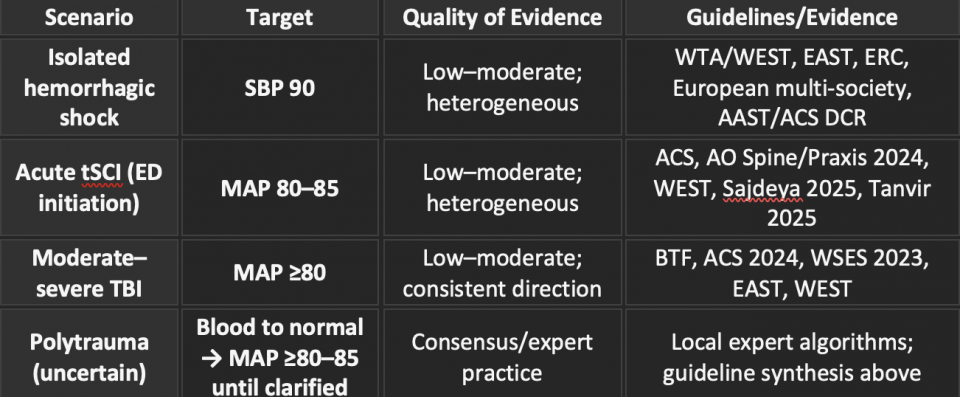
Based on an in depth literature review of the current guidelines on the 3 topics and opinion from trauma experts I support the use of the following targets and approach for patient with shock presentation related to trauma:
Why BP Targets Matter
The first hour decides trajectory: hemorrhage kills early, while the brain and spinal cord suffer secondary ischemic injury from insufficient perfusion. The challenge is that the pressure required to preserve clot stability may compromise CNS perfusion, while the pressure needed to adequately perfuse the CNS may worsen ongoing bleeding. This creates a clinical grey zone when we are trying to determine initial blood pressure targets in these patients. Furthermore, when we examine the evidence for isolated injury patterns, there is significant variability across guideline recommendations, which leaves us deciding whether to follow one approach strictly or attempt to integrate multiple recommendations without always understanding the strength or limitations of the underlying evidence.
In this post, we will examine the available evidence for these individual injury patterns and provide an up to date review of the literature. We will then build on this foundation and apply it to the undifferentiated polytrauma patient, which more accurately reflects the reality of emergency department presentations.
Isolated Hemorrhagic Shock
Pathophysiology and rationale
Higher intravascular pressures can disrupt nascent clot formation in noncompressible hemorrhage. This disruption leads to ongoing uncontrolled bleeding and consumption of coagulation factors, which can progress to disseminated intravascular coagulopathy, multiorgan failure, and ultimately death if not rapidly addressed.
Early evidence base
A landmark paper published in NEJM by Bickell et al. (Bickell et al., 1994) was the first randomized controlled trial examining permissive hypotension prior to definitive operative control. Patients were randomized to a “hypotensive” group, meaning no fluid resuscitation prior to the operating room, or a “normotensive” group, where fluids were administered to maintain a normal blood pressure at the discretion of the treating physician. They demonstrated a mortality benefit in the hypotensive group, with survival to discharge of 70% compared to 62%.
Current Guideline Recommendations
- Eastern Association for the Surgery of Trauma (EAST): Recommend a MAP of 50 in cases of pure hemorrhagic shock.
- They provide this recommendation based on a “landmark” paper by (Morrison et al., 2011) This was an interim analysis of a later published 2016 paper that demonstrated reduced post op coagulopathy and blood product use in a MAP of 50mmHg group compared to MAP of 65mmHg
- This was not replicated however in the later published final report by (Carrick et al., 2016) There was no difference in primary and secondary outcomes between the MAP 50 and MAP 65 group
- Western Trauma Association (WTA/WEST): Recommend a SBP target of 90mmHg (Croft et al., 2025)
- European Resuscitation Council (ERC): Recommend a SBP 80-90mmHg and MAP 50-60mmHg(Lott et al., 2025)
- European Guideline: In a joint guideline by major European associations (ESAIC/ESICM/ESTES/EuSEM/NATA) they made the recommendation to maintain a SBP 80–90mmHg or MAP 50–60mmHg.(Rossaint et al., 2023)
- Interestingly this was a Grade 1B recommendation based their interpretation of work by Tran et al. (Tran et al., 2018). and Safiejko et al.(Safiejko et al., 2022)
- However, when analyzing the individual systematic reviews and meta-analyses (as well as speaking to a publishing author), they would support a grade 3 recommendation based on their findings.
- AAST/ACS 2024 DCR: Recommend a SBP of 70-90mmHg. (LaGrone et al., 2024). Now it is important to note that this is absolutely contraindicated in cases of neurologic injury.
My overall interpretation of the literature is that the recommendation for permissive hypotension in isolated hemorrhagic shock reflects a Grade 3 level of evidence. With respect to specific targets, I am more inclined to maintain a systolic blood pressure of 90 mmHg in this population. The evidence supporting lower blood pressure targets has not demonstrated sufficient consistency across large, well-conducted randomized trials. This perspective is supported by discussions with local expert Dr. Alexandre Tran, a critical care physician and trauma surgeon. His interpretation aligns with this view: there is likely benefit to avoiding excessive blood pressure in these cases, but the optimal target remains unclear. Importantly, maintaining a systolic blood pressure around 90 mmHg is unlikely to result in significant end-organ dysfunction in most patients.
Practical Acute ED/Trauma Approach
If this is truly isolated hemorrhage, target a systolic blood pressure of 90 mmHg during active bleeding while simultaneously expediting massive transfusion protocol activation and definitive hemorrhage control.
Do not let the crystalloid debate paralyze your resuscitation. Even landmark massive transfusion trials included nontrivial amounts of crystalloid, and outcome benefits were not dependent on a “zero crystalloid” strategy. Use balanced blood products preferentially, but do not delay hemodynamic support if vascular access is limited or blood products are not immediately available.
Pearl: The moment you suspect traumatic brain injury or traumatic spinal cord injury, permissive hypotension no longer applies. You must shift to neuroprotective blood pressure targets based on the most clinically significant injury.
Acute Traumatic Spinal Cord Injury
Pathophysiology to the bedside
High cervical and upper thoracic injuries disrupt sympathetic tone, leading to unopposed parasympathetic activity. This results in vasoplegia, bradycardia, and reduced spinal cord perfusion following the initial mechanical injury. What follows is the secondary injury that we have the potential to influence. The spinal cord becomes vulnerable to ischemic injury due to inadequate blood flow, which is why our resuscitative strategies in these presentations focus on maintaining an elevated MAP to support perfusion.
In the ED, norepinephrine is the first-line vasopressor. Its alpha effects address vasoplegia, while its beta effects help counteract bradycardia. Other agents are available, but each comes with limitations. Phenylephrine may worsen reflex bradycardia. Dopamine has variable and less predictable hemodynamic effects. Epinephrine tends to produce excessive beta stimulation, which can be undesirable in this context.
The Shaky Evidence Base
- Early signals, such as Vale et al. 1997 (Vale et al., 1997), suggested improved neurologic outcomes with maintaining a MAP ≥85 for 7 days. However, this study had significant methodological limitations. It was uncontrolled, and the primary outcome was subjective and based on expert opinion. While it did report improved outcomes with higher MAP targets, the quality of the data is too limited to draw firm conclusions. At best, it served as hypothesis-generating work that informed future studies.
- Prospective and retrospective cohort studies, including Squair et al. 2017 (Squair et al., 2017) and Martin et al. 2015 (Martin et al., 2015), demonstrate associations between higher achieved MAP and improved neurologic outcomes. However, these studies do not establish causality. Importantly, drops below a MAP of 70 were not consistently associated with worse outcomes. It is therefore plausible that the observed association reflects injury severity, where patients with more severe spinal cord injuries present with more profound neurogenic or spinal shock, rather than a true treatment effect.
- Sajdeya et al. (Sajdeya et al., 2025) published the most recent randomized controlled trial in 2025. This study included 92 patients and compared a MAP target of 85–90 versus ≥65–70. There was no significant difference in outcomes at 6-month follow-up. However, the study had a 42% loss to follow-up, which significantly limits the reliability and interpretability of the results.
- Tanvir et al. (Tanvir et al., 2025) published the most up-to-date systematic review and meta-analysis, which found that a MAP <75–80 was associated with worse neurologic function based on ASIA scores. However, the included data were predominantly observational, with moderate to high heterogeneity, limiting the strength of the conclusions.
Current Guidance
- ACS Best Practices 2022: Recommends a MAP of 85–90 for 7 days (Grade 3) (Schroeder et al., 2022).
- This is largely a re-endorsement of their 2013 guideline (Walters et al., 2013), which relied heavily on a scoping review by Sabit et al. (Sabit et al., 2018). That review included 9 studies, of which 4 demonstrated benefit with a MAP of 85, while 5 showed no significant difference in neurologic outcomes based on ASIA scores. This inconsistency underpins the Grade 3 strength of recommendation.
- AO Spine/Praxis 2024 (Evaniew et al., 2024): Recommends a MAP target of 70–95 for 3–7 days (Grade 3). This represents a downgrade from their 2013 guideline, reflecting mixed outcome data as well as recognition of vasopressor-related harms, including skin ischemia and dysrhythmias, particularly in older cohorts treated with dopamine and phenylephrine.
- WEST: Recommends maintaining a MAP >85, with the greatest benefit observed when this target is achieved early, particularly within the first 12 hours of presentation (LaRiccia et al., 2024).
- EAST: Does not provide a formal MAP target but notes that there is limited evidence to support a target of 90 over 85 (Ploumis et al., 2010).
Expert Opinion
Given the variability in the literature and the wide range of recommended targets, I sought input from a local spine specialist. Dr. Stephen Kingwell, a spine surgeon at The Ottawa Hospital and director of the combined orthopaedic and neurosurgical fellowship, emphasized that the evidence base is low quality, which explains the heterogeneity in guideline recommendations.
In his practice, he targets a MAP of 80–85 for 7 days following injury. His rationale is that these injuries carry a high risk of permanent neurologic deficit, and if there is a potential intervention that carries relatively low risk and may offer benefit, it is reasonable to pursue it. This approach reflects a pragmatic interpretation of a signal in the literature, despite the absence of high-quality evidence.
Practical ED sequence
-
Rule out and treat hemorrhage first, prioritizing blood product resuscitation before initiating vasopressors.
-
When neurogenic shock predominates, initiate norepinephrine and target a MAP of 85. This represents a practical compromise that aligns with the majority of guideline recommendations and expert opinion.
Pearl: A MAP of 85 is not supraphysiologic. A normal blood pressure of 120/80 corresponds to a MAP of approximately 85, which can help contextualize this target when communicating with bedside teams and families.
Traumatic Brain Injuries
Key pathophysiologic difference: TBI is not ICH
Intracranial hemorrhage (ICH) is typically pressure dependent and often driven by arterial bleeding, where the goal is to limit further hemorrhage by controlling blood pressure. In contrast, traumatic brain injury (TBI)–related hemorrhage is often non–pressure dependent, involving venous bleeding, middle meningeal sources, parenchymal contusions, and shear injury. The primary threat in TBI is reduced cerebral perfusion pressure (CPP). Our main lever to preserve CPP in the acute setting is maintaining adequate MAP. Therefore, during early resuscitation, the priority is to avoid hypotension and ensure sufficient perfusion until definitive intracranial pathology is identified and managed.
Definite mortality and morbidity with hypotension
- Multiple observational datasets demonstrate a stepwise increase in mortality when SBP drops below 110 mmHg, with further increases in risk below 90 and 70 mmHg (Hasler et al., 2012).
- Pooled analyses, including the IMPACT dataset, describe a U-shaped relationship between blood pressure and outcomes, reinforcing that exposure to hypotension is consistently associated with worse outcomes (Brenner et al., 2012; Murray et al., 2007).
Guideline consensus
- Brain Trauma Foundation (BTF) 4th edition (Carney et al., 2016): Provides age-based recommendations with Grade 3 level evidence.
- SBP ≥110 for most adults aged 15–49 and ≥70 years
- SBP ≥100 for adults aged 50–69 years
- WEST: Recommends the same targets as the BTF.
- ACS 2024 / WSES 2023 / ERC: Largely converge on maintaining SBP ≥110 and MAP ≥80, all supported by Grade 3 level evidence (American College of Surgeons, 2024; Lott et al., 2025; Picetti et al., 2023).
Practical ED moves
In patients presenting with clear traumatic brain injury, there is consistent guideline support to maintain a MAP ≥80 during initial resuscitation.
The expert move: Based on expert opinion, prior to performing procedures that may precipitate hypotension, consider titrating vasopressors to transiently achieve a MAP ≥85.
Additional neuroprotective measures should be implemented alongside hemodynamic optimization. While maintaining MAP ≥80, ensure head elevation, appropriate analgesia and sedation, normocapnia, and use hyperosmolar therapy when indicated, while arranging neurosurgical consultation and ICP monitoring.
For more on ICP management, read on here.
Polytrauma – When Priorities Collide in Real Life
Blunt polytrauma rarely presents as “clean” hemorrhage or “pure” neurotrauma. In the setting of incomplete information, you need a default strategy that protects the brain and spinal cord without exacerbating bleeding, and one that can be clearly operationalized by the entire team. Your resuscitation strategy will need to be guided by findings from the primary survey and adjuncts obtained during resuscitation, including X-ray and PoCUS.
Phase 1 — Hemorrhage first
- Activate the massive transfusion protocol early.
- Resuscitate toward physiologic normal, targeting approximately SBP ~120 and/or MAP ≥65, to restore preload before initiating vasopressors.
Phase 2 — Neuro perfusion
- Add norepinephrine to achieve the highest relevant neuroprotective target while ongoing diagnostics are completed. Pragmatically, this means targeting a MAP ≥80–85, which supports early cerebral perfusion pressure in TBI and aligns with commonly recommended ranges in tSCI.
Phase 3 — Maintain
- Once the neuroprotective MAP target is achieved, establish your norepinephrine infusion and maintain it.\
- If the patient becomes hypotensive, increase the rate of volume resuscitation. Avoid under-resuscitating the hemorrhagic component of shock.
- If the patient becomes hypertensive, titrate down the vasopressor infusion accordingly.
References
American College of Surgeons. (2024). American College of Surgeons. Best Practices Guidelines: The Management of Traumatic Brain Injury. https://doi.org/10.15585/mmwr.ss6609a1
Bickell, W. H., Wall, M. J., Pepe, P. E., Martin, R. R., Ginger, V. F., Allen, M. K., & Mattox, K. L. (1994). Immediate versus Delayed Fluid Resuscitation for Hypotensive Patients with Penetrating Torso Injuries. New England Journal of Medicine, 331(17), 1105–1109. https://doi.org/10.1056/NEJM199410273311701
Brenner, M., Stein, D. M., Hu, P. F., Aarabi, B., Sheth, K., & Scalea, T. M. (2012). Traditional systolic blood pressure targets underestimate hypotension-induced secondary brain injury. Journal of Trauma and Acute Care Surgery, 72(5), 1135–1139. https://doi.org/10.1097/TA.0b013e31824af90b
Carney, N., Totten, A. M., Ullman, J. S., Hawryluk, G. W. J., Bell, M. J., Bratton, S. L., Chesnut, R., Harris, O. A., Rubiano, A. M., Tasker, R. C., Vavilala, M. S., Wilberger, J., Wright, D. W., & Ghajar, J. (2016). Guidelines for the Management of Severe Traumatic Brain Injury 4th Edition.
Carrick, M. M., Morrison, C. A., Tapia, N. M., Leonard, J., Suliburk, J. W., Norman, M. A., Welsh, F. J., Scott, B. G., Liscum, K. R., Raty, S. R., Wall, M. J., & Mattox, K. L. (2016). Intraoperative hypotensive resuscitation for patients undergoing laparotomy or thoracotomy for trauma. Journal of Trauma and Acute Care Surgery, 80(6), 886–896. https://doi.org/10.1097/TA.0000000000001044
Croft, C. A., Lorenzo, M., Coimbra, R., Duchesne, J. C., Fox, C., Hartwell, J., Holcomb, J. B., Keric, N., Martin, M. J., Magee, G. A., Moore, L. J., Privette, A. R., Schellenberg, M., Schuster, K. M., Tesoriero, R., Weinberg, J. A., & Stein, D. M. (2025). Western Trauma Association critical decisions in trauma: Damage-control resuscitation. Journal of Trauma and Acute Care Surgery, 98(2), 271–276. https://doi.org/10.1097/TA.0000000000004466
Evaniew, N., Davies, B., Farahbakhsh, F., Fehlings, M. G., Ganau, M., Graves, D., Guest, J. D., Korupolu, R., Martin, A. R., McKenna, S. L., Tetreault, L. A., Vedantam, A., Brodt, E. D., Skelly, A. C., & Kwon, B. K. (2024). Interventions to Optimize Spinal Cord Perfusion in Patients With Acute Traumatic Spinal Cord Injury: An Updated Systematic Review. Global Spine Journal, 14(3_suppl), 58S-79S. https://doi.org/10.1177/21925682231218737
Hasler, R. M., Nüesch, E., Jüni, P., Bouamra, O., Exadaktylos, A. K., & Lecky, F. (2012). Systolic blood pressure below 110mmHg is associated with increased mortality in penetrating major trauma patients: Multicentre cohort study. Resuscitation, 83(4), 476–481. https://doi.org/10.1016/j.resuscitation.2011.10.018
LaGrone, L. N., Stein, D., Cribari, C., Kaups, K., Harris, C., Miller, A. N., Smith, B., Dutton, R., Bulger, E., & Napolitano, L. M. (2024). American Association for the Surgery of Trauma/American College of Surgeons Committee on Trauma: Clinical protocol for damage-control resuscitation for the adult trauma patient. Journal of Trauma and Acute Care Surgery, 96(3), 510–520. https://doi.org/10.1097/TA.0000000000004088
LaRiccia, A. K., Sperwer, K., Lieber, M. L., & Spalding, M. C. (2024). Mean arterial pressure (MAP) augmentation in traumatic spinal cord injuries: Early hyperperfusion treatment influences neurologic outcomes. The Journal of Spinal Cord Medicine, 47(6), 918–925. https://doi.org/10.1080/10790268.2023.2223447
Lott, C., Karageorgos, V., Abelairas-Gomez, C., Alfonzo, A., Bierens, J., Cantellow, S., Debaty, G., Einav, S., Fischer, M., González-Salvado, V., Greif, R., Metelmann, B., Metelmann, C., Meyer, T., Paal, P., Peran, D., Scapigliati, A., Spartinou, A., Thies, K., … Deakin, C. D. (2025). European Resuscitation Council Guidelines 2025 Special Circumstances in Resuscitation. Resuscitation, 215. https://doi.org/10.1016/j.resuscitation.2025.110753
Martin, N., Kepler, C., Zubair, M., Sayadipour, A., Cohen, M., & Weinstein, M. (2015). Increased mean arterial pressure goals after spinal cord injury and functional outcome. Journal of Emergencies, Trauma, and Shock, 8(2), 94. https://doi.org/10.4103/0974-2700.155507
Morrison, C. A., Carrick, M. M., Norman, M. A., Scott, B. G., Welsh, F. J., Tsai, P., Liscum, K. R., Wall, M. J., & Mattox, K. L. (2011). Hypotensive Resuscitation Strategy Reduces Transfusion Requirements and Severe Postoperative Coagulopathy in Trauma Patients With Hemorrhagic Shock: Preliminary Results of a Randomized Controlled Trial. Journal of Trauma: Injury, Infection & Critical Care, 70(3), 652–663. https://doi.org/10.1097/TA.0b013e31820e77ea
Murray, G. D., Butcher, I., McHugh, G. S., Lu, J., Mushkudiani, N. A., Maas, A. I. R., Marmarou, A., & Steyerberg, E. W. (2007). Multivariable Prognostic Analysis in Traumatic Brain Injury: Results from The IMPACT Study. Journal of Neurotrauma, 24(2), 329–337. https://doi.org/10.1089/neu.2006.0035
Picetti, E., Catena, F., Abu-Zidan, F., Ansaloni, L., Armonda, R. A., Bala, M., Balogh, Z. J., Bertuccio, A., Biffl, W. L., Bouzat, P., Buki, A., Cerasti, D., Chesnut, R. M., Citerio, G., Coccolini, F., Coimbra, R., Coniglio, C., Fainardi, E., Gupta, D., … Robba, C. (2023). Correction: Early management of isolated severe traumatic brain injury patients in a hospital without neurosurgical capabilities: a consensus and clinical recommendations of the World Society of Emergency Surgery (WSES). World Journal of Emergency Surgery, 18(1), 29. https://doi.org/10.1186/s13017-023-00489-5
Ploumis, A., Yadlapalli, N., Fehlings, M. G., Kwon, B. K., & Vaccaro, A. R. (2010). A systematic review of the evidence supporting a role for vasopressor support in acute SCI. Spinal Cord, 48(5), 356–362. https://doi.org/10.1038/sc.2009.150
Rossaint, R., Afshari, A., Bouillon, B., Cerny, V., Cimpoesu, D., Curry, N., Duranteau, J., Filipescu, D., Grottke, O., Grønlykke, L., Harrois, A., Hunt, B. J., Kaserer, A., Komadina, R., Madsen, M. H., Maegele, M., Mora, L., Riddez, L., Romero, C. S., … Spahn, D. R. (2023). The European guideline on management of major bleeding and coagulopathy following trauma: sixth edition. Critical Care, 27(1), 80. https://doi.org/10.1186/s13054-023-04327-7
Sabit, B., Zeiler, F. A., & Berrington, N. (2018). The Impact of Mean Arterial Pressure on Functional Outcome Post Trauma-Related Acute Spinal Cord Injury: A Scoping Systematic Review of the Human Literature. Journal of Intensive Care Medicine, 33(1), 3–15. https://doi.org/10.1177/0885066616672643
Safiejko, K., Smereka, J., Filipiak, K. J., Szarpak, A., Dabrowski, M., Ladny, J. R., Jaguszewski, M. J., & Szarpak, L. (2022). Effectiveness and safety of hypotension fluid resuscitation in traumatic hemorrhagic shock: A systematic review and meta-analysis of randomized controlled trials. Cardiology Journal, 29(3), 463–471. https://doi.org/10.5603/CJ.a2020.0096
Sajdeya, R., Yanez, N. D., Kampp, M., Goodman, M. D., Zonies, D., Togioka, B., Nunn, A., Winfield, R. D., Martin, N. D., Kohli, A., Huynh, T. T., Okonkwo, D. O., Poblete, R. A., Gilmore, E. J., Chesnut, R. M., Bunnell, A. E., Ohnuma, T., Hashemaghaie, M., & Treggiari, M. M. (2025). Early Blood Pressure Targets in Acute Spinal Cord Injury. JAMA Network Open, 8(9), e2525364. https://doi.org/10.1001/jamanetworkopen.2025.25364
Schroeder, G., Alexander, V., & Welch, W. (2022). ACS BEST PRACTICES GUIDELINES SPINE INJURY.
Squair, J. W., Bélanger, L. M., Tsang, A., Ritchie, L., Mac-Thiong, J.-M., Parent, S., Christie, S., Bailey, C., Dhall, S., Street, J., Ailon, T., Paquette, S., Dea, N., Fisher, C. G., Dvorak, M. F., West, C. R., & Kwon, B. K. (2017). Spinal cord perfusion pressure predicts neurologic recovery in acute spinal cord injury. Neurology, 89(16), 1660–1667. https://doi.org/10.1212/WNL.0000000000004519
Tanvir, A., Rizk, A. A., Wang, W., Alsagga, H., Shakil, H., Le, H., Mondal, P., Zeiler, F. A., & Chowdhury, T. (2025). Effect of blood pressure threshold on adverse outcomes in patients with acute spinal cord injury: a systematic review and meta-analysis. Critical Care, 29(1), 308. https://doi.org/10.1186/s13054-025-05531-3
Tran, A., Yates, J., Lau, A., Lampron, J., & Matar, M. (2018). Permissive hypotension versus conventional resuscitation strategies in adult trauma patients with hemorrhagic shock: A systematic review and meta-analysis of randomized controlled trials. Journal of Trauma and Acute Care Surgery, 84(5), 802–808. https://doi.org/10.1097/TA.0000000000001816
Vale, F. L., Burns, J., Jackson, A. B., & Hadley, M. N. (1997). Combined medical and surgical treatment after acute spinal cord injury: results of a prospective pilot study to assess the merits of aggressive medical resuscitation and blood pressure management. Journal of Neurosurgery, 87(2), 239–246. https://doi.org/10.3171/jns.1997.87.2.0239
Walters, B. C., Hadley, M. N., Hurlbert, R. J., Aarabi, B., Dhall, S. S., Gelb, D. E., Harrigan, M. R., Rozelle, C. J., Ryken, T. C., & Theodore, N. (2013). Guidelines for the Management of Acute Cervical Spine and Spinal Cord Injuries. Neurosurgery, 60(Supplement 1), 82–91. https://doi.org/10.1227/01.neu.0000430319.32247.7f
Perhaps a typo? “A normal blood pressure of 120/80 corresponds to a MAP of approximately 85” Isn’t that around 95? thanks for the great synthesis!