

Undifferentiated abdominal pain; three words that give every Emergency Physician (EP) the shivers. Plain abdominal X-Ray’s (AXR) are a commonly ordered test in the Emergency Department (ED). Does the AXR play any role in the diagnostic workup of constipation? As CT and US are readily available in most EDs, what is the evidence for AXR in non-traumatic abdominal pain in the ED? With the emergence of ‘low dose CT’ (LDCT), how do we counsel patients regarding radiation dose? What are the critical diagnostic pitfalls that EPs must be aware of? Lets delve deeper into these imaging modalities.
Canadian Association of Radiologists (CAR) recommends AXR for geriatric and psychiatric patients where an accurate clinical history may not be feasible. 1
Role of AXR in the Diagnostic Workup of Constipation
- Validated scoring systems for diagnosing constipation have poor inter-rater reliability and are not practical for EPs to use.2
- A patient with serious underlying pathology is just as likely to have significant fecal loading on AXR as a patient with constipation. 3
- The reported sensitivity (61-80%) of AXR is poor to moderate. 4
Role of AXR in Non-traumatic Abdominal Pain
- A significant proportion of ED patients who have an AXR go on to receive further imaging (CT or US) – suggesting that EPs are using the AXR as a screening test or because of diagnostic uncertainty. 5-7
- The AXR has a minimal impact in correctly changing the EPs initial diagnosis following a H&P (the AXR only significantly improves the sensitivity in the diagnosis of SBO). 8
- For several disease processes (SBO, LBO, free air, volvulus, urolithiasis, body packers) the sensitivity and specificity are moderate at best. 9-15
- A major flaw in the existing evidence is that we do not know why EPs order AXRs.
Low dose CT scans in the ED
- LDCT has similar sensitivity and specificity as standard dose CT for appendicitis 16,17 and ureteral calculi. 18
- Diagnostic Pitfall: LDCT will pick up high-contrast disease (e.g. ureteral calculi), but may miss low-contrast disease (e.g. pancreatic tumour, organ metastases). 19
- Therefore, LDCT should be used in younger patients (age <50) in whom you have a high pretest probability that they have the diagnosis in question (e.g. appendicitis). It is NOT appropriate for older patients in whom you have a wide differential diagnosis.
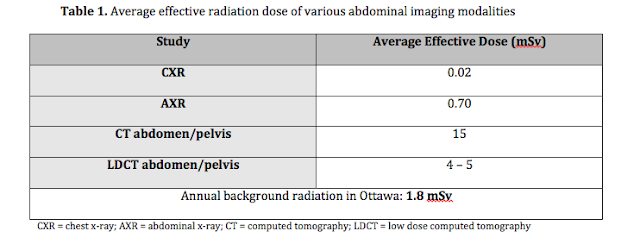
- The table below is useful when counseling patients regarding radiation doses for abdominal imaging. 20
Take Home Points
- AXR plays no role in the diagnostic workup of constipation
- Exception: geriatric or psychiatric patients in whom you cannot obtain an accurate history
- The presence of fecal loading on AXR does not rule out significant underlying pathology.
- AXR has a limited role for abdominal pain in the ED
- AXR may be useful in select cases (examples: patient with recurrent SBO, or known radiopaque ureteral calculi).
- Evidence suggests EPs may be ordering AXR’s as either a screening test, or because of diagnostic uncertainly.
- Major evidence gap: we do not know why EP’s actually order AXR’s.
- LDCT protocols have diagnostic pitfalls that EP’s should be aware of
- LDCT is appropriate for younger patients where there is a high pretest probability of a single specific diagnosis.
- LDCT may miss low-contrast disease processes (eg: organ metastases, pancreatic tumours).

Dr. Krishan Yadav is a 5th year Emergency Medicine resident at the University of Ottawa, with a special interest in Clinical Epidemiology.
Edited by Dr. Shahbaz Syed, 4th year Emergency Medicine resident, University of Ottawa
Edited by Dr. Shahbaz Syed, 4th year Emergency Medicine resident, University of Ottawa
References
1. CAR Referral Guidelines Secton G: Gastrointestinal System. 2012. (Accessed June 22, 2015, at http://www.car.ca/uploads/standards guidelines/car-referralguidelines-g-en_20120918.pdf.)
2. Moylan S, Armstrong J, Diaz-Saldano D, Saker M, Yerkes EB, Lindgren BW. Are abdominal x-rays a reliable way to assess for constipation? J Urol 2010;184:1692-8. doi: 10.016/j.juro.2010.05.054. Epub Aug 21.
3. Freedman SB, Thull-Freedman J, Manson D, et al. Pediatric abdominal radiograph use, constipation, and significant misdiagnoses. J Pediatr 2014;164:83-8.e2.
4. Berger MY, Tabbers Mm Fau – Kurver MJ, Kurver Mj Fau – Boluyt N, Boluyt N Fau – Benninga MA, Benninga MA. Value of abdominal radiography, colonic transit time, and rectal ultrasound scanning in the diagnosis of idiopathic constipation in children: a systematic review.
5. Jackson K, Taylor D, Judkins S. Emergency department abdominal x-rays have a poor diagnostic yield and their usefulness is questionable. Emerg Med J 2011;28:745-9. doi: 10.1136/emj.2010.094730. Epub 2010 Aug 15.
6. Kellow ZS, MacInnes M, Kurzencwyg D, et al. The role of abdominal radiography in the evaluation of the nontrauma emergency patient. Radiology 2008;248:887-93. doi: 10.1148/radiol.2483071772.
7. Sreedharan S, Fiorentino M, Sinha S. Plain abdominal radiography in acute abdominal pain–is it really necessary? Emerg 2014;21:597-603.
8. van Randen A, Lameris W, Luitse JS, et al. The role of plain radiographs in patients with acute abdominal pain at the ED. Am J Emerg Med 2011;29:582-9.e2.
9. Gans SL, Stoker J, Boermeester MA. Plain abdominal radiography in acute abdominal pain; past, present, and future. Int J Gen Med 2012;5:525-33.
10. Smith JE, Hall EJ. The use of plain abdominal x rays in the emergency department. Emerg Med J 2009;26:160-3. doi: 10.1136/emj.2008.059113.
11. Costello J, Townend W. Best evidence topic report. Abdominal radiography in “body packers”. Emerg Med J 2004;21:498.
12. Heidenreich A, Desgrandschamps F, Terrier F. Modern approach of diagnosis and management of acute flank pain: review of all imaging modalities. Eur Urol 2002;41:351-62.
13. MacKersie AB, Lane MJ, Gerhardt RT, et al. Nontraumatic acute abdominal pain: unenhanced helical CT compared with three-view acute abdominal series. Radiology 2005;237:114-22.
14. Ballantyne GH, Brandner MD, Beart RW, Jr., Ilstrup DM. Volvulus of the colon. Incidence and mortality. Ann Surg 1985;202:83-92.
15. Mutgi A, Williams JW, Nettleman M. Renal colic. Utility of the plain abdominal roentgenogram. Arch Intern Med 1991;151:1589-92.
16. Kim K, Kim YH, Kim SY, et al. Low-dose abdominal CT for evaluating suspected appendicitis. N Engl J Med 2012;366:1596-605. doi: 10.056/NEJMoa1110734.
17. Poletti PA, Platon A, De Perrot T, et al. Acute appendicitis: prospective evaluation of a diagnostic algorithm integrating ultrasound and low-dose CT to reduce the need of standard CT. Eur Radiol 2011;21:2558-66. doi: 10.1007/s00330-011-2212-5. Epub 2011 Jul 30.
18. Fracchia JA, Panagopoulos G, Katz RJ, Armenakas N, Sosa RE, DeCorato DR. Adequacy of low dose computed tomography in patients presenting with acute urinary colic. J Endourol 2012;26:1242-6. doi: 10.089/end.2012.0130. Epub 2012 Jun 27.
19.Fuentes-Orrego JM, Sahani DV. Low-dose CT in clinical diagnostics. Expert Opin Med Diagn 2013;7:501-10. doi: 10.1517/17530059.2013.826647. Epub 2013 Aug 13.
20. Mettler FA, Jr., Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology 2008;248:254-63. doi: 10.1148/radiol.2481071451.
·
·