A male in his 60’s presents with progressive dyspnea on exertion x 1 month starting while he was swimming in the ocean. He had not been diving. He has no significant medical history and takes no medications.
Two weeks after the onset of symptoms the patient had seen his family physician. A chest X-ray (CXR) was completed and was normal. An outpatient stress ECHO was requested.
The patient had had two Emergency presentations:
- On his first ED visit he was assessed for shortness of breath. He was having no chest pain and vitals were within normal limits. The following investigations were normal: CXR, CBC, electrolytes, BUN, Creatinine, CK and TnI. The patient was discharged home pending the outpatient stress ECHO and told to return if symptoms worsened.
- On the second ED visit 6 days later, the patient complained of worsening SOBOE, no chest pain, no PND, no orthopnea, no fever or cough, no leg pain or edema. There were no known PE risk factors. He is a non-smoker, drinks ETOH occasionally.
On exam:
Triage vitals: 35.7 HR 84 BP 179/83 RR 24 O2 sat 95% r/a
Patient appears in no acute distress but respiratory rate is noticeably increased.
CVS normal S1/S1 no S3/S4, no murmurs, JVP not elevated
Equal pulses bilateral
Chest clear
No unilateral extremity warmth, erythema or tenderness along deep venous system
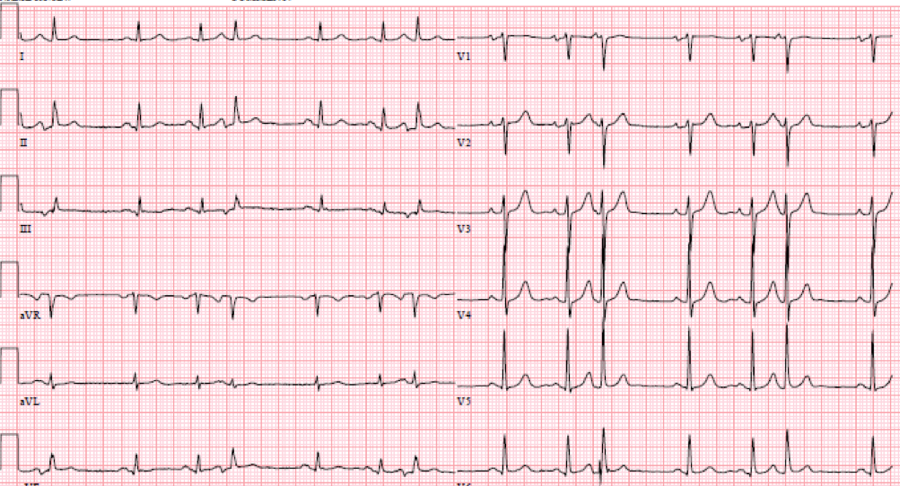
ECG from 1st ED visit, 6 days prior:

ECG analysis: NSR. Normal axis. Narrow QRS. Few PACs. No ST segment/T wave changes.
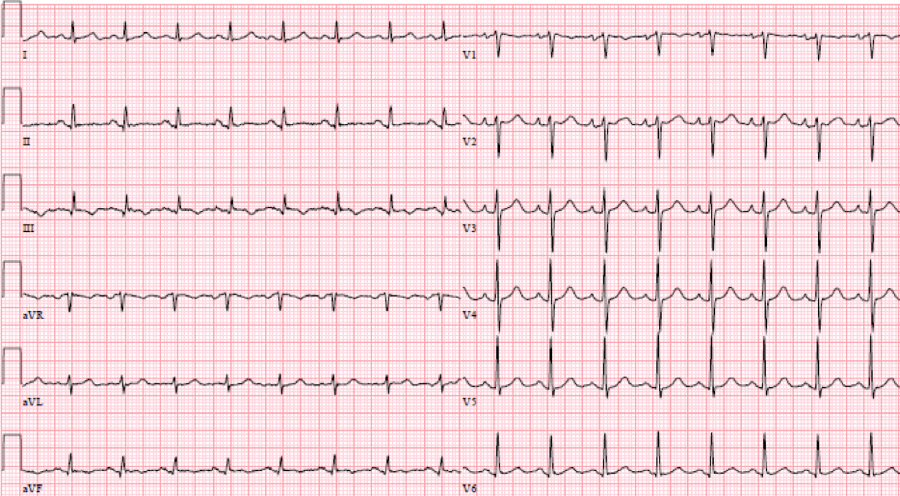
ECG on the day of presentation:
ECG analysis: Borderline sinus tachycardia. Normal Axis. Narrow QRS. New T wave inversion lead III. Q wave lead 3. No block. No other ST segment/T wave changes.
At this point consider your differential.
It should remain broad and, really, could include most items listed for dyspnea with a normal chest XR. This includes anemia, ACS, heart failure, obstructive lung disease, metabolic abnormalities, pericardial effusion/pericarditis, neuromuscular disorders, pulmonary HTN, airway issues and medicine’s greatest enigma, a pulmonary embolism.
A point-of-care ultrasound scan was done to help narrow the differential.
Below are three cardiac views. Think of what you would be looking for given the clinical scenario.
 |
| PSLA |
 |
| PSSA |
 |
A4C
Mostly with intermediate point of care echocardiography, in this patient, we would be looking for gross LV function using the “eyeball” method, presence of a pericardial effusion and rough RV:LV size.
In these images, we can estimate that the LV function is grossly normal and there is no pericardial effusion. Unfortunately, due to quality, we are unable to comment on the RV:LV size ratio. However, we would be looking for a RV:LV ratio of 0.6:1 as normal with a ratio of 1:1 as severe RV dilation.
We can eliminate a few diagnoses off the differential with this scan. However, with the diagnosis of PE remaining a 2-point DVT scan was carried out:
Right lower extremity
|
In each of these images it appears the vein fully collapses with compression. We can conclude that there is likely no DVT present within the limitations of the 2-point compression scan (see discussion for further details)
If we incorporate our Wells score for PE and our scan as above we can generate a diagnostic algorithm:
Using this algorithm, a positive POCUS DVT scan can eliminate the need for CT, however a negative scan should be combined with a D-dimer to guide further testing.
In our patient:
Wells Score: 3 (PE as likely or more likely than alternative)
D-Dimer: 6024
Troponin: 459
Due to the positive D-Dimer a CT-PE was carried out, demonstrating:
Large pulmonary emboli in the right pulmonary artery, right upper, middle and lower lobar arteries and left lower lobar artery. There are also smaller numerous bilateral segmental emboli. Moderate degree of right heart strain.
The patient was admitted to hospital, anti-coagulated, was discharged home on day 2 of admission on Dalteparin.
Radiology performed bilateral leg Dopplers were negative for DVT.
Discussion
1. Your clinical gestalt must supercede your PoCUS result. If your scan is suboptimal then call it indeterminate and proceed to a definitive investigation such as the CTPE study in this case.
2. 2-Zone Lower extremity DVT PoCUS can be very helpful when it is positive for DVT. However one should not rely on a negative PoCUS DVT scan to definitively rule out a DVT. Additional investigations such as the d-dimer and radiology performed Doppler US should be performed if there is a reasonable clinical suspicion for thromboembolism.
Expert Reviewer:
PoCUS for DVT (2-zone technique) has been shown to have a high sensitivity and specificity, when compared to a gold-standard of radiology performed ultrasound. Therefore, it is reasonable to use it to exclude DVT in patients who have a low clinical probability of DVT.
However, the 2-zone technique will miss clots that are isolated to the mid femoral vein (ie, above the popliteal zone and below the sapheno-femoral junction). Fortunately, it is felt that clots isolated to this part of the venous system are uncommon. PoCUS will also likely miss calf vein thrombosis. The management of calf vein thrombosis is an area of controversy, but patients with isolated calf vein thrombosis are certainly at lower risk of fatal VTE than those with more proximal clots. In my practice, I will discharge low risk patients with a negative PoCUS, but I will advise them to return to the ED if they have progression of swelling or pain, which might indicate extension of a calf vein thrombosis.
When a patient is suspected of having a pulmonary embolism, ultrasound for DVT has utility because a positive result may obviate the need for chest imaging. This approach is often used in pregnant patients. However, a negative result (PoCUS or radiology performed) cannot end the workup as many, even most, patients with PE will have a negative leg ultrasound.
PoCUS strategies to diagnose pulmonary embolism have usually focused on right heart dilation or strain. These findings will only be present in larger, more hemodynamically significant PEs, therefore they lack sensitivity. Lung PoCUS for pleural based infarcts shows promise, but this technique requires more operator skill and requires further study.