
Platelets: too much, too little, don’t work. The approach to platelet emergencies is perhaps a little bit more complicated than that, so we attempt to breakdown a simplified approach to platelets in the Emergency Department (ED). Patients with various disease processes often present to the emergency department with critically low platelet counts.
When should we consider transfusing these patients prophylactically to prevent bleeding?
Some of these patients may require a procedure (such as lumbar puncture, central line or paracentesis) in the ED.
When is it safe to do these procedures? When should we consider transfusing during/prior to these procedures to prevent severe bleeding?
The following should provide a simple guide to some of these platelet-related dilemmas in the ED.
Prophylactic platelet transfusions:
1. Thrombocytopenia associated with chemotherapy:
- Most studies of spontaneous bleeding derived from hospitalized patients with hematologic malignancies receiving high dose chemotherapy.1
- These patients are at high risk of spontaneous bleeding due to vascular insults from chemotherapy
- Major bleeding (WHO grade 2 or higher):
- Increases at platelets < 20
- Increases dramatically at platelets < 10
- Increases with fever/infection
- Most guidelines and institutions recommend giving 1 adult dose of platelets for Plt < 10 or Plt < 20 with fever in hospitalized patients.3-5
- In the ED, consider transfusing platelets for any chemotherapy associated thrombocytopenic patient with platelets < 20.
- Factors to consider:
- Next follow up.
- Distance and practicality of followup appointments.
- Rate of platelet count decrease (if known).
- Available hospital resources: can they be seen next day in medical day unit to receive transfusion?
- Do they need to be admitted due to systemic illness, infection, etc.
- Factors to consider:
2. Thrombocytopenia associated with ideopathic thrombocytopenic purpura(ITP):
- Platelet transfusions are usually not indicated unless there is severe bleeding.
- Very low risk of spontaneous bleeding (< 1% / yr for age< 60).6
- Spontaneous bleeding increases at around Plt < 20.7
- Management (usually in conjunction with a hematologist):8,9
- Severe bleeding present:
- IVIG 1g/kg
- Methylprednisolone 1g IV
- Platelet transfusion
- Tranexamic acid 1g IV over 10 min then 1g IV over 8 hours
- Hematology consult
- Severe bleeding absent:
- Platelets < 30
- IVIG, steroids, immunosuppressive therapy or thrombopoietin receptor agonists, splenectomy
- Platelets > 30
- Observe, consider treatments above if minor bleeding uncontrolled.
- Timely follow up.
- Platelets < 30
- Severe bleeding present:
 |
3. Thrombocytopenia associated with liver disease:
Patients with liver disease have many reasons to be hypo/hyper-coagulable, therefore, the balance of bleeding vs. clotting in these patients is unpredictable, and not reflective of coagulation studies.
Fortunately, in these patients Plt < 30 are uncommon (~5%) and Plt <20 are rare (<1%).11
Therefore, in the ED; only transfuse platelets for severe bleeding.
4. Other scenarios:
- Are platelet transfusions contraindicated in patients with TTP or HIT?
- No absolute contraindications to giving platelets.12-14
- One large retrospective database review suggests NNH = 75 (TTP) and NNH = 26 (HIT) for arterial thrombosis and no increased risk of VTE when platelets are given.15
- Therefore, must balance risk of severe bleeding vs thrombosis on an individual level.
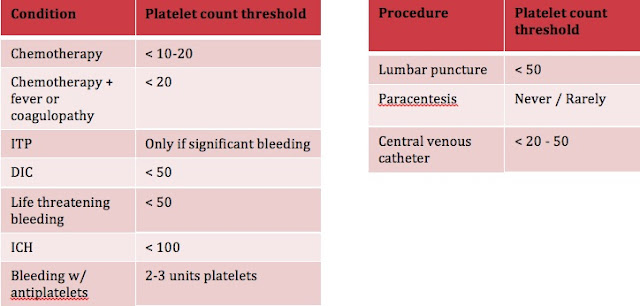
- Should strongly consider transfusing platelets in the following situations3:
- DIC or life threatening bleeding
- If patients platelets < 50
- ICH
- If patients platelets < 100
- Life threatening bleeding related to anti-platelet medications
- Transfuse 2-3 adult doses of paltelets
- DIC or life threatening bleeding
ED Procedures and Thrombocytopenia
1. Lumbar puncture
-
Thrombocytopenia
- Older case reports of spinal hematomas with Plt < 20.17,18
- Several studies demonstrate safety of LP at Plt < 20.19,20
- Safe threshold somewhere likely between Plt 20-50
- Most guidelines recommend platelet transfusion for Plt < 50 prior to LP as a safe margin (given potentially devastating consequence of spinal hematoma).3,4,5,21
Bottom line: In the ED, strongly consider using platelets < 50 as threshold for transfusion prior to lumbar puncture.
-
Antiplatelets
- ASA
- Several retrospective studies on patients receiving epidurals while on ASA.
- No reported spinal hematomas.22-24
- European Society of Anaesthesiology (ESA) and American Society of Regional Anesthesia (ASRA) guidelines suggest it is safe to proceed with LP.25,26
- Several retrospective studies on patients receiving epidurals while on ASA.
- Clopidogrel
- Surgical studies reliably demonstrate increased bleeding compared to ASA.
- 2 case reports of spinal hematomas in patients receiving epidural catheters while on Clopidogrel (but also confounded by receiving dose of Enoxaparin, Dalteparin).27,28
- ESA/ASRA guidelines suggest is unsafe to proceed with LP.22,23
- However, these recommendations are based on case reports, in which patients also received heparin – so these recommendations should be taken with a grain of salt. There is a potential risk, so case based considerations and shared decision making should be utilized.
- ASA
Bottom line: Lumbar puncture is safe in patients on ASA, but should require some careful consideration before being performed on patients on Clopidogrel.
2. Paracentesis
- Rate of severe bleeding exceedingly low despite INR ranges 0.9-8.7 and platelets as low as 19 in 2 large studies.29,30
- Severe bleeding usually caused by vessel puncture, not coagulopathy.
- As previously mentioned, the occurrence of platelets < 20 is rare in patients with liver disease.11
Bottom line: Platelet transfusions are rarely/never required prior to paracentesis.
3. Central Venous Catheters (CVCs)
- One study of 604 CVCs had a 32% bleed rate.31
- 96% grade 1, 4% grade 2 (prolonged compression).
- Demonstrated increased OR of bleeding only for platelets < 20.
- Another study reports 57 plasma exchange catheters for presumed TTP.32
- 29 for platelets < 30, 10 for platelets < 10, and 28 patients for platelets > 30.
- NO difference in minor bleeding (~30% for each group).
- No major bleeding requiring intervention.
- Most guidelines suggest transfusion for Plt < 50.3,5,21
- AABB 2015 guidelines recommend transfusion for plt < 20.4
Bottom line: In the ED, can probably use platelets < 20 as threshold for pre-procedure platelet transfusion for CVC insertion:
- Use ultrasound guidance
- Utilize a potentially compressible site (IJ, femoral).
- Experienced practitioner.
Take Home Points

Dr. Michael Ho is a 4th year Emergency Medicine resident at the University of Ottawa, with a special interest in medical education and resuscitation.
Edited by Dr. Shahbaz Syed, 4th year Emergency Medicine resident, University of Ottawa
References
1. Gaydos et al. The quantitative relation between platelet count and hemorrhage in patients with acute leukemia. NEJM 1962; 266:905
2. Gmur et al. safety of stringent prophylactic platelet transfusion policy for patients with acute leukemia. Lancet 1991; 338: 1223
3. BCSH. Guidelines for the use of platelet transfusions. Br J Haematol 2003; 122:10
4. Kaufman et al. Platelet transfusion: a clinical practice guideline from the AABB. Ann Int Med 2015; 162:205
5. Schiffer et al. Platelet Transfusion for Patients With Cancer: Clinical Practice Guidelines of the American Society of Clinical Oncology. J Clin Onc 2001; 19:1519
6. Cortelazzo et al. High risk of severe bleeding in aged patients with chronic idiopathic thrombocytopenic purpura. Blood 1991; 77:31
7. Vianelli et al. Long-term follow-up of idiopathic thrombocytopenic purpura in 310 patients. Haematologica 2001; 86:504
8. Cines et al. How I treat idiopathic thrombocytopenic purpura (ITP). Blood 2005; 106:2244
9. George JN. Management of patients with refractory immune thrombocytopenic purpura. J Thromb Haemost 2006; 4:1664
10. Dabbagh et al. Coagulopathy does not protect against venous thromboembolism in hospitalized patients with chronic liver disease. CHEST 2010; 137:1145
11. Grabau et al. Performance standards for therapeutic abdominal paracentesis. Hepatology 2004; 40:484
12. Scully et al. Guidelines on the diagnosis and management of thrombotic thrombocytopenic purpura and other thrombotic microangiopathies. Br J Haematol 2012; 156:323
13. Swisher et al. Clinical outcomes after platelet transfusions in patients with thrombotic thrombocytopenic purpura. Transfusion 2009; 49:873
14. Linkins et al. Treatment and Prevention of Heparin-Induced Thrombocytopenia. CHEST 2012; 141:e495S
15. Goel et al. Platelet transfusions in platelet consumptive disorders are associated with arterial thrombosis and in-hospital mortality. Blood 2015; 125:1470
16. Makris et al. Guideline on the management of bleeding in patients on antithrombotic agents. Br J Haematol 2012; 160:35
17. Edelson et al. Spinal subdural hematomas complicating lumbar puncture. Arch Neurol 1974; 31:134
18. Breuer et al. Radicular vessels are the most probable source of needle-induced blood in lumbar puncture: significance for the thrombocytopenic patient. Cancer 1982; 49:168
19. Vavricka et al. Safety of lumbar puncture for adults with acute leukemia and restrictive prophylactic platelet transfusion. Ann Hematol 2003; 82:570
20. Howard et al. Safety of lumbar puncture for children with acute lymphoblastic leukemia and thrombocytopenia. JAMA 2000; 284:2222
21. Patel et al. Consensus guidelines for periprocedural management of coagulation status and hemostasis risk in percutaneous image-guided interventions. J Vasc Interv Radiol 2012; 23:72
22. CLASP: a randomised trial of low-dose aspirin for the prevention and treatment of pre-eclampsia among 9364 pregnant women. CLASP (Collaborative Low-dose Aspirin Study in Pregnancy)
23. Horlocker et al. Preoperative antiplatelet therapy does not increase the risk of spinal hematoma associated with regional anesthesia. Anesth Analg 1995; 80:303
24. Horlocker et al. Risk assessment of hemorrhagic complications associated with nonsteroidal antiinflammatory medications in ambulatory pain clinic patients undergoing epidural steroid injection. Anesth Analg 2002; 95:1691
25. Gogarten et al. Regional anaesthesia and antithrombotic agents: recommendations of the European Society of Anaesthesiology. Eur J Anaesthesiol 2010; 27:999
26. Horlocker et al. Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy. American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med 2010; 35
27. Litz et al. Spinal epidural hematoma after spinal anesthesia in a patient treated with clopidogrel and enoxaparin. Anesthesiology 2004; 101:1467–1470.
28. Tam et al. Epidural haematoma after a combined spinal-epidural anaesthetic in a patient treated with clopidogrel and dalteparin. Br J Anaesth 2006; 96:262
29. Grabau et al. Performance standards for therapeutic abdominal paracentesis. Hepatology 2004; 40:484
30. Pache et al. Severe hemorrhage following abdominal paracentesis for ascites in patients with liver disease. Ailment Pharmacol Ther 2005; 21:525
31. Zeidler et al. Optimal preprocedural platelet transfusion threshold for central venous catheter insertions in patients with thrombocytopenia. Transfusion 2011; 51:2269
32. Duffy et al. Platelet transfusions and bleeding complications associated with plasma exchange catheter placement in patients with presumed thrombotic thrombocytopenic purpura. J Clin Apher 2013; 28:356