
With the protocols and time constraints of our ED environment, it is fairly easy to fall into the trap of imaging prior to examining our orthopedic patients. This may result in missed injuries, as we tend to base our diagnosis on the X-ray, rather than the patient assessment. In today’s post, we will review relatively common but frequently missed lower extremity orthopedic injuries including a general approach, focused assessment, and management of these injuries.
Introduction: Commonly Missed Lower Extremity Injuries
- “Orthopedic injuries are among the most likely conditions to be missed in the ED” 1
- The extremity injuries discussed in this post are mostly clinical diagnoses and include:
- Knee Dislocation
- Extensor Mechanism Injury
- Compartment Syndrome
- Tibiofibular Syndesmosis Injuries
- Objectives:
- Increase awareness of 4 lower extremity injuries that are seen and sometimes missed in our EDs
- Develop an ED approach to these less common but serious MSK injuries
- Review the mechanism of injury, risk factors, physical examination, and management of these injuries with some clinical pearls
Knee Dislocation

Seroyer, et al. Management of the acute knee dislocation: the Pittsburgh experience. Injury. 2008;39:710–718.
- Tibiofemoral dislocation leads to tremendous ligamentous disruption 2
- Rare: 0.5% of joint dislocations, but potentially limb-threatening:
- Amputation rate 11 – 86 % 3
- Nerve injury 14 – 35 % 4
- Popliteal artery injury 5 – 65% 5
Review of the Literature
Medina, et al. Vascular and neve injury after knee dislocation: A sytematic review. Clin Ortho Relat Res. 2014;472:2621-2629.
- 862 patients with knee dislocations
- 171 sustained vascular injury
- Weighted frequency of 18%.
- 80% (134 of 160) of vascular injuries underwent repair
- 12% (22 of 134) of vascular injuries resulted in amputation
Natsuhara, et al. What is the frequency of vascular injury after knee dislocation. Clin Orthop Relat Res. 2014;472:2615–2620.
- 11 million orthopaedic patients (ICD-9 diagnostic codes for all knee dislocation 2004 to 2009)
- 8050 limbs with knee dislocation identified
- 267 had a concomitant vascular injury for an overall frequency of 3.3%
- 34 of the 267 cases (13%) underwent surgical treatment
- Largest study to date, with data suggesting lower frequencies of vascular injury associated with knee dislocation and a lower proportion undergoing surgical management
Risk Factors
- Male
- High velocity injuries (high energy hyperextension)
- Obesity (for ultra low velocity dislocations, falls from standing or walking)
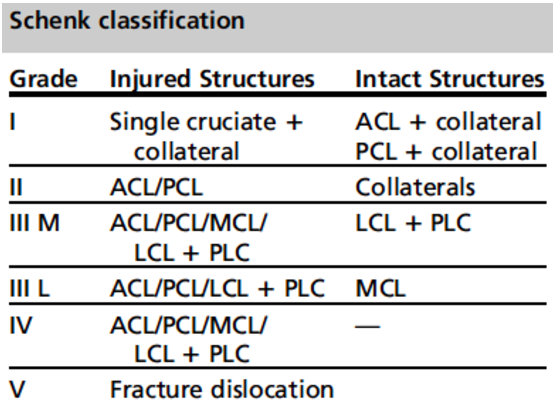
Classifying the injury:
- Schenk: structures injured
- Kennedy: direction of displacement
- Anterior most common (40%)
Lachman, et al. Traumatic knee dislocatons: Evaluation, management, and surgical treatment. Orthop Clin N Am. 2015; 46:479-493.
Physical Exam
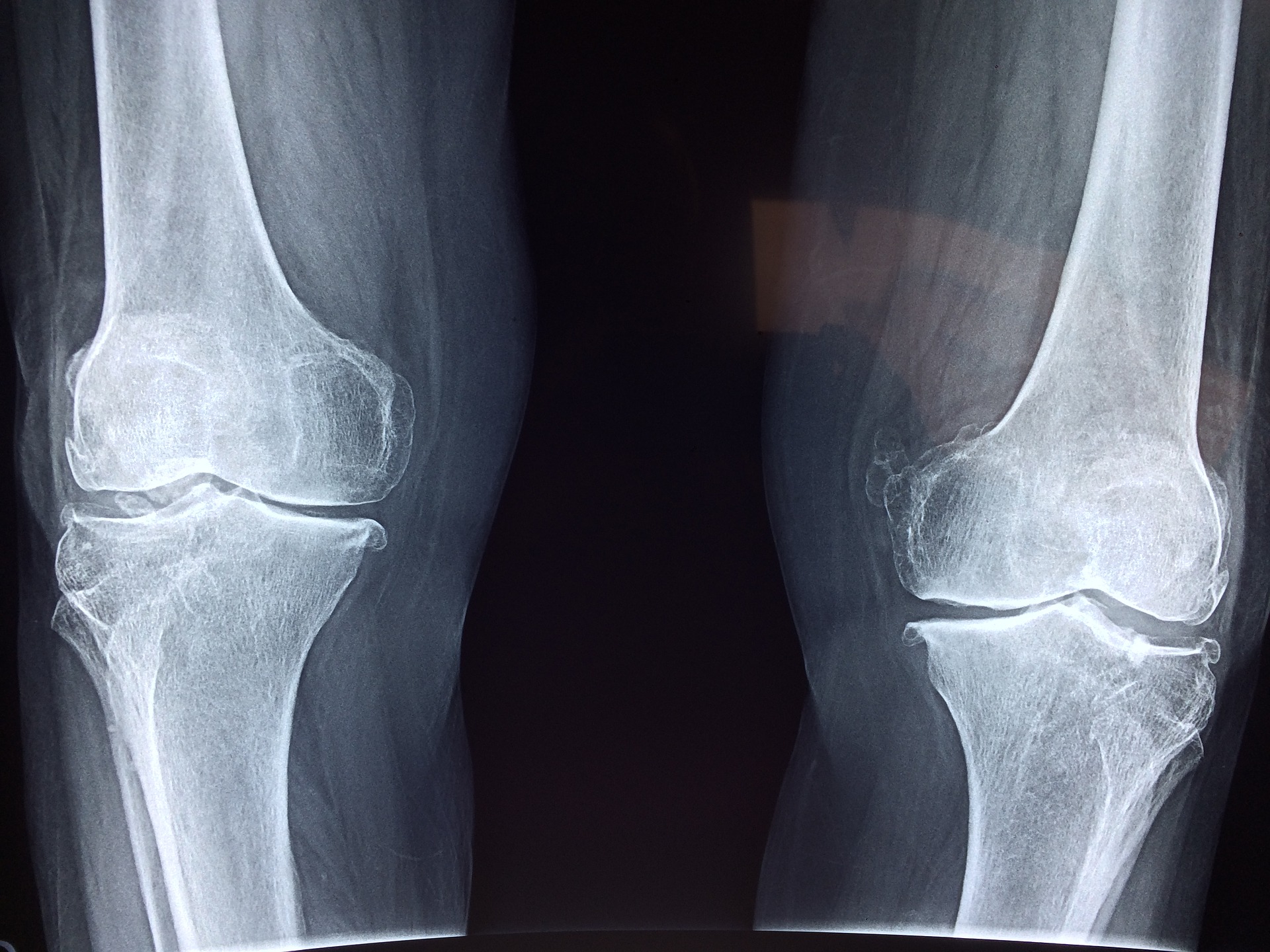
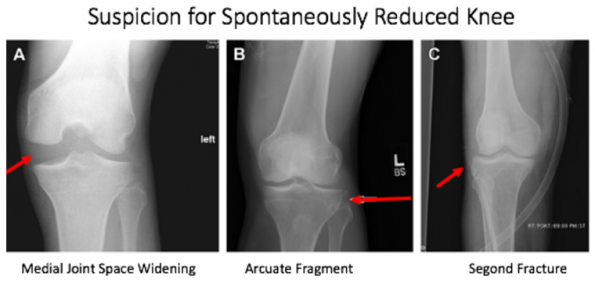
- Examination is key, ½ spontaneously reduce prior to ED arrival
- +/- Knee swelling
- Knee capsule is usually torn with injury, which allows an associated hemarthrosis to dissipate into surrounding tissues
- Buckling knee with foot drop
- Loose knee on exam
- Absent/asymmetric distal pulses
- Paresthesias
- Posterior sag sign
- Knee hyper-extends when examiner lifts the foot by the heel
- Dimple sign 7, 8
- Ankle-Brachial Index (ABI)
- < 0.9 100 % PPV
- > 0.9 100 % NPV
- +/- Knee swelling
Imaging
Lachman, et al. Traumatic knee dislocatons: Evaluation, management, and surgical treatment. Orthop Clin N Am. 2015; 46:479-493.
Management
- Serial physical exams and ABI in ED are key
- Vascular will decide further imaging modalities, such as angiography
- IF the knee has not reduced spontaneously, early reduction is key
Extensor Mechanism Injury
- Extensor mechanism:
- Quadriceps muscle and tendon
- Patella
- Patellar tendon
- Injury to any of these disrupts the extensor mechanism
- Highly disabling injury 11, 12
(1) Quadriceps Tendon Rupture
- 50% missed in ED 12
- ~ 1/3 of all extensor mechanism injuries 11
Risk Factors
- M > F (8:1)
- > 40 years: peak 6-7th decade
- Systemic disease: RA, SLE, connective tissue disease, chronic steroids
Physical Exam
- Active straight leg raise (when supine, patient actively lifting leg up) – Extensor lag
- Audible crepitus
- Palpable gap or suprapatellar mass 8, 13
Xray Findings
- The Low Patella = Patella Baja
- From joint line to patella should be approximately 1 finger breadth, lower than this, think baja
- Check contralateral side, may be a variant of normal
- Avulsion patellar fragment

- Patellar spur
- Suprapatellar calcification
Ultrasound
- Quick and cost-effective
- Quadriceps tendon is superficial
- Varying sensitivity and specificity in the literature
Management
- Partial
- Non-operative
- Immobilized ~ 6 weeks
- Complete
- Knee immobilizer
- Surgical management (timely) 8, 12, 14
(2) Patellar Tendon Rupture
The patellar tendon is the second strongest tendon in the human body, requiring a force of ~17.5 x body weight to rupture.
Associated injuries
- Tibial plateau fracture
- Meniscal tear
- Intra-articular ligament ruptures 12, 15
Risk Factors/Mechanism
- Unilateral
- < 40 years
- Knee flexed with quads contraction
- Steroid use, autoimmune disease 11, 16
Physical exam
- Straight leg raise/knee extension – Extensor lag
- Feel for gap, mobile patella
- Assess for associated fracture 8
X-ray Findings
- The High Patella = Patella Alta
- Patella should be approximately 1 finger breadth from joint line, above this = alta
- Focal intratendinous radiolucency (FIR)
- Sens 82.5, spec 95.2%
- Avulsion inferior pole patella
- Avulsion tibial tuberosity
- Infrapatellar fat pad disruption 15, 17, 18
Ultrasound
- Less sensitive and specific than quadriceps ultrasound
- False positives in obese and muscular patients
- Complete tear: Retracted, swelling, edge artefact, waviness 17, 19
Management
- Surgical
- Risk of re-rupture is high!
Compartment Syndrome
- Definition: Increased pressure in a confined space 20
- 3 categories:
- More contents in the compartment
- Less volume within the compartment
- External pressure 2
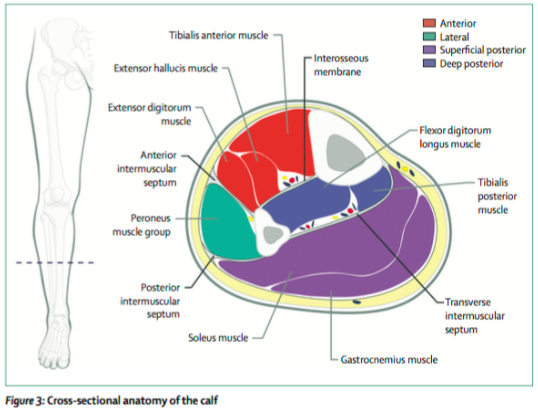
- The lower leg is the most common location of acute extremity compartment syndrome, with the anterior and lateral compartments more frequently affected.
- ~31-36% of acute extremity compartment syndrome = from tibial diaphysis fractures 21
- Compartment locations/contents:
Von Keudell AG, Weaver M, Appleton PT, Bae DS, Syer GSM, Jupiter JB, Vrahas MS. Emergency surgery 3: Diagnosis and treatment of acute extremity compartment syndrome. The Lancet. 2015; 286: 1299-1310.
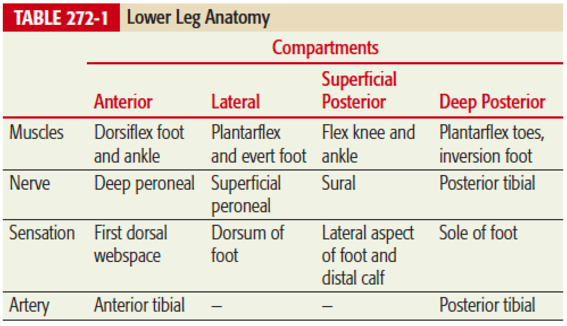
Tintinalli, et al. (2016). Emergency medicine: A comprehensive study guide (7th ed.) (p 1866). New York: McGraw-Hill, Medical Pub. Division.
Risk Factors
- M > F (10x if trauma)
- Young > old 21
Signs and Symptoms:
- “6 Ps”= pain, paralysis, paresthesia, pallor, pulselessness, poikilothermia
- “pain, pain, pain, …” – most important symptom
- Pain out of proportion
- Pain requiring increased analgesia
- Pain with passive stretch
- Paresthesias, hypoesthesias 24
- “pain, pain, pain, …” – most important symptom
Pressure Monitoring: General Principles
- Within 5 cm of fracture site
- Pain control
- Check all compartments involved
- Do not raise the affected limb above level of heart 22
The numbers:
- Normal pressures < 8 mm Hg (adults)
- First symptoms of ischemia 20 – 30 mm Hg
- Differential pressure: △P = Diastolic BP – intracompartmental BP ≤ 30 mm Hg 21, 22
Compartmental Pressure Monitoring
- High false positives associated with single measurement of pressure
- Continuous compartmental pressure monitoring not validated, not used frequently in Canada in lieu of clinical monitoring and serial physical exams
Management
- In the awake, mentating patient:
- History and clinical exam
- Early ortho involvement
- Indications for compartmental pressure monitoring:
- Unresponsive/uncooperative patient
- Multiple distracting injuries 25, 26
Tibiofibular Syndesmosis Injuries (the High Ankle Sprain):
Maisonneuve Fracture. wikiRadiography. n. d. photograph, viewed February 15, 2017 http://www.wikiradiography.net/page/Maisonneuve+Fracture
- A fibrous joint; complex between distal tibia and fibula
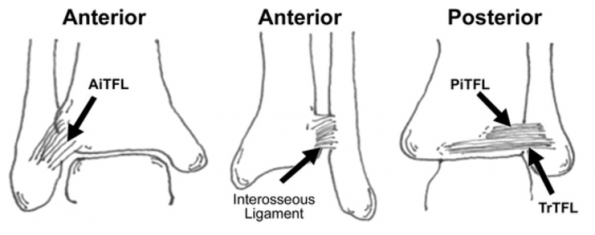
- Two bones plus 4 ligaments:
- Anterior tibiofibular ligament
- Interosseous ligament (IOL)
- Posterior inferior tibiofibular ligament (PITFL)
- Transverse tibiofibular ligament (TTL)
- Two bones plus 4 ligaments:
- Mechanism of Injury: External rotation + dorsiflexion ankle + eversion of talus 29
- ~20 % missed in ED 28
- 1-18% ankle sprains are high ankle sprains 30
Signs and Symptoms:
- ‘High ankle pain’ and anterolateral ankle pain
- Inability to weight bear or pain at push off
- Swelling proximal to ankle joint
- Pain with dorsiflex, external rotation 30, 31
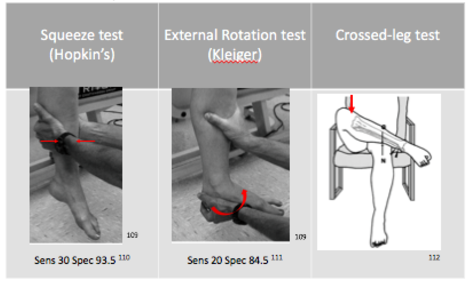
Physical Examination: Special Tests
X-ray Interpretation
- Measurements = 1 cm above tibial plafond
- Tibiofibular overlap
- Normal > 1 mm mortise
- Normal > 6 mm AP 30, 31
- Medial clear space
- Normal ≤ 4 mm 28, 30, 31
- Tibiofibular clear space
- Distance between lateral border of posterior tibial prominence and medial border of the fibula
- Normal < 5 – 6 mm
- Tibiofibular overlap
- Stress views (gravity or weighted) may be helpful to diagnose a syndesmotic injury 31, 33, 34
- High specificity but lower sensitivity

Tibiofibular overlap

Medical clear space
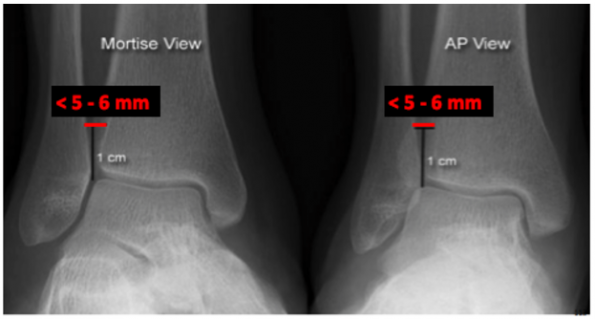
Tibiofibular clear space
Management
- No fracture, mild syndesmotic sprain (grade I)
- Conservative management
- Severe injuries (grade II – III)
- Surgical intervention
- Considered unstable 31, 33, 34
Summary
- Knee Dislocations:
- Beware the ultra-low velocity
- Perform physical exam including ABI + pulses
- Some X-ray associated features such as medial joint space widening, segond fracture, and an arcuate fragment may be present
- Extensor Mechanism Injuries:
- Perform an active straight leg raise in every patient with knee injury
- Assess gaps in the extensor mechanism
- Assess whether the patella is high or low riding
- Ultrasound is a good adjunct
- Compartment Syndrome:
- PAIN is the key feature
- Fractures are a common cause(tibial fractures 36%)
- Measuring compartment pressures:
- One-time use is associated with high false positives
- Continuous use is not validated
- Indications for use: unresponsive/uncooperative patient or multiple distracting injuries
- Key value with pressure monitoring is delta pressure: △P = Diastolic BP – intracompartmental BP ≤ 30 mm Hg
- Syndesmotic Disruption:
- Consider with EVERSION mechanism or if patient has Weber B or C fracture
- A combination of special tests can be helpful in physical examination and x=X-ray measurements are key:
- Tibiofibular overlap > 6 mm AP
- Medial clear space < 4 mm
- Tibiofibular clear space < 5-6 mm (AP & mortise)
References
References:
- Cross, C. Reducing missed orthopedic injuries in the ER. CMAJ January 7, 2014 186:E18; published ahead of print December 9, 2013, doi:10.1503/cmaj.109-4674.
- Marx, J. A., & Rosen, P. (2014). Rosen’s emergency medicine: Concepts and clinical practice (8th ed.). Philadelphia, PA: Elsevier/Saunders.
- Seroyer ST, Musahl V, Harner CD. Management of the acute knee dislocation: the Pittsburgh experience. Injury. 2008;39:710–718.
- Hegyes MS, Richardson MW, Miller MD. Knee dislocation. Complications of nonoperative and operative management. Clin Sports Med. 2000:19:519-43.
- Natsuhara, K.M., Yeranosian, M.G., Cohen, J.R. et al, What is the frequency of vascular injury after knee dislocation. Clin Orthop Relat Res. 2014;472:2615–2620.
- Medina O, Arom GA, Yeranosian MG, Petrigliano FA, McAllister DR. Vascular and neve injury after knee dislocation: A sytematic review. Clin Ortho Relat Res. 2014;472:2621-2629.
- Lachman JR, Rehman S, Pipitone PS. Traumatic knee dislocatons: Evaluation, management, and surgical treatment. Orthop Clin N Am. 2015; 46:479-493.
- Helman A.“Episode 91: Acute Knee Injuries Pearls and Pitfalls”. Emergency Medicine Cases, January 24, 2017, https://emergencymedicinecases.com/occult-knee-injuries/
- Mills WJ, Barei DP, McNair P. The value of the ankle-brachial index for diagnosing arterial injury after knee dislocation: a prospective study. J Trauma. 2004;56(6)1261-1265.
- Boyce RH, Singh K, Obremskey WT. Review: Acute management of traumatic knee dislocations for the generalist. J Am Acad Orthop Surg. 2015; 23:761-768.
- Tarazi N, O’loughlin P, Amin A,, Koegh P. Case report: A rare case of bilateral patellar tendon ruptures: A case report and literature review. Case Rep Orthop. 2016; 2016:6912968. doi: 10.1155/2016/6912968. Epub 2016 Apr 20.
- Pengas IP, Assiotis A, Khan W, Spalding T (2016) Adult native knee extensor mechanism ruptures. Injury. doi:10.1016/j.injury.2016.06.032
- Wheeless CR. Rupture of the Quadriceps. Wheeless’ textbook of orthopaedics, February 12, 2017, http://www.wheelessonline.com/ortho/rupture_of_the_quadriceps.
- Hak DJ, Sanchez A, Trobisch P. (2010) Review Article: Quadriceps tendon injuries. Orthopedics. doi: 10.3928/01477447-20091124-20.
- Ng JP, Cawley DT, Beecher SM, Lee MJ, Bergin D, Shannon FJ. Focal intertendinous radiolucency: A new radiographic method for diagnosing patellar tendon ruptures. The Knee. 2016; 23: 482-486.
- Garner MR, Gausden E, Berkes MB, Nugyen JT, Lorich DG. Extensor mechanism injuries of the knee: Demographic characteristics and comorbidities from a review of 726 patient records. J Bone Joint Surg Am. 2015; 97:1592-6.
- Berg K, Peck J, Boulger C, Bahner DP. Case Report: Patellar tendon rupture: An ultrasound case report. BMJ Case Rep. 2013. doi:10.1136/bcr-2012-008189.
- Fazal MA, Moonot P, Haddad F. Clinical Article: Radiographic features of acute patellar tendon rupture. Orthopedic Surgery. 2015;7:338-342.
- Swamy GN, Nanjayan SK, Yallappa S, Bishnoi A, Pickering SA. Is ultrasound diagnosis reliable in acute extensor tendon injuries of the knee? Acta Orthop Belg. 2012; 78(6) 764-70.
- Roberts JR, Hedges JR. (2015) Roberts and Hedges’ Clinical Procedures in Emergency Medicine (Roberts, Clinical Procedures in Emergency Medicine) (6th ed.)(p.1095). Philadelpia, PA: Elsevier/Saunders.
- Shadgan B, Menon M, Sanders D, Berry G, Martin C, Duffy P, Stephan D, O’Brien PJ. Current thinking about acute compartment syndrome of the lower extremity. Can J Surg. 2010;53(5) 329-334.
- Von Keudell AG, Weaver M, Appleton PT, Bae DS, Syer GSM, Jupiter JB, Vrahas MS. Emergency surgery 3: Diagnosis and treatment of acute extremity compartment syndrome. The Lancet. 2015; 286: 1299-1310.
- Tintinalli, J. E., Kelen, G. D., & Stapczynski, J. S. (2016). Emergency medicine: A comprehensive study guide (7th ed.) (p 1866). New York: McGraw-Hill, Medical Pub. Division.
- Raza H, Mahaptra A. Review article: Acute compartment syndrome in orthopedics: Causes, diagnosis and management. Advances in Orthopedics. 2015. http://dx.doi.org/10.1155/2015/543412.
- Whitney A, O’Toole RV, Hui E, Sciadini MF, Pollak AN, Manson TT, Eglseder A, Andersen RC, LeBrun C, Doro C, Nascone JW. Do one-time intracompartmental pressure measurements have
- Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: Are clinical findings predictive of the disorder? Journal of Orthopaedic Trauma. 2002; 16(8): 572-577.
- Maisonneuve Fracture. wikiRadiography. n. d. photograph, viewed February 15, 2017 http://www.wikiradiography.net/page/Maisonneuve+Fracture
- Helman A.“Episode 58: – Commonly Missed Uncommon Orthopedic Injuries, Part 2”. Emergency Medicine Cases, January 2015, https://emergencymedicinecases.com/episode-58-tendons-ligaments-missed-orthopedic-injuries/
- Schnetzke M, Vetter SY, Beisemann N, Swartman B, Grutzner PA, Franke J. Management of syndesmotic injruies: What is the evidence? World J Orthop. 2016; 7(11): 718-725.
- McCollum GA, van den Bekerom MPJ, Kerkhoffs GMMJ, Calder JDF, van Dijk CN. Syndesmosis and deltoid ligament injuries in the athlete. Knee Surg Sports Traumatol Arthosc. 2013; 21:1328-1337
- Lin CF, Gross MT, Weinhold P. Ankle syndesmosis injuries: Anatomy, biomechanics, mechanism of injury, and clinical guidelines for diagnosis and intervention. J Orthop Sports Phys Ther. 2006; 36(6): 372-384
- Kiter E, Bozkurt M. The crossed-leg test for examination of the ankle syndesmosis injuries. Foot and Ankle International. 2005; 26(2): 187-188
- Schock HJ, Pinzur M, Manion L, Stover M. The use of gravity or manual-stress radiographs in the assessment of supination-external rotation fractures of the ankle. J Bone Joint Surg. 2007; 89: 1055-1059.
- Sman AD, Hiller CE, Refshauge KM. Diagnostic accuracy of clinical tests for diagnosis of ankle syndesmosis injury: a systematic review. Br J Sports Med. 2013; 47: 620-628

