

There are few phrases in emergency medicine that generate as much discomfort as hearing, “Remember that patient you saw yesterday? They’re back.” Most of us immediately retrace the encounter in our minds, wondering whether something was missed or whether we should have managed things differently. That reaction is understandable because return visits can occasionally uncover important safety issues. However, many bouncebacks are not diagnostic failures at all. Some reflect expected disease progression, barriers to follow-up, uncertainty, or the reality that emergency physicians often assess patients at only a single point in an evolving illness. The challenge is not simply identifying return visits, but separating meaningful signal from noise.
Why Return Visits Matter
Emergency department return visits sit at the intersection of patient safety, clinician feedback, and health-system strain, but they do not represent a single clinical entity. A patient may return because of natural disease progression, persistent symptoms, uncertainty, lack of timely outpatient care, social vulnerability, medication effects, scheduled follow-up, diagnostic error, therapeutic error, or some combination of these factors. That heterogeneity explains why revisit metrics have remained both attractive and frustrating. They clearly identify a population worthy of attention, but the broad numerator bundles together appropriate returns, unavoidable returns, and genuinely preventable adverse events.
The literature therefore supports a more precise framing. Calder et al. prospectively evaluated nearly 13,000 ED visits and found that roughly 7% of discharged patients had a return visit within 7 days, whereas Ontario’s later programmatic experience showed that only about 1% of visits fell into the much narrower 72-hour return-with-admission category that is considerably more useful for quality review.
In Calder’s work, passive voluntary reporting did not identify useful triggers for adverse events. In contrast, an electronic trigger based on 72-hour all-cause return visits with admission yielded a positive predictive value of 12% for adverse events, meaning that reviewing approximately eight flagged cases identified one event truly related to the initial ED care.
That is the fundamental signal-versus-noise lesson that underpins the Ontario approach. The value of revisit review lies less in the crude revisit rate itself and more in selecting the subgroup most likely to yield meaningful learning.
Why Crude Return Visits are a Poor Physician Quality Metric
The broad revisit rate has face validity, but it performs poorly as a report card for individual emergency physicians. A crude 48-hour, 72-hour, or 7-day revisit rate combines related and unrelated complaints, scheduled and unscheduled returns, same-site and cross-site revisits, and visits driven by patient or system factors that are often largely outside the control of the index clinician. The literature repeatedly cautions against collapsing all of these phenomena into a single quality metric.
Pham et al. showed that 72-hour returns in a national US cohort were not clearly sicker than non-return patients and did not consume meaningfully greater resources, undermining the assumption that a revisit automatically reflects unsafe care. Similarly, single-site dashboards systematically undercount revisits because a substantial proportion of patients return to a different ED.
The more defensible use of revisit data is therefore as a trigger for structured chart review and case finding rather than as a blunt performance measure. This distinction is not merely semantic. If systems treat return visits as punitive scores, clinicians will predictably respond with defensive testing or defensive admission. If systems instead use return visits to identify high-yield cases for audit, they become a practical tool for improving diagnostic safety and quality of care.
Ontario’s Return Visit Quality Program
Ontario’s Emergency Department Return Visit Quality Program (RVQP) operationalized this narrower, case-finding approach at scale. Beginning in 2016, the province’s highest-volume EDs were required to review selected 72-hour all-cause return visits with admission and all 7-day sentinel return visits with admission for paired high-risk presentations and diagnoses, including acute myocardial infarction after chest pain or shortness of breath, subarachnoid hemorrhage after headache or sinusitis, and pediatric sepsis after fever.
The logic was straightforward. Admission on the return visit enriches the case mix for clinically meaningful deterioration, while the sentinel diagnoses further enrich the population for time-sensitive conditions where delayed diagnosis can carry substantial harm.
During the first three years of the program, 86 participating Ontario EDs recorded 13,559,664 visits. They identified 125,698 72-hour all-cause return visits with admission (0.93% of all visits) and 847 7-day sentinel return visits with admission (0.0062% of all visits). Sites completed 12,852 detailed audits and identified 3,010 adverse events or quality issues, for an overall yield of 23.4%.
Importantly, the yield differed substantially across the two program streams. Approximately 21.9% of audited 72-hour all-cause cases and 45.1% of 7-day sentinel cases contained an adverse event or quality issue.
Those numbers are scientifically and educationally important. They show that most return visits with admission still do not reflect poor initial care, but they also demonstrate that a carefully designed trigger can identify a subgroup with enough signal to support meaningful departmental learning.
Equally important, the RVQP was not designed to drive down crude return-visit rates. Ontario’s guidance explicitly warns against using revisit metrics as blunt performance targets because doing so creates predictable unintended consequences, including unnecessary index admissions, over-investigation, greater crowding, and increased low-value resource use.
The program is better understood as an audit infrastructure for local quality improvement. Its purpose is to identify recurring patterns, themes, and system vulnerabilities that can subsequently be addressed through pathway revision, education, feedback, communication changes, or process redesign.
In that sense, the RVQP functions less as a scorecard and more as a surveillance-and-learning platform.
What Ontario Audits Find
One of the program’s major contributions is its thematic classification of recurrent quality issues. Chartier et al. identified 11 recurring themes that cluster into three broad domains.
The first is patient characteristics, particularly patient risk profile and elder care. These themes capture patients with high baseline complexity, including frailty, multimorbidity, cognitive impairment, limited supports, recurrent ED use, atypical presentations, and vulnerability to deterioration despite reasonable initial management.
The second domain is ED team actions and processes, including physician cognitive lapses, documentation deficiencies, communication and handover problems, radiology issues, failure to account for abnormal vital signs, and problems involving high-risk medications or drug interactions. This category contains many of the highest-yield physician-level opportunities for improvement, particularly around anchoring, premature closure, reassessment discipline, and making discharge reasoning explicit.
The third domain involves system issues, including discharge planning and community follow-up, patients who leave against medical advice or without being seen, and limited access to imaging or other diagnostic resources.
The value of this framework is that it helps avoid simplistic hindsight judgments. A return visit can simultaneously be influenced by patient-level risk, team-level decision making, and system-level constraints. The audit question therefore becomes not merely whether the patient returned, but why they returned and whether a modifiable safety or quality issue was present at the time of the index discharge.

What Patients Say About Why They Come Back
The most clinically useful counterweight to physician-centered interpretations of return visits comes from the patient-perspective literature. In Return Visits to the Emergency Department: The Patient Perspective, Rising et al. interviewed 60 adults who had an unscheduled return to the ED within 9 days of discharge.
Most patients did not describe the index encounter as obviously negligent or dismissive. Instead, returns were commonly driven by persistent or worsening symptoms, fear, uncertainty, lack of explanation regarding the cause of symptoms, difficulty accessing timely outpatient follow-up, medication concerns, and the belief that the ED remained the fastest or only place to obtain answers.
That finding matters because it reframes a substantial proportion of return visits as failures of certainty, communication, or access rather than failures of technical care alone. A patient may receive a clinically reasonable workup and still leave frightened, unconvinced, or unclear about what to expect next.
This is where the bedside implications become practical. Reassurance cannot simply consist of telling a patient that the tests were normal and discharge is appropriate. It requires explicitly naming the working diagnosis, or acknowledging when a definitive diagnosis is not yet available; explaining which dangerous diagnoses were considered and why they are less likely based on the current information; clarifying the expected clinical trajectory; and providing symptom-based return precautions alongside a concrete follow-up and backup plan.
In other words, patient experience is not separate from quality in the return-visit literature. Persistent uncertainty, poor understanding, and inability to access follow-up become part of the mechanism by which otherwise reasonable index encounters convert into repeat ED use.
The Double-Edged Sword: Unsafe Discharge vs Unnecessary Admission
Any serious discussion of bouncebacks has to confront the opposing hazard of trying to eliminate return visits by admitting more patients. The evidence reviewed in this presentation strongly argues against that reflex.
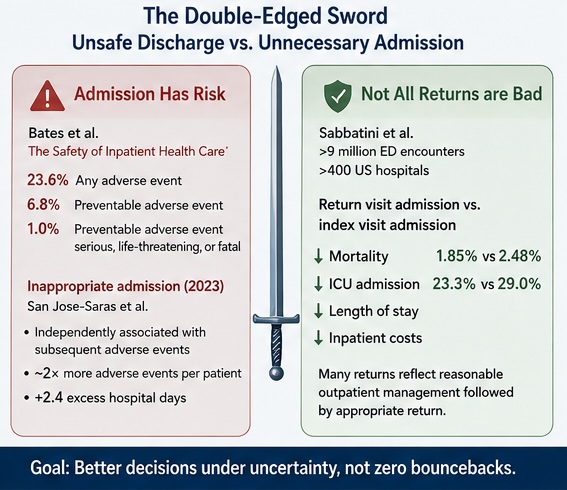
In The Safety of Inpatient Health Care, Bates et al. reported that 23.6% of hospitalized patients experienced at least one adverse event, 6.8% experienced a preventable adverse event, and 1.0% experienced a preventable adverse event rated as serious, life-threatening, or fatal. Admission, therefore, is not a neutral alternative to discharge. It is an intervention with measurable risk.
That argument is strengthened by later work examining inappropriate hospitalization. In a 2023 study evaluating inappropriate hospital admission as a risk factor for subsequent adverse events, San Jose-Saras and colleagues found that inappropriate admission was independently associated with subsequent adverse events, roughly doubled the mean number of adverse events per patient, and added an average of 2.4 excess hospital days.
The practical lesson is not that admission is inherently bad. Rather, admission carries its own morbidity, and indiscriminate admission to suppress revisit numbers is not a patient-safety strategy.
The most provocative evidence in this area comes from Sabbatini et al., who examined more than 9 million ED encounters across over 400 US hospitals. If return admission were simply a marker of unsafe discharge, one would expect patients admitted on a return visit to experience worse in-hospital outcomes than comparable patients admitted during the index visit. Instead, the opposite pattern emerged.
Patients discharged from the index ED visit and later admitted on a return visit had lower in-hospital mortality (1.85% vs 2.48%), lower ICU admission rates (23.3% vs 29.0%), shorter lengths of stay, and lower inpatient costs than patients admitted during the index visit. By contrast, patients readmitted after a hospital discharge had worse outcomes than those admitted during the index ED encounter.
These findings do not prove that every initial discharge was correct, nor do they excuse missed diagnoses. What they do suggest is that many return admissions represent a reasonable period of outpatient management followed by clinically appropriate return when an illness declares itself or fails initial therapy.
That is why the central task in emergency medicine is not to avoid every return visit, but rather to discharge well and admit when the prospective risk-benefit balance truly favours hospitalization.
What Discharge Actually Means in Emergency Medicine
A scientifically defensible way to frame discharge is as a risk-managed decision under uncertainty. The ED clinician evaluates an undifferentiated patient at a single point in time, rules out or lowers the probability of immediately dangerous conditions to an acceptable threshold, initiates treatment where appropriate, reassesses the patient’s response, and determines whether ongoing in-hospital evaluation is more likely to help than harm.
Discharge does not mean that nothing is wrong. It means that, based on the information currently available, admission is not clearly indicated and a monitored outpatient course is reasonable.
That framing is essential because many diagnoses evolve over hours to days. Some patients will deteriorate, develop new findings, or re-present with clearer manifestations of disease despite a reasonable initial assessment. Viewed prospectively rather than retrospectively, that phenomenon is inherent to emergency medicine rather than evidence of failure.
Implications for ED Practice
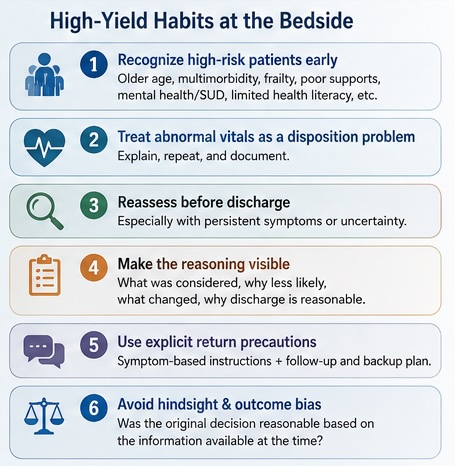
The Ontario and broader revisit literature points toward several high-yield clinical habits.
- First, recognize high-risk patients before disposition, including older adults, frail patients, those with multimorbidity, heart failure, renal disease, psychiatric or substance-use comorbidity, limited health literacy, language barriers, poor home supports, or unreliable follow-up.
- Second, treat abnormal vital signs as a disposition problem until they have been explained, repeated, and documented.
- Third, build in a reassessment pause before discharge, particularly in patients with persistent pain, ongoing diagnostic uncertainty, or discordance between the history, examination, and test results.
- Fourth, make the clinical reasoning visible in the chart: what dangerous diagnoses were considered, why they were considered less likely, what changed after treatment or observation, and why discharge remained reasonable despite residual uncertainty.
- Fifth, use explicit symptom-based return precautions rather than generic instructions to “return if worse.”
- Finally, when seeing the patient on a return visit, avoid hindsight bias and outcome bias. The second physician has more information than the first. The audit question should be whether the original decision was reasonable based on the information available at that time, rather than whether the final diagnosis would have seemed obvious in retrospect.
The literature also suggests that interventions aimed at globally reducing revisits have produced mixed results. Generic discharge education, routine phone calls, and other broad interventions often demonstrate limited impact on meaningful downstream outcomes. More targeted interventions appear more promising in selected populations, including older adults with falls, frequent users with complex psychosocial needs, and patients receiving pharmacist-led medication support.
This aligns closely with the philosophy behind the Ontario RVQP: broad revisit suppression is the wrong target, whereas targeted identification of modifiable quality problems is the better one.
Implications for Departmental Quality Improvement
For departments, the major lesson is that return visits are most useful when they are aggregated into themes rather than weaponized as individual scorecards. A structured return-visit review process should classify cases into expected disease progression, potentially preventable return, probable adverse event or quality issue, and indeterminate return.
Cases can then be coded according to the same domains emphasized by Ontario: patient factors, ED team factors, and system or disposition factors. This structure allows departments to transform memorable individual bouncebacks into higher-reliability quality-improvement work.
Examples include revision of chest pain pathways, standardized ECG or troponin workflows, obstetric consultation pathways, callback systems for abnormal pending results, triage or LWBS mitigation strategies, and simple forcing functions around repeat vital signs before discharge.
Education remains valuable, but the highest-yield interventions often involve standardization, reminders, clearer policies, or automation rather than simply encouraging clinicians to be more careful.
Conclusions
The mature interpretation of ED return visits is neither complacent nor punitive. Return visits matter because they identify a subset of patients who experienced worsening illness, unresolved uncertainty, barriers to care, communication failures, or genuine adverse events. Yet the broad revisit rate remains too heterogeneous to serve as a fair measure of physician quality.
The Ontario RVQP provides a more useful model: focus on return visits with admission, enrich further with sentinel diagnoses, audit those cases in a structured way, and use the results to identify recurring clinical and systems themes.
The bedside response is not to eliminate return visits at all costs. Rather, it is to improve risk recognition, reassessment, communication, documentation, and follow-up planning while remaining honest that some return visits are expected and some admissions carry harm.
In emergency medicine, the real quality target is not zero bouncebacks. It is better decisions under uncertainty.
References
Calder L, Pozgay A, Riff S, et al. Adverse events in patients with return emergency department visits. BMJ Qual Saf. 2015;24:142-148.
Pham JC, Kirsch TD, Hill PM, et al. Seventy-two-hour returns may not be a good indicator of safety in the emergency department: a national study. Acad Emerg Med. 2011;18:390-397.
Chartier LB, Ovens H, Hayes E, et al. Improving Quality of Care Through a Mandatory Provincial Audit Program: Ontario’s Emergency Department Return Visit Quality Program. Ann Emerg Med. 2021;77:193-202.
Chartier LB, Jalali H, Seaton MB, et al. Qualitative evaluation of a mandatory provincial programme auditing emergency department return visits. BMJ Open. 2021;11:e044218.
Rising KL, Padrez KA, O’Brien M, Hollander JE, Carr BG, Shea JA. Return Visits to the Emergency Department: The Patient Perspective. Ann Emerg Med. 2015;65:377-386.e3.
Bates DW, Levine DM, Salmasian H, et al. The Safety of Inpatient Health Care. N Engl J Med. 2023;388:142-153.
San Jose-Saras D, Vicente-Guijarro J, Sousa P, et al. Inappropriate hospital admission as a risk factor for the subsequent development of adverse events. BMC Med. 2023;21:382.
Sabbatini AK, Kocher KE, Basu A, Hsia RY. In-Hospital Outcomes and Costs Among Patients Hospitalized During a Return Visit to the Emergency Department. JAMA. 2016;315:663-671.

Beautifully submitted!