

The Zika Virus exploded onto the international health scene in the last several months. It was first discovered in humans in 1951 and remained limited to Africa and Asia until the first major outbreak in Micronesia in 2007. Since then the virus has continued to evolve and spread from the Pacific Islands and French Polynesia to the main major outbreak in South America in early 2015 and finally to the US in January 2016.
The virus itself is a single stranded RNA virus from the flavivirus family. This family also includes dengue, chikungunya, West Nile and yellow fever. Zika is mainly transmitted by the Aedes aegypti mosquito.2
Zika Symptoms
Approximately 20-25% of patients who contract Zika will have symptoms. Most will experience a self-resolving viral illness. Symptoms usually last 2-7 days.2
The symptoms of Zika include:2,3
- Low grade fever (usually <38.5C)
- Myalgias/arthralgias (hands/feet)
- Retro-orbital pain
- Conjunctivitis
- Maculopapular rash
- Lymphadenopathy
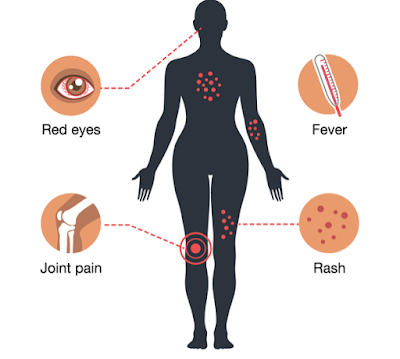
The symptoms of Zika are very similar to dengue and chikungunya. It is very difficult to tell these viral infections apart on the basis of history and physical exam alone.
Canadian Statistics
As of November 3, 2016 Canada has experienced:1
- 359 Zika travel related cases
- 2 sexually transmitted cases
- 16 Zika infected pregnancies
- Of these 16 pregnancies 2 had vertical transmission
- 1 of these neonates had Zika related abnormalities at birth
- Of these 16 pregnancies 2 had vertical transmission
 |
|
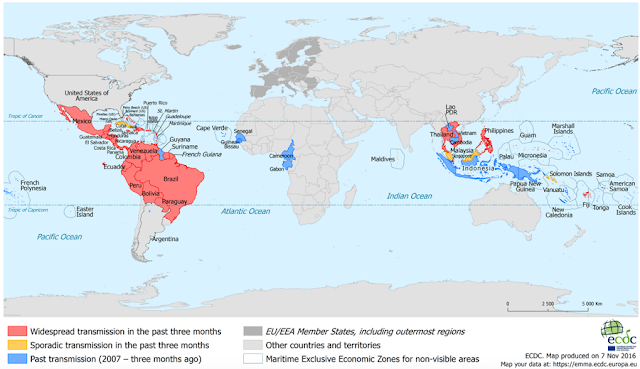
Current Worldwide Status of ZikaCurrent known routes of transmission2
Prevention of Zika Infection – General2
Prevent mosquito bites2
Prevent sexual transmission2
Diagnosis of Zika2
|
There are currently 2 different categories of tests:
- PCR to detect the virus itself
- Serology to detect antibodies to the virus
Antibodies appear 5-6 days post symptom onset. There is some known cross-reactivity between the assays used to detect antibodies against Zika and other flaviviruses (especially dengue).
For patients presenting with:
- < 10 days of symptoms – PCR and serology needs to be completed
- > 10 days of symptoms – only serology needed
Chikungunya and dengue testing are automatically added to any Zika tests sent.8
The current turn-around times are:
- PCR – up to 14 days
- Serology – 3-8 weeks
In addition to the general Public Health requisition there is a specific “Mandatory Information Intake Form for Zika Virus Testing” that must also be completed with any blood work sent. This form can be found online at Public Health Ontario.
Current Diagnostic Approach to Zika Virus at The Ottawa Hospital8

There is currently no universal screening of returned travellers or patients with potential Zika contact. This has been decided at the national level.
The only patients currently being tested include:
- Patients with symptoms
- Asymptomatic pregnant women
- Asymptomatic women who may become pregnant
Potential Zika cases or pregnant asymptomatic patients with possible Zika contact are all currently being referred to the TOH Tropical Disease Clinic. Zika blood work drawn in the ED can be followed at this clinic.
If pregnant women are found to have Zika, or their symptoms are very suggestive of Zika, they will be referred by the Tropical Disease Clinic to Maternal Fetal Medicine (MFM). There is no need to refer these patients directly from the ED to Maternal Fetal Medicine.
On the referral form please include:
- Travel location
- Dates of travel
- Symptoms & onset
- Pregnancy status
- Flavivirus vaccinations
- Japanese encephalitis
- Yellow fever
Treatment of Zika Virus2
There is currently no specific antiviral treatment for Zika. The treatment is supportive, similar to treatment for other viral illnesses. The patient should be advised to rest, stay hydrated and take acetaminophen if needed for pain or fever. They should avoid NSAIDs until dengue is ruled out. Symptoms should resolve within 7 days.
Complications – GBS
- Guillain-Barre syndrome is the most commonly reported and most researched serious complication of Zika virus2
- Cao-Lormeau et al., 2016 conducted a case control study in French Polynesia9
- 2 sets of controls
- 1 – patients with non-febrile illness who presented to ED
- 2 – patients with Zika but no GBS symptoms
- Had 42 patients with GBS during study
- 98% had anti-Zika 1gM or IgG
- All had neutralizing antibodies
- Found incidence of GBS during outbreak was 1 in 4 000 Zika infected patients
- 98% had anti-Zika 1gM or IgG
- 2 sets of controls
Zika and Pregnancy

Zika has been implicated in a variety of pregnancy complications.2
Currently this list includes:
- Microcephaly
- Fetal death
- Placental insufficiency
- Fetal growth restriction
- CNS injury
Brasil et al. 2016 enrolled 88 pregnant women into a prospective clinical trial. Of 88 pregnant women who presented to the study clinics with a new rash 72 were found to be positive for Zika in blood or urine. 42 of the 77 completed the required US.3
Of these 42 women 12 had fetal abnormalities on US:
- 2 fetal deaths (36 + 38 wks GA)
- 5 IUGR (+/- microcephaly)
- 4 ventricular calcifications
- 4 abnormal cerebral or umbilical artery flow
- 2 abnormal amniotic fluid volume
- 2 CNS lesions
Abnormalities on US were found in women who contracted the virus through all trimesters (see figure below).
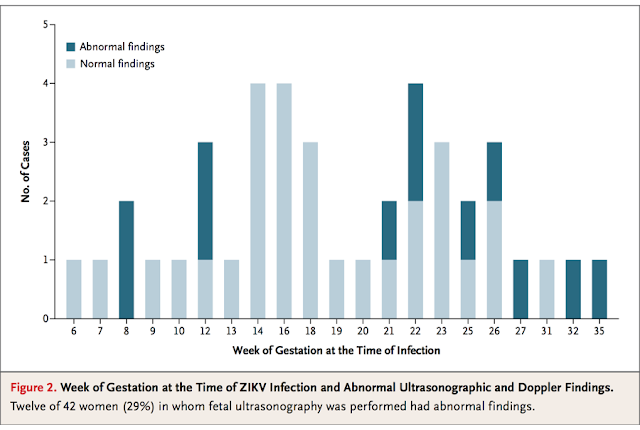 Brasil P, Pereira J,Jose P., Raja Gabaglia C, Damasceno L, Wakimoto M, Ribeiro Nogueira RM, et al. Zika Virus Infection in Pregnant Women in Rio de Janeiro — Preliminary Report. N Engl J Med 2016;ePub. |
|
Cauchemez etal. 2016 conducted a retrospective analysis looking at the gestational age at which the risk of Zika induced microcephaly peaks.10 They collected serological and surveillance data to estimate infection risk. They then used this data in conjunction with information regarding 8 cases of microcephaly found during the outbreak to find the best mathematical model to predict periods of risk during pregnancy.
The best model found risk highest in 1st trimester and possibly early 2nd trimester. The risk of microcephaly was predicted to be 1% in women who contract Zika in the 1st trimester.
Top 5 Take Home Points1. List of Zika infected countries is constantly changing
o Refer patients to the Zika websites at WHO, CDC or Health Canada for current information
2. Most patients who contract Zika will have a benign viral illness
3. Risk of GBS with Zika is 1 in 4 000
4. Zika causes microcephaly, especially in 1st trimester
5. In the ED for a patient suspected of having Zika:
o Draw blood work (and complete the 2 requisitions)
o Refer to Tropical Medicine Clinic
 Dr. Julia Traer, MD, CCFP is a 3rd year resident in the CCFP-EM Program at the University of Ottawa.
-Edited and Formatted by Dr. R Suttie, PGY2 at the University of Ottawa
‘
References:1. Government of Canada. Surveillance of Zika virus. http://www.healthycanadians.gc.ca/diseases-conditions-maladies-affections/disease-maladie/zika-virus/surveillance-eng.php#s2-1. Accessed November 7, 2016.
2. Zika Working Group on behalf of the Committee to Advise on Tropical Medicine and Travel (CATMAT). Canadian recommendations on the prevention and treatment of Zika virus: Update. Can Comm Dis Rep 2016;42:101-11
3. Brasil P, Pereira J,Jose P., Raja Gabaglia C, Damasceno L, Wakimoto M, Ribeiro Nogueira RM, et al. Zika Virus Infection in Pregnant Women in Rio de Janeiro — Preliminary Report. N Engl J Med 2016;ePub.
4. Centers for Disease Control and Prevention. Zika Basics: Flipbook for Community Health Workers. https://www.cdc.gov/zika/pdfs/zika_basics_low-literacy_flipbook.pdf. Accessed November 7, 2016.
5. European Centre for Disease Prevention and Control. Current Zika transmission. http://ecdc.europa.eu/en/healthtopics/zika_virus_infection/zika-outbreak/pages/zika-countries-with-transmission.aspx. Accessed November 7, 2016.
6. World Health Organization. Zika virus, Microcephaly and Guillain-Barré Syndrome Situation Report 3 November 2016. 2016; http://apps.who.int/iris/bitstream/10665/250724/1/zikasitrep3Nov16-eng.pdf?ua=1 Accessed November 7, 2016.
7. Musso D, Nhan T, Robin E, Roche C, Bierlaire D, Zisou K, et al. Potential for Zika virus transmission through blood transfusion demonstrated during an outbreak in French Polynesia, November 2013 to February 2014. Euro Surveil 2014;19(14):20761.
8. The Ottawa Hospital. TOH Zika Management Plan & Information for Health Care Providers. The Ottawa Hospital intranet. Accessed November 20, 2016.
9. Cao-Lormeau V, Blake A, Mons S, Lastere S, Roche C, Vanhomwegen J, et al. Guillain-Barré Syndrome outbreak associated with Zika virus infection in French Polynesia: a case- control study. Lancet 2016;ePub.
10. Cauchemez S, Besnard M, Bompard P, Dub T, Guillemette-Artur P, Eyrolle-Guignot D, et al. Association between Zika virus and microcephaly in French Polynesia, 2013–15: a retrospective study. Lancet 2016;ePub.
|