

For those of us who work in the Emergency Department, we are very well versed in migraine management. We see these patients frequently, and typically don’t hesitate to utilize our typical maxeran/toradol/fluids combo, as it is typically very effective. But what if your first, second and even third line treatments are ineffective?
Prior to considering neurology consultation for further management, perhaps we should consider one of the more controversial and novel treatments, such as propofol or magnesium. How about migraine preventative therapy, what’s the evidence behind dexamethasone in preventing recurrence? Here we seek to further delve into novel migraine therapies in the ED
Propofol
- The initial evidence for propofol for refractory migraines come from a single-centre, open-label trial at an outpatient headache clinic. Ultimately, they found a 95.4% average reduction in headache severity in patients receiving propofol 20-30 mg IV q3-5 minutes, with no adverse events or rescue analgesics required1.
- Since then, many studies have examined propofol utilization for refractory headaches, and have all had beneficial outcomes with minimal adverse events, but each of these studies were subject to various limitations and criticisms2,3.
- The most robust study, a randomized controlled trial comparing propofol to sumatriptan, demonstrated a significant improvement in VAS scores at 30 minutes, decreased migraine recurrence and less anti-emetic therapy use in the propofol group4 .

Bottom Line
- It appears that propofol is cheap, effective and safe. More research, however, is needed for formal recommendation.
- Propofol treatment is certainly more resource intensive, but given the current literature demonstrating effectiveness, it may be worth trying in the ED for patients with severe migraine, unresponsive to traditional therapy.
- The dosing varies slightly between studies, but generally consists of an initial bolus of 20-40 mg IV followed by additional 10-20 mg IV boluses every 3-5 minutes.
Magnesium
- Demirkaya and colleagues performed a randomized single-blinded placebo-controlled study in 2001, trying to determine the efficacy of magnesium (1g IV over 15 minutes) in treating acute migraines, and demonstrated:
- 30 minute response rate of 100% for MgSO4, compared to 6.7% in the placebo group
- 30 minute pain-free rate of 90% for MgSO4, compared to 0% for placebo. The 24 hour return rate for the magnesium group was 0%.
- This study was limited by its small sample size, process of randomization and short-term followup5,6.
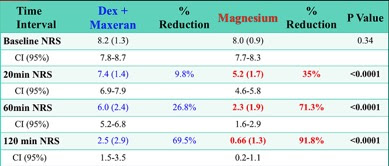
- Since then, a more robust double-blind RCT of 70 adult patients with migraine compared dexamethasone (8mg) with metoclopramide (10mg) to magnesium (1g). Pain scores were compared at 20, 60 and 120 minutes7.
- The study demonstrated that the magnesium group had a significant reduction in pain scores at 20, 60 and 120 minutes.
- This study helps to highlight that magnesium should strongly be considered as a therapy for refractory migraine.
- Although more methodologically sound than previous studies, limitations include a short follow-up period, convenience sampling and small sample size from a single centre.
Dexamethasone
- In 2008, Colman and colleagues published a large meta-analysis examining the efficacy of dexamethasone for preventing recurrence during acute severe migraine headache.
- This rather robust meta-analysis examined 7 RCT’s comparing steroids versus placebo, or other standard therapy. All 7 studies reported a lower recurrence of migraine in the dexamethasone group and ultimately, the review identified an ARR of 11.1% and NNT of 9 for the dexamethasone group8.
- A second meta-analysis was conducted in 2013, including the most recent literature and also demonstrated a significant benefit of steroids compared to placebo for preventing migraine recurrence at 24-72 hours9, with a NNT of 10.
- The only major difficulty interpreting this data was the variability used in steroid route and dosing.
- That being said, it is clear that steroids do have a benefit in preventing migraine recurrence, and we would recommend a single dose of 10 mg IV dexamethasone for moderate-severe migraine.

Bottom Lines
- Propofol is cheap, effective and safe – more studies are required, but it is likely an effective treatment option for patients with refractory migraines.
- Magnesium is highly accessible, cheap, safe, easy to administer and appears to be highly efficacious for headache resolution.
- Dexamethasone has been demonstrated to significant reduce migraine recurrence following therapy, and we would recommend an single dose of 10 mg IV.

Dr. Tamara McColl is an 5th year Emergency Medicine resident at the University of Ottawa, with an special interest in medical education.
Edited by Dr. Shahbaz Syed, 4th year University of Ottawa Emergency Medicine Resident.
References
- Kruz et al. Intravenous propofol: Unique effectiveness in treating intractable migraine. Headache. 2000. 40(3): 224-30
- Soleimanpour et al. Effectiveness of intravenous dexamethasone versus Propofol for pain relief in the migraine headache: A prospective double blind randomized clinical trial. BMC Neurology. 2012. 12:114
- Sheridan et al. Low-dose propofol for the Abortive Treatment of Pediatric Migraine in the Emergency Department. Pediatr Emer Care. 2012. 28: 1293-96.
- Moshtaghion et al. The Efficacy of Propofol vs. Subcutaneous Sumatriptan for Treatment of Acute Migraine Headaches in the Emergency Department: A Double-Blinded Clinical Trial. 2014. Pain Practice. 15(8): 701-5
- Demirkaya et al. Effectiveness of intravenous magnesium sulfate in the treatment of acute migraine attacks. Headache. 2001. 41:171-177
- Bigal et al. Intravenous magnesium sulphate in the acute treatment of migraine without aura and migraine with aura. A randomized, double-blind, placebo-controlled study. Cephalagia. 2002. 22:345-353.
- Shahrami et al. Comparison of the therapeutic effects of magnesium sulphate vs dexamethasone/metoclopramide on alleviating acute migraine headache. J Emerg Med. 2015. 48(1):69-76
- Colman et al. Parenteral dexamethasone for acute severe migraine headache: meta-analysis of randomized controlled trials for preventing recurrence. BMJ. 2008. 336 (7657):1359-61
- Huang et al. Steroids for preventing recurrence of acute severe migraine headaches: a meta-analysis. Eur J Neurol 2013. 20:1184-1190