
I’ve written about it previously – but, patient’s ‘bouncing back’ to the Emergency Department (ED) after discharge has always been perceived as a negative thing, but I think that this is an inadequate lens to view patient care. The patient returned to the ED? Good, they did what they were supposed to. There are many instances where a disease has not evolved to the point where it requires investigation – and constantly chasing unlikely diagnoses leads to worse patient care. In order to enhance the care of these bounceback patients, however, we need to first improve our charting on patients.
Emergency Medicine is an ever-evolving speciality, as many patients don’t have access to primary care (especially in the midst of a global pandemic) – so patients may be receiving all of their primary care through the ED or walk-in clinics. The prevalence of patients obtaining care in this fashion is certainly going up, and in conjunction with this, we see a bounceback rate of patients re-presenting to the ED within one week of discharge hovering around 25%.
Charting
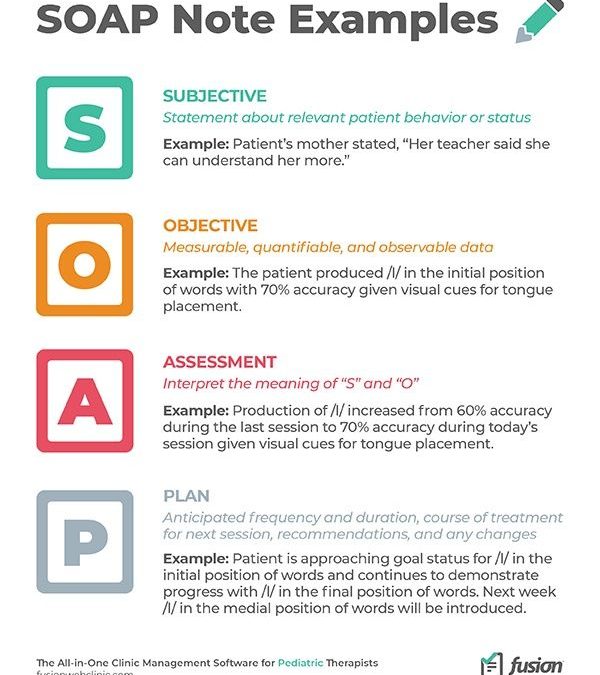
When it comes to documentation, we are often taught and trained to document with a medicolegal lens with a consistent structure (think: SOAP note), but, I think this does our colleagues and patients a disservice. When so many patients are re-presenting to the ED, and are being seen by multiple different providers, our documentation needs to be a more rational record of our thought process.
Let us use a case example to demonstrate the importance of this. You assess a young female with abdominal pain in whom you are concerned about appendicitis (lets assume you are not worried about any pelvic pathology). After doing an ultrasound, the report states; “unable to visualize appendix, but no ancillary findings of appendicitis seen.” I’m sure at some point, we’ve all encountered this.
Even though you can’t visualize the appendix, the probability of appendicitis in this case is quite low. You have three options; discharge with good RTED instructions, a CT scan, or call a surgeon.
Personally, I think the right answer is to employ shared decision making and involve the patient in your decision making process. It is clear here, if the patient is discharged, but returns with worsening pain – the next course of action would be a CT scan of the abdomen.
I would document this in this fashion:
U/S cannot visualize the appendix, but there are no ancillary findings of appendicitis and the patient’s pain has improved. We utilized shared decision making, and have decided to discharge the patient. Should her pain worsen, she should return to the ED for the consideration of further diagnostic testing.
Note: I did not promise the patient anything, but insinuate through my note that she needs a reassessment, because there is nothing worse than promising a test for somebody else. I documented my shared decision making and rationalized this in my chart.
Rethinking your Documentation
When you see a patient who has just bounced back to the ED – the impression written by the previous physician should contain the highest yield information in regards to what they thought, what their decision making was, and how to approach subsequent visits to the ED.
To do this, entails re-framing your thinking from a ‘medicolegal’ approach to charting, and instead chart from the perspective of ‘what is my colleague going to think when they read this if the patient bounces back’. An important consideration in this regard is justifying your thought process as to why you did or didn’t do anything in that particular case (as relevant). We are often very focused on documenting pertinent positives or negatives from a ‘medicolegal’ frame of mind, but a history written this way does little to capture a picture of clinical gestalt, and it is this gestalt that needs to be highlighted by physicians in their charting.
If your practice pattern skews to the left, i.e.: you tend to do fewer investigations, this method of documentation is especially important to justify why you are (or not) making specific decisions. For example – I never prescribe antibiotics or swab patients for strep throat (REBEL EM with a great summary on why). In my charting, I always document my rationale for why I am not doing what would be perceived as conventional standard of care, and at times will include references as to why I am doing things a particular way.
When doing Quality Assurance (QA) tasks – such as following up on blood cultures, swabs, etc. My interpretation of the results is incumbent upon understanding what the treating physician was thinking. If they saw a patient with isolated fever and ordered blood cultures, one of which returns positive – it is hard to appreciate what I am supposed to do with that information (is it a contaminant?). Now, if the physician had a high pre-test probability for bacteraemia, that patient should return to the ED for assessment. However, we don’t tend to chart this way, so this information is often not available so the default is to have the patient be reassessed. If I knew, however, that the pretest probability was quite low, I’d be more comfortable waiting for the second blood culture or ensuring follow up if the patient felt well at home.
When swabbing wounds or abscesses – QA is a nightmare, because it is often impossible to know what to do with these test results when the primary ordering physician isn’t following up on them, because the subsequent MD didn’t see the original lesion in the first place. Thus the importance of documenting your thinking so that others can make more informed decisions on subsequent interactions. The same thing holds true for an abdominal pain or delirium workup where a urine culture is sent, and returns positive after the patient has been discharged – but it is unclear if they truly had UTI symptoms. It can be hard to interpret what to do with this data without further guidance from the physician who actually saw the patient.
I think too often we fail to account for the patient’s next encounter with the healthcare system. A way to improve your patient care and to make you a better colleague – is in the impression component of your chart (this is far easier with electronic charting), document your rationale for your practice pattern on that patient, and any specific instructions that may be prudent for subsequent visits. This will enhance the quality of the care you provide as a result of improving your documentation, and your colleagues will appreciate it.
