
We have seen a large surge of the utilization of New Oral Anticoagulants (NOAC’s) in the past few years, as such, it has been a novel challenge when these patients present to the Emergency Department (ED) with life threatening bleeding. Dr. Michael Ho looks to discuss treatment options, and future options in these patients.
NOACs vs Warfarin
Dabigatran, Rivaroxaban and Apixaban have seen a dramatic increase in use since their approval in Canada. Dabigatran is a direct thrombin (Factor II) inhibitor, while the latter two are direct Xa inhibitors. These drugs are collectively referred to as novel oral anticoagulants (NOACs). They have also been called direct, or target-specific oral anticoagulants (DOACs or TSOACs) [1].
The NOACs have many practical advantages over warfarin:
- Rapid onset of action
- Shorter half-life
- Less food and drug interference
- Predictable pharmacokinetics
- Ease of use and no requirement for monitoring
The downsides to NOACs are the higher cost to the patient, the inability to easily quantify anticoagulant effect and a lack of specific reversal agent.
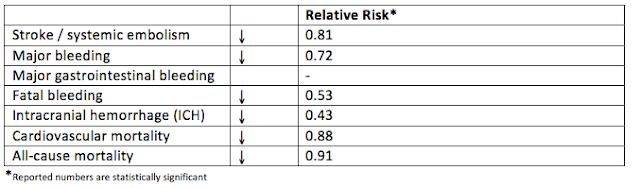
Clinically, NOACs have demonstrated significant advantage over warfarin [2,3].
Because of their practical and clinical advantages, NOAC use will continue to rise [4]. Even with decreased bleeding rates and better outcomes with bleeding (mostly due to reduced ICH), many clinicians still have some reluctance with prescribing NOACs due to the lack of a specific reversal agent.
Reversal of anticoagulation
Warfarin
Since warfarin induces anticoagulation by inhibiting the synthesis of vitamin K dependent factors (II, VII, IX, X, C+S), the simple and easy reversal strategy is to replace the factors [5].
Warfarin reversal in life threatening bleeding can be accomplished with either:
- Fresh Frozen Plasma (FFP) + Vitamin K
- Prothrombin Complex Concentrate (PCC) + Vitamin K
PCC has been shown to reverse INR much more quickly than FFP, in the range of 30-60 minutes. PCC also requires less volume for infusion (<100 ml PCC vs 1 L for 4 units of FFP), and therefore avoids problems with fluid overload and pulmonary edema [5,6].
NOACs
Current practice for reversal of NOACs in life threatening bleeding uses the following principles [1,7,8]:
- Stop all anticoagulants and antiplatelet agents
- Identify the source of bleeding and apply local and surgical measures as appropriate
- Supportive measures (volume, pRBCs, platelets) as needed
- Confirm timing of last dose of NOAC, if <4 hours consider activated charcoal
- Measure coagulation parameters: PT/INR, aPTT, anti-Xa, TT
- If patient is taking dabigatran and
-
- TT is normal: there is no drug on board
- TT abnormal but aPTT normal: clinically insignificant drug on board
-
- If patient is taking apixaban or rivaroxaban and
-
- Anti-Xa < 0.1: no drug on board
- Calculate CrCl and estimate half-life [1]
- Most NOACs have a half-life of approximately 12-14 hours
- Accumulation of drug does not occur
- Low plasma concentrations of all NOACs are expected after one half-life
- Administer 4-factor PCC of FEIBA [7]
- The evidence for administering PCC or activated PCC (FEIBA) for life threatening bleeding is based off weak evidence in animal models, in vitro studies and studies on healthy volunteers.
- Evidence slightly favours FEIBA for Dabigatran reversal and 4-factor PCC for Xa inhibitor reversal.
- Requires high doses (>50 U/kg) to “overload” the coagulation system with clotting factors and induce thrombin generation in the setting of thrombin of Xa inhibition.
- Concerns with this strategy: non-specific reversal, increased risk of thrombosis with high dose PCC, inconsistent experimental data, and no human data demonstrating benefit.
- At the Ottawa Hospital (TOH) we currently use FEIBA for all NOAC bleeding for simplicity.
- For patients on Dabigatran, hemodialysis can be considered [7].
- 50% of active Dabigatran is removed after 4 hours of HD in ESRD patients
- Xa inhibitors are too highly protein bound for HD to be useful.
Idarucizumab (Praxbind)
In response to the demand for a specific reversal agent for dabigatran, Boehringer Ingelheim (manufacturer of dabigatran) engineered a Praxbind, a monoclonal antibody fragment that binds to dabigatran and thrombin-bound dabigatran at an affinity 350x stronger than endogenous thrombin. In animal studies, it has shown to significantly decrease bleeding and clinical outcomes [9]. In a phase I human study, it showed rapid biochemical reversal of dabigatran by measure of dilute thrombin time and ecarin clotting time – both validated measures of dabigatran plasma concentration. Complications and adverse events were reported to be very low [10,11].
The REVERSE-AD trial, an international multi-center prospective cohort (phase III) study evaluating the reversal of dabigatran in patients with life threatening bleeding or requiring urgent surgery is currently ongoing [12]. Target enrolment is 300 patients. The authors (Pollack et al.) published an interim analysis of their first 90 patients in NEJM, which led to the approval for use of Praxbind in the U.S. and Europe. Here is a summary of their paper:
Enrolment:
- 90 patients, 86 were taking Dabigatran for atrial fibrillation
- Group A: Life threatening bleeding: 51 patients
- Group B: Emergency procedures: 39 patients
Primary Outcome: Reversal at 4 hours post infusion of Praxbind using dilute thrombin time (dTT) and ecarin clotting time (ECT)
Secondary Outcomes:
- Group A: Time to hemostasis, modified Rankin scores for ICH patients and hemodynamic stability.
- Group B: intraprocedural hemostasis, periprocedural bleeding for 24 hours
Results
- Primary
- 11/51 patients had normal Dabigatran levels at baseline, they were excluded from analysis.
- At 4 hours, 100% of the remaining 40 patients were reversed with Praxbind
- Normalization of dTT and ECG occurred within 30 minutes of Praxbind infusion.
- Secondary
- Group A:
- Bleeding assessable in 35/51 patients
- Median time to hemostasis: 11.4 hours
- Group B:
- Normal hemostasis in 33/36 patients
- Adverse events:
- 18 deaths (20% mortality rate)
- 5 thrombotic events (1 in the first 72 hours, others after day 7)
- 2 GI bleeds
- Group A:
PROs:
- International, mutli-center trial
- Robust demonstration of biochemical reversal
- Hemostasis evaluated
- Only 2 patients lost to follow up.
CONs:
- Group A (Life threatening bleeding)
- No Control group
- Authors state a control group “…would be unethical to assign patients to receive placebo or no active treatment” – the authors here are making a big assumption that their drug is already clinically effective and safe.
- How can we make any conclusions about the clinical efficacy and safety of this drug without a control group?
- Small sample size
- Difficult to make conclusions about safety
- Mortality rate was high (20%)
- Typical mortality rate of major extracranial bleeding is 5-8% in other studies. Only 4/90 (4.4%) of deaths were due to ICH. Was this study group just very sick, or did the study drug increase the mortality rate? Without a control group, there is no way to know.
- Only 50% of patients in Group A with “life threatening bleeding” required a blood transfusion.
- They did not report bleeding scores
- They did not report modified Rankin score outcomes for ICH patients
- Study was funded by Boehringer Ingelheim, the company that engineered the drug
- No Control group
- Group B (emergency procedures)
- Were these procedures truly emergent?
- Most commonly performed procedure: orthopedic OR
- Other included procedures:
- LP, abscess I&D, HD line placement, ureteric stents
- No neurosurgical interventions
- Subjective assessment of intraoperative hemostasis
- Were these procedures truly emergent?
Bottom Line
- This study confirms phase I trial findings of biochemical reversal of effect in bleeding patients and patients requiring emergency procedures
- (Subjectively) normal hemostasis was reported
- Does not convincingly report a clinically meaningful benefit
- Safety still in question
Availability and Cost
- Under accelerated approval by FDA in US and Europe
- Submitted for approval in Canada Feb 2016
- Expected cost: $3400 per dose (2 x 2.5g)
- Cost direct to hospital pharmacy
- Comparison
- FEIBA: $3500
- PCC: $1500
- 6 units FFP: $1500
- These costs are direct to Canadian Blood Services
- Expected to be available in the ER at TOH, use restricted by Thrombosis
- Expected indication: life threatening bleeding (including ICH) and the need for emergency surgery / procedure within 8 hours.
Antidote Pitfalls
- Worth mentioning that having this (expensive) antidote might lead to [1]:
- Overuse when it is unclear if patient is taking an anticoagulant OR which one they are taking
- Careless timing of invasive procedures
- Delay in necessary intervention
- We also have no idea how to use this drug in the case of overdose.
Does reversal of anticoagulation help our patients?
We’ve been talking a bit about reversing bleeding with NOACs, but does reversal make a clinically meaningful difference to our patients? To look at this question, the best place to look is warfarin. Warfarin has been around for a long time, and reversal is easy (replace the factors) and fast (PCC).

Evidence that rapid reversal makes no difference:
- Zubkov et al. Arch Neurol 2008 [13]
- 88 patient prospective cohort with warfarin-related ICH reversed with FFP and Vitamin K.
- Initial INR and time to INR reversal had no correlation with survival to 7 days in univariate or multivariate analyses.
- Sarode et al. Circulation 2013 [5]
- 202 patient RCT reversing warfarin-related major bleeding with FFP vs PCC
- Similar hemostatic efficacy at 24 hours
- No difference in 30-day mortality rate
- The 45-day mortality rate was 9.7% vs 4.6% favouring FFP (authors state these deaths not related to reversal).
- Alonso et al. Thromb Haemost 2013 [14]
- 71 patient prospective cohort of warfarin-related ICH, reversed with PCC + Vitamin K
- Baseline INR, anticoagulation reversal, hematoma enlargement were not related to functional outcomes.
Evidence that rapid reversal is helpful:
- Tilton et al. Ann Pharm 2014 [15]
- 403 patient retrospective study of 3-factor PCC for reversal of warfarin-related acute bleeding
- Achieving INR < 1.5 correlated with survival (OR 3.8, P<0.01).
- Tazarourte et al. Crit Care 2014 [16]
- 822 patient prospective study of 4-factor PCC + Vitamin K for reversal of warfarin-related severe bleeding
- Giving PCC ≥ 20 units/kg and vitamin K ≥ 5 mg IV within 8 hours was associated with:
- 2-fold reduction in 7-day mortality in all patients
- 3-fold reduction in 7 day mortality for ICH patients
- Steiner et al. Int J Stroke 2011 (INCH trial) [17]
- The INCH trial is an open-label RCT comparing reversal of warfarin-related ICH with FFP vs PCC. These unpublished results were presented at the International Stroke Conference (Feb 2016) and are available online.
- In favour of PCC:
- Decreased rate of hematoma expansion
- Mortality rate 19% vs 35% (non-sig, P=0.14)
- All 4 deaths in the first 48 hours were int he FFP group – all of these were related to hematoma expansion
- First death in PCC group was at day 5, due to cardiac arrest
- No difference in functional outcomes
Overall, there isn’t any high quality evidence suggesting a clear benefit with rapid INR normalization. Perhaps outcomes in these ICH patients are independent of INR reversal, but it is likely the outcomes of extracranial bleeding (that hasn’t been studied well) would benefit. Regardless, we have a very good scientific basis to treat coagulopathy in these patients.
The truth will be similar for NOAC reversal agents for quite some time, and we will likely be forced to use these antidotes in the absence of robust clinical data in life threatening bleeding.
Upcoming development: Andexanet alfa (Xa inhibitor reversal agent)
This is a recombinant modified form of factor Xa that binds to Xa inhibitors (apixaban, rivaroxaban, edoxaban) with similar affinity to endogenous factor Xa18. It was created by Portola Pharmaceuticals Inc. It doesn’t assemble into a prothrombinase complex but has been shown to compete with factor Xa binding to tissue factor pathway inhibitor (TFPI) to produce a procoagulant effect.
ANNEXA Trials
The ANNEXA trials are parallel RCTs whose results were reported by Siegal et al. NEJM 2015 [19]. They assessed the reversal of anticoagulation with apixaban and rivaroxaban with andaxanet alfa in 101 healthy older volunteers aged 50-75.
Results for Apixaban:
- Anti-Xa activity reduced by 94% compared to 21% with placebo
- Thrombin generation restored to 100% vs 11%
Results for Rivaroxaban:
- Anti-Xa activity reduced by 92% compared to 18% with placebo
- Thrombin generation restored 98% vs 7%.
For both groups, there were transient increases in D-Dimer and Prothrombin fragments 1+2 suggesting risk of thrombosis. No serious adverse effects or thrombotic events were reported in this 101 patient study.
Phase II Study
There is an ongoing Phase III trial similar to the REVERSE-AD trial for dabigatran (ClinicalTrials.gov: NCT02329327)
- Estimated enrolment of 270 patients with major bleeding while using a Xa inhibitor in the last 18 hours
- Co-primary efficacy endpoints
- Change in Anti-Xa levels within 2 hours
- Effective hemostasis within 12 hours
- 45-day safety follow up
- No control group
It’s very easy to imagine that the results of this study will be similar to those in the interim analysis of the Reverse-AD trial (Pollack et al NEJM 2015) [12]. That is, they will demonstrate biochemical evidence of reversal in bleeding patients, subjective ratings of hemostasis and they will describe clinical outcomes that will be meaningless without a control group.
Given the demonstrated transient increases in D-Dimer and Prothrombin fragments 1+2, it will be interesting to see if this drug does cause thrombotic events, particularly in patients with comorbid illnesses.
Upcoming development: Ciraparantag / PER977 (NOAC and Heparin reversal)
This is a very interesting development from Perosphere Inc. Ciraparantag is a small, water-soluble cationic molecule that binds to UFH, LMWH and NOACs via non-covalent binding and charge-charge interactions. It does not interfere with warfarin or commonly used cardiac, anesthetic or antiepileptic drugs. Ex vivo testing using thromboelastography suggests no pro-coagulant activity
Experimental data [20]
- Rat tail transection model using Dabigatran, Rivaroxaban, Apixaban and Edoxaban
- 12.5 mg PER977 decreased bleeding by >90% vs control
- Rats given Edoxaban: thromboelastography assays normalized within 30 minutes with 20 mg/kg PER977.
- Human in vitro study: reduced anti-Xa activity of Rivaroxaban, Apixaban, Enoxaparin in dose-dependent relationship
- A phase I study of 80 healthy volunteers showed rapid reversal of whole blood clotting time in patients receiving Edoxaban
- Phase II trials are ongoing..
Bottom Lines
- NOACs are safer than warfarin, and are here to stay.
- Reversal of anticoagulation has not convincingly been shown to improve clinical outcomes, even when it is safe and effective.
- Reversal agents for NOACs are coming, whether we want them or not. Their biochemical results are robust, but their clinical benefits are not yet proven. We will likely be forced to use these drugs without evidence of clinical benefit for the time being.
- Idarucizumab (Praxbind) will likely soon be available in Canadian EDs, and they will be indicated for life threatening bleeding and emergency procedures/surgery.
- Drugs to watch for:
- Andexant alfa (Xa inhibitor reversal)
- Ciraparantag (NOAC and heparin reversal)

Dr. Michael Ho is a 4th year Emergency Medicine resident at the University of Ottawa, with a special interest in resuscitative medicine.
Edited by Dr. Shahbaz Syed, PGY-4 Emergency Medicine resident at the University of Ottawa.
References
1. Husted S, Verheugt FWA, Comuth WJ. Reversal Strategies for NOACs: State of Development, Possible Clinical Applications and Future Perspectives. Drug Saf. 2015;39(1):5-13. doi:10.1007/s40264-015-0357-x.
2. Chai-Adisaksopha C, Hillis C, Isayama T, Lim W, Iorio A, Crowther M. Mortality outcomes in patients receiving direct oral anticoagulants: A systematic review and meta-analysis of randomized controlled trials. J Thromb Haemost. 2015;13(11):2012-2020. doi:10.1111/jth.13139.
3. Chai-adisaksopha C, Crowther M, Isayama T, Lim W. The impact of bleeding complications in patients receiving target-speci fi c oral anticoagulants : a systematic review and meta-analysis. Blood. 2014;124(15):2450-2459. doi:10.1182/blood-2014-07-590323.The.
4. Xu Y, Holbrook AM, Simpson CS, Dowlatshahi D, Johnson AP. Prescribing patterns of novel oral anticoagulants following regulatory approval for atrial fibrillation in Ontario, Canada: a~population-based descriptive analysis. C open. 2013;1(3):E115-E119. doi:10.9778/cmajo.20130032.
5. Sarode R, Milling TJ, Refaai MA, et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: A randomized, plasma-controlled, phase IIIb study. Circulation. 2013;128(11):1234-1243. doi:10.1161/CIRCULATIONAHA.113.002283.
6. Hickey M, Gatien M, Taljaard M, Aujnarain A, Giulivi A, Perry JJ. Outcomes of urgent warfarin reversal with frozen plasma versus prothrombin complex concentrate in the emergency department. Circulation. 2013;128(4):360-364. doi:10.1161/CIRCULATIONAHA.113.001875.
7. Dickneite G, Hoffman M. Reversing the new oral anticoagulants with prothrombin complex concentrates (PCCS): What is the evidence? Thromb Haemost. 2013;111(2):189-198. doi:10.1160/th13-05-0431.
8. Siegal DM, Garcia D a, Crowther M a, Dc W. How I treat target-specific oral anticoagulant − associated bleeding How I Treat How I treat target-speci fi c oral anticoagulant – associated bleeding. Blood. 2014;123(8):1152-1158. doi:10.1182/blood-2013-09-529784.
9. Grottke O, Honickel M, Van Ryn J, Ten Cate H, Rossaint R, Spronk HM. Idarucizumab, a Specific Dabigatran Reversal Agent, Reduces Blood Loss in a Porcine Model of Trauma with Dabigatran Anticoagulation. J Am Coll Cardiol. 2015;66(13):1518-1519. doi:10.1016/j.jacc.2015.07.051.
10. Eikelboom JW, Quinlan DJ, Van Ryn J, Weitz JI. Idarucizumab the antidote for reversal of dabigatran. Circulation. 2015;132(25):2412-2422. doi:10.1161/CIRCULATIONAHA.115.019628.
11. Schiele F, Ryn J Van, Canada K, et al. A specific antidote for dabigatran : functional and structural characterization. 2013;121(18):3554-3562. doi:10.1182/blood-2012-11-468207.The.
12. Pollack C V, Reilly P a, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal. N Engl J Med. 2015:1-10. doi:10.1056/NEJMoa1502000.
13. Zubkov AY, Mandrekar JN, Claassen DO, Manno EM, Wijdicks EFM, Rabinstein AA. Predictors of outcome in warfarin-related intracerebral hemorrhage. Arch Neurol. 2008;65(10):1320-1325. doi:10.1001/archneur.65.10.1320.
14. de Lecinana MA, Huertas N, Egido JA, et al. Questionable reversal of anticoagulation in the therapeutic management of cerebral haemorrhage associated with vitamin K antagonists. Thromb Haemost. 2013;110(6):1145-1151. doi:10.1160/TH13-04-0318.
15. Tilton R, Michalets EL, Delk B, Sutherland SE, Ramming SA. Outcomes Associated With Prothrombin Complex Concentrate for International Normalized Ratio Reversal in Patients on Oral Anticoagulants With Acute Bleeding. Ann Pharmacother. 2014;48(9):1106-1119. doi:10.1177/1060028014537897.
16. Tazarourte K, Riou B, Tremey B, Samama C-M, Vicaut E, Vigué B. Guideline-concordant administration of prothrombin complex concentrate and vitamin K is associated with decreased mortality in patients with severe bleeding under vitamin K antagonist treatment (EPAHK study). Crit Care. 2014;18(2):R81. doi:10.1186/cc13843.
17. Steiner, T., Poli S., Griebe M., Husing J., Hajda J., Bendszus M., Boesel J., Christensen H., Dohmen C., Freiberger A., Hennerici M., Kolmer J., Stetefeld H., Wartenberg .E., Weimer C., Hacke W. VR. International normalized ratio Normalization in patients with Coumarin-related intracranial Haemorrahges – randomized controlled multicentre trial to compare safety and preliminary efficacy of fresh frozen plasma and prothrombin complex – Presented at Int. In: ; 2016.
18. Lu G, DeGuzman FR, Hollenbach SJ, et al. A specific antidote for reversal of anticoagulation by direct and indirect inhibitors of coagulation factor Xa. Nat Med. 2013;19(4):446-451. doi:10.1038/nm.3102.
19. Siegal DM, Curnutte JT, Connolly SJ, et al. Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. N Engl J Med. 2015:151111074542008. doi:10.1056/NEJMoa1510991.
20. Ansell JE, Bakhru SH, Laulicht BE, Steiner SS, Grosso M, Brown K, Dishy V, Noveck RJ CJ. Use of PER977 to reverse the anticoagulant effect of edoxaban. New Engl J Med. 2014;371(22):2141-2142.