
In the ED we are certainly no stranger to seeing alcohol use disorder, its complications, and alcohol withdrawal. Every day in Canada, there are approximately 269 hospitalizations directly attributable to alcohol. This is more than admissions for acute MI. As the primary entry point for admissions to hospital, in the ED this is something that we see and manage on a daily basis.
Alcohol use disorder is the most prevalent substance use disorder both in Canada and in the World. With more than 20% of people drinking regularly above Canada’s low risk drinking guidelines at some point in their lives.
Framing the Conversation
In this post, I hope to cover the following:
- Briefly review the pathophysiology of alcohol withdrawal syndrome (AWS)
- Review the pharmacology of both benzodiazepines and phenobarbital as they relate to AWS management
- Discuss the use of phenobarbital in the following cases:
- Benzodiazepine-resistant AWS
- As an adjunct to benzodiazepines in moderate-to-severe AWS
- And as monotherapy in AWS
- Review the prescription of anti-craving medications from the ED
*Disclaimers*
- We are not going to review CIWA or other symptom triggered scales, nor will we be reviewing the evidence for the use of benzodiazepines as first line for alcohol withdrawal.
- We will also not be reviewing outpatient benzodiazepine tapers and the use of gabapentin for withdrawal management, though I would encourage everyone to review this in detail here.
- The use of phenobarbital for alcohol withdrawal is currently a very controversial topic in the world of addiction and emergency medicine. My conclusions may or may not be in line with what you have previously heard depending on what you’ve read and who you’ve talked to, and I think that’s OK. I do think we’ll see a lot more research on this topic in the near future, and I think it’s really great to see how many people are interested in improving care for what has historically been a stigmatized patient population.
Understanding the Physiology: Why Patients Escalate
At its core, alcohol withdrawal is a failure of balance. Chronic alcohol exposure enhances inhibitory tone through GABA and suppresses excitatory pathways through NMDA receptors. Over time, the brain adapts by downregulating inhibition and upregulating excitation.
When alcohol is abruptly removed, the system becomes unopposed, and what you are left with is a hyperexcitable brain, manifesting as: autonomic instability, tremor and agitation, seizures, and delirium.
Important points to highlight moving forward are that:
- While we see alcohol withdrawal all the time, and certainly we do see severe withdrawal as well, it’s not actually all that common. Most estimates are that only around 10-20% of ED visits for alcohol withdrawal are considered severe. Existing literature uses a variety of different definitions of severity, including CIWA cutoffs, other grading scales, physician gestalt, clinical symptoms, et cetera
- Secondly, the clinical course of alcohol withdrawal varies greatly among patients in terms of the symptoms they experience and severity, and progression through the stages is also highly variable
Below is a general timeline of symptoms seen in alcohol withdrawal for MOST patients:
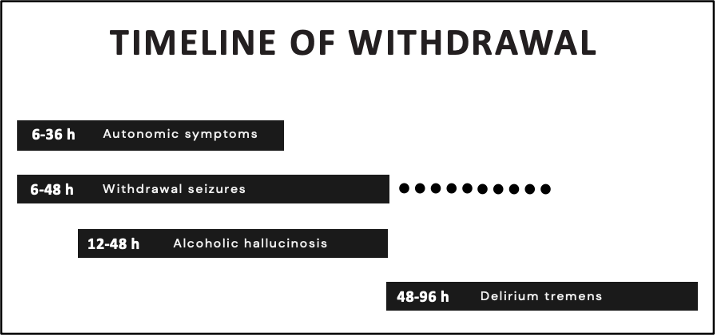
- Autonomic symptoms: typically begin within 6h, and include tremors, autonomic hyperactivity (but not instability), GI symptoms, et cetera. These symptoms can be extremely uncomfortable for patients, but are generally not life-threatening.
- Withdrawal seizures are seen in up to 10% of patients with alcohol withdrawal. These seizures are typically brief, generalized tonic-clonic seizures with short post-ictal periods, and status epilepticus is very rare.
- Hallucinations are seen in up to 25% of patients, and can be tactile, visual, or auditory. Patients with hallucinations maintain a clear sensorium and are not typically delirious. This is not the same thing as delirium tremens, nor is it a predictor of progression to DTs
- Delirium Tremens is the most serious and feared manifestation of AWS, typically occurring between 48-96h from the patient’s last drink. It is defined by a disturbed LOC, hyperactive delirium, as well as severe withdrawal symptoms including marked autonomic hyperactivity. Risk of death is 3-5%.
Gaba-ergic Options to Treat Withdrawal
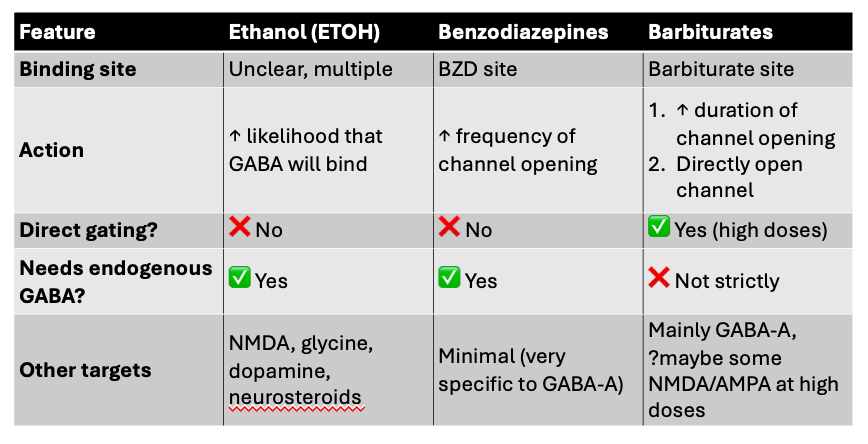
Benzodiazepines are the first line treatment for AWS. They act by binding the GABA receptor at a specific benzodiazepine site, acting as positive modulators of the GABA system. They increase the likelihood that endogenous GABA will bind, AND increase the frequency of channel opening in response to GABA. They require endogenous GABA to work and do not directly open the channel themselves.
- Diazepam is rapid onset, and rapidly crosses the BBB to exert its inhibitory effects. Diazepam also has active metabolites, which effectively prolong its clinical effects. Its half-life is around 20-50h
- In cases where we want to avoid the effects or accumulation of active metabolites, we use lorazepam. Specifically, we tend to use it in patients with severe or active liver disease, active respiratory disease, and our frail or elderly patients. The half-life of lorazepam is around 8-14h
Phenobarbital both prolongs the opening of the GABA channel to enhance inhibitory signaling, AND it can actually directly open the channel in the absence of any endogenous GABA.
- Phenobarbital also has global depressive effects on other excitable cell membranes such as the heart and smooth muscle.
- Phenobarbital may inhibit the glutamate system, which would of course make it the perfect mechanistic fit for the treatment of an alcohol withdrawal state. However these effects are a lot less clear, with some basic science studies showing that the actual doses needed to achieve any clinically significant inhibition of this system are more than 3x the therapeutic dose.
- The half-life of phenobarbital is around 80-120h
Utilizing Phenobarbital
1. Patient with Benzodiazepine Resistant AWS
-
- There is no agreed upon definition of benzo-resistance. Common definitions in the literature include the use of >200mg diazepam in a 3h time frame, or >40mg/dose with no improvement in symptoms. Clinically, this is when you are giving appropriate, high doses of benzodiazepines, on repeated occasions, and when you reassess your patient there has either been no effect, or they are worse.
- There is no agreed upon definition of benzo-resistance. Common definitions in the literature include the use of >200mg diazepam in a 3h time frame, or >40mg/dose with no improvement in symptoms. Clinically, this is when you are giving appropriate, high doses of benzodiazepines, on repeated occasions, and when you reassess your patient there has either been no effect, or they are worse.
-
- In these cases, the major proposed benefit of phenobarb is that it rapidly acts at the GABA receptor, with a different mechanism of action than benzodiazepines, and exerts its clinical effects over a very long period of time, all while not necessarily requiring endogenous GABA. It can prevent seizures while not necessarily requiring intubation and mechanical ventilation like propofol would. In fact, it can help to AVOID intubation in these rare situations.
-
- Phenobarbital is a generally well-accepted treatment option in these cases. This IS an indication for phenobarb in the addiction medicine world, and not really the main source of the controversy surrounding phenobarbital.
-
- Dosing: Dr. Jess Hann, an Emergency Medicine and Addictions Specialist in Vancouver recommends the following:
- If benzos have already been given, and are not effective:
- IV phenobarbital : 120-240mg boluses over 3-5 minutes, repeated every 30 minutes prn
- PO phenobarbital: 100-200mg PO, repeated after ~60 minutes prn
- If no benzos have been given yet (ex: your patient has a well-documented history of bzd-resistance)
- IV phenobarbital loading dose usually 5-7 (some sources 5-10) mg/kg (IBW) given over 30 minutes
- Reassess after loading dose complete to determine if top-up load required, then begin PRN dosing based on symptoms
- If benzos have already been given, and are not effective:
- Bottom line: this is an indication for the use of phenobarbital, and you are supported by the addiction medicine literature if you use it in these cases. However, keep in mind that your site’s ICU team may prefer to use other adjuncts or be less comfortable with this medication, and this patient’s ultimate disposition is likely to ICU.
- Dosing: Dr. Jess Hann, an Emergency Medicine and Addictions Specialist in Vancouver recommends the following:
2. As an Adjunct
-
- The biggest and most prominent review that has been done on this topic are the GRACE-4 guidelines, which were published last year and included several Canadian researchers. GRACE-4 specifically looked at the following question: in patients over the age of 18 who are receiving pharmacologic therapy for moderate to severe alcohol withdrawal in the ED. Does the use of adjunctive phenobarbital by any route, compared to benzodiazepines alone lead to improvement in outcomes?
- It concluded the following: in adult ED patients (over the age of 18), with moderate to severe alcohol withdrawal, who are being admitted to hospital, we suggest using phenobarbital in addition to benzodiazepines compared to using benzodiazepines alone
- However, GRACE-4 had several important weaknesses:
- Nearly all studies included used lorazepam if a specific benzodiazepine was studied. This is NOT our standard of care, as we prefer to use diazepam for its faster onset and longer duration of action.
- The safety data reported from the studies included was extremely heterogenous, with some not reporting on safety at all. The safety data that was reported was generally not comprehensive nor of particularly high quality.
- The studies included were extremely heterogenous, and authors state as a result of this they were unable to pool data for a meta-analysis. There was very wide variability in the patient populations – for example some included patients that were actually planned to be discharged, some were those who got admitted to a highly monitored setting, one study was exclusively looking at patients with concurrent opioid and alcohol withdrawal. There was also wide variety in the phenobarbital dosing strategies used, which is why GRACE-4 was unable to make any specific recommendations regarding this
- There was a large amount of indirect evidence, not specifically ED studies
- The biggest and most prominent review that has been done on this topic are the GRACE-4 guidelines, which were published last year and included several Canadian researchers. GRACE-4 specifically looked at the following question: in patients over the age of 18 who are receiving pharmacologic therapy for moderate to severe alcohol withdrawal in the ED. Does the use of adjunctive phenobarbital by any route, compared to benzodiazepines alone lead to improvement in outcomes?
-
- Bottom line: as an adjunct to benzos in moderate to severe alcohol withdrawal syndrome, I’m not convinced that that the evidence is there yet. I would be interested in seeing how phenobarbital adjunctive therapy holds up when compared to diazepam monotherapy, which is more in keeping with our standard of care. I would also want to see more robust safety data. I would be extremely concerned if a patient received a loading dose of Phenobarbital, and subsequently self-discharged.
3. As Monotherapy
-
- In 2019, the North Battleford Hospital in Saskatchewan implemented a phenobarbital monotherapy pathway as an option for AWS management, without modifying their existing benzodiazepine pathway. The order-set was rolled out informally, and the use of each pathway was left completely to the treating physician’s discretion
- In 2022 they published their observational findings that spanned 2019-2021 and included 183 visits in this QI study. Ultimately, they found that patients were 71.3% less likely to be hospitalized for alcohol withdrawal if they received phenobarbital as compared to diazepam.
- This study has quite a few limitations, including its QI design, small sample size of which only 26 patients were hospitalized, and only 8 patients left the ED AMA. They also DID NOT report any safety data.
- Dr. Brady Bouchard, an Emergency Medicine and Addictions Specialist, and the provincial EM addiction and vulnerable populations lead for the province of Saskatchewan, told me that in his experience with phenobarbital, he finds that they are admitting far fewer patients with AWS to hospital, and providers are far more comfortable with discharging these patients. He has had zero incidences of airway intervention within the safety data that he is currently working on collecting for publication.
- Currently, a large provincial retrospective study is ongoing, and he is working on developing a large prospective trial in the near future.
- Bottom line: again, I don’t think the evidence is there yet. I certainly love the idea of a medication that can be given in a load to control my patients’ symptoms, and to be able to discharge them safely to the community, but again I would need to see more robust safety data. I will certainly be watching what comes out of Saskatchewan in the years to come, and I wonder if the way we use phenobarbital now will be entirely different than the way that we use it in 10 years.
- In 2019, the North Battleford Hospital in Saskatchewan implemented a phenobarbital monotherapy pathway as an option for AWS management, without modifying their existing benzodiazepine pathway. The order-set was rolled out informally, and the use of each pathway was left completely to the treating physician’s discretion
Anti-Craving Medication
There are 2 main options when discussing anti-craving medications:
- Naltrexone – an opioid antagonist, so it blocks the release of endogenous opioids triggered by the consumption of ethanol. It decreases cravings, prevents relapse, and reduces bingeing.
-
- Contraindications: active opioid use and those with active or sequelae of hepatic dysfunction.
- Patients need to have their liver enzymes checked in a follow-up appointment
- It is NOT contraindicated in patients who continue to drink, and can technically be started in withdrawal, though more ideally started once GI and other severe symptoms have abated.
- Common side effects: headache, nausea, vomiting, anorexia, abdominal pain, insomnia, and dizziness.
- Dosing: 50mg daily, though I recommend starting at 25mg daily for a few days then increasing to 50mg in order to decrease side effects
- LU code: 532
- Contraindications: active opioid use and those with active or sequelae of hepatic dysfunction.
- Acamprosate – an NMDA receptor antagonist, glutamate ‘stabilizer’, GABA receptor ‘modulator’. It decreases cravings and reduces the discomfort of abstinence. It should be started after withdrawal is complete, and its efficacy has only been established specifically in individuals who have achieved and wish to maintain abstinence.
-
- Contraindications: CrCl <30, and renal dose adjustment is required
- Common side effects: diarrhea, abdominal pain, headache, somnolence
- Dosing:
- CrCl >50: 666mg TID
- CrCl 30-50: 333mg TID
- LU code: 531
- Patients started on anti-craving medications should have follow-up (Naltrexone requires LFTs be checked)
Summary
- Alcohol withdrawal syndrome (AWS) is common in the ED, but truly severe withdrawal represents a minority of cases. Severe complications include seizures and delirium tremens, the latter carrying a mortality risk of 3-5%.
- Benzodiazepines remain the first-line treatment for AWS. Diazepam is generally preferred due to its rapid onset and long duration, while lorazepam may be favoured in patients with liver disease, respiratory compromise, or frailty.
- Phenobarbital has a unique pharmacologic profile because it can directly activate the GABA receptor, even in the absence of endogenous GABA. This may explain its utility in benzodiazepine-resistant withdrawal.
- The strongest current indication for phenobarbital is benzodiazepine-resistant AWS. In these patients, phenobarbital is widely accepted in addiction medicine and may help prevent escalation to intubation and ICU-level sedation.
- Current enthusiasm for phenobarbital is growing, but caution is warranted. Questions remain regarding optimal dosing, patient selection, discharge safety, and comparison to aggressive diazepam monotherapy.
- For Benzodizapine-resistant alcohol withdrawal:
- IV Phenobarbital 120-240 mg IV over 3-5 minutes, repeated every 30 minutes prn based on reassessment
- PO Phenobarbital 100-200 mg po repeated after approximately 60 minutes prn
- For patients with a known history of benzodiazepine-resistant withdrawal where phenobarbital is being used early:
- Loading dose: 5-7 mg/kg (IBW) over 30 minutes
- Reassess after completion of the loading dose to determine if additional loading or PRN dosing is required.
- For Benzodizapine-resistant alcohol withdrawal:
- Anti-craving medications should be part of ED care discussions. Naltrexone and acamprosate are evidence-based options that can reduce relapse and support long-term recovery when paired with appropriate follow-up.
- Alcohol use disorder is a chronic medical disease, not a moral failing. Emergency physicians are uniquely positioned not only to manage acute withdrawal safely, but also to initiate long-term recovery-oriented care.
References
- Borgundvaag B, Bellolio F, Miles I, Schwarz ES, Sharif S, Su MK, et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE-4): Alcohol use disorder and cannabinoid hyperemesis syndrome management in the emergency department. Acad Emerg Med. 2024;31(5):425-455.
- Canver BR, Newman RK, Gomez AE. Alcohol Withdrawal Syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
- Cheng XJC, Chung J, Yoo N, Akerman M, Bender M, Chan K, et al. Impact of phenobarbital when used in combination with benzodiazepines for the treatment of alcohol withdrawal syndrome: A retrospective analysis. Am J Emerg Med. 2025;92:79-84.
- Chowdhury MDS, Rothenberg R, Hoffman RS. The Effect of Phenobarbital on Excitatory Transmission in Alcohol Withdrawal Syndrome. Ann Emerg Med. 2024;84(3):327-328.
- Goodberlet M, Dube K, Kovacevic M, Szumita P, DeGrado J. Evaluation of a Phenobarbital-Based Protocol for Severe Alcohol Withdrawal in Critically Ill Patients. Hosp Pharm. 2021;56(5):550-559.
- Gottlieb M, Chien N, Long B. Managing Alcohol Withdrawal Syndrome. Ann Emerg Med. 2024;84(1):29-39.
- Grover S, Ghosh A. Delirium Tremens: Assessment and Management. J Clin Exp Hepatol. 2018;8(4):460-470.
- Hammond DA, Rowe JM, Wong A, Wiley TL, Lee KC, Kane-Gill SL. Patient Outcomes Associated With Phenobarbital Use With or Without Benzodiazepines for Alcohol Withdrawal Syndrome: A Systematic Review. Hosp Pharm. 2017;52(9):607-616.
- Hawa F, Gilbert L, Gilbert B, Hereford V, Hawa A, Al Hillan A, et al. Phenobarbital Versus Lorazepam for Management of Alcohol Withdrawal Syndrome: A Retrospective Cohort Study. Cureus. 2021;13(2):e13282.
- Hendey GW, Dery RA, Barnes RL, Snowden B, Mentler P. A prospective, randomized trial of phenobarbital versus benzodiazepines for acute alcohol withdrawal. Am J Emerg Med. 2011;29(4):382-385.
- Ibarra F. Single dose phenobarbital in addition to symptom-triggered lorazepam in alcohol withdrawal. Am J Emerg Med. 2020;38(2):178-181.
- Lebin JA, Mudan A, Murphy CE, Wang RC, Smollin CG. Return Encounters in Emergency Department Patients Treated with Phenobarbital Versus Benzodiazepines for Alcohol Withdrawal. J Med Toxicol. 2022;18(1):4-10.
- Lee CM, Dillon DG, Tahir PM, Murphy CE. Phenobarbital Treatment of Alcohol Withdrawal in the Emergency Department. Acad Emerg Med. 2024;31(5):515-524.
- Lewis CB, Patel P, Adams N. Phenobarbital. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
- Long B, Keim SM, Gottlieb M, Rathlev N. Is Phenobarbital an Effective Treatment for Alcohol Withdrawal Syndrome? J Emerg Med. 2024;67(5):e494-e503.
- Mahmoud S, Anderson E, Vosooghi A, Herring AA. Treatment of opioid and alcohol withdrawal in a cohort of emergency department patients. Am J Emerg Med. 2021;43:17-20.
- Nelson AC, Kehoe J, Sankoff J, Mintzer D, Taub J, Kaucher KA. Benzodiazepines vs barbiturates for alcohol withdrawal: Analysis of three different treatment protocols. Am J Emerg Med. 2019;37(4):733-736.
- Pistore A, Penney S, Bryce R, Meyer C, Bouchard B. A retrospective evaluation of phenobarbital versus benzodiazepines for treatment of alcohol withdrawal in a regional Canadian emergency department. Alcohol. 2022;102:59-65.
- Pourmand A, AlRemeithi R, Kartiko S, Bronstein D, Tran QK. Evaluation of phenobarbital-based approach in treating patients with alcohol withdrawal syndrome: A systematic review and meta-analysis. Am J Emerg Med. 2023;69:65-75.
- Punia K, Scott W, Manuja K, Campbell K, Balodis IM, MacKillop J. SAEM GRACE: Phenobarbital for alcohol withdrawal management in the emergency department: A systematic review of direct evidence. Acad Emerg Med. 2024;31(5):481-492.
