

The Canadian population is rapidly aging, and within the next 15 years, 1 in every 4 people will be 65 years or older 1. Elderly patients already make up 25% of Canadian Emergency Department (ED) visits, and this number is expected to increase 2. What should concern you about this trend is that:
- Older patients are also high risk for adverse outcomes, ED re-visits and hospitalization after discharge.
- In a Canadian meta-analysis, 30% of older patients seen in the ED bounced back within 3 months, and 10% died at 3 months 3.
Many institutions are fortunate enough to have access to Geriatric Emergency Management Nursing teams. Nevertheless, it is becoming more important for the Emergency physician to understand core issues that affect the assessment and management of older ED patients. In this post, we will review three key concepts related to older ED patients:
- Frailty
- Falls assessments
- Pain management
Frailty in the older ED patient
There is no commonly accepted definition in the literature for frailty; some authors think it refers to a physical phenotype of vulnerability to stressors, whereas other experts think it also includes social and psychological aspects 4. Basically, frailty represents a syndrome of decreased reserve and ability to resist stressors due to cumulative decline of multiple body systems. Frailty is not normal aging – it only represents a subset of older patients (up to 10% in outpatient studies and 20% in ED-based studies) 5-7.

The best known and cited criteria for frailty were set out by Fried and colleagues. In their system, patients need 3 of the following 5 criteria to be considered frail 7:
- Objective weakness (i.e. decreased grip strength)
- Slow gait
- Low levels of physical activity
- Subjective exhaustion
- Unintentional weight loss
Though unintentional weight loss is a criteria, older patients can also be obese and frail. In fact, in the Women’s Health and Aging Study, obese women were more likely to meet the other frailty indicators listed above than normal-weight women 8.
Now, you might still be wondering why Emergency physicians need to care about frailty. Actually, all medical providers should be concerned with frailty in older patients. Frailty is associated with a high risk of morbidity and mortality, independent of comorbidities or disability. Frail patients are at a 50% higher risk of falls and hip fracture, and their mortality is between 2 and 6 times higher over time than non-frail cohorts 5,9,10.
There are many tools in existence to quantify frailty and predict outcomes, though few have been validated or extensively studied in ED populations. Two tools that you should be aware of are the Clinical Frailty Scale (CFS) and the Study of Osteoporotic Fractures Frailty Index (SOF). The CFS was designed by Rockwood and colleagues from Halifax, and uses a 7-point scale to quantify frailty (revised version below). It has been used in some of the ED-based Canadian Emergency Departments Team Initiative (CETI) studies recently performed in our ED 9,11. The other tool, the SOF index, is a simple 3-point index that requires patients to have 2 of (1) subjective exhaustion, (2) objective weakness, and (3) unintentional weight loss > 5% to be considered frail. It has also been studied in the ED and is one of the more simple and accessible tools we have 12,13.
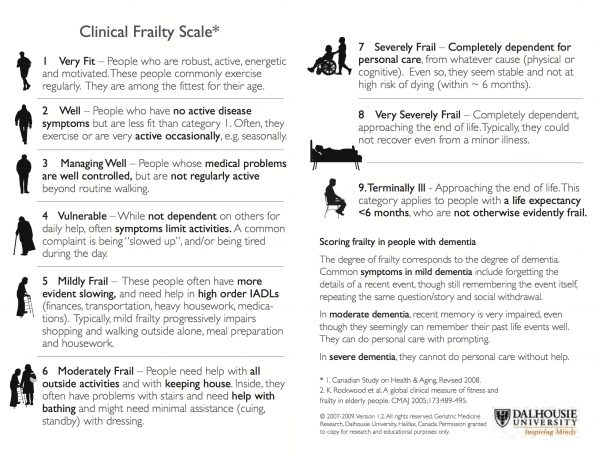
Geriatric Medicine Research, Faculty of Medicine, Dalhousie University. http://geriatricresearch.medicine.dal.ca/pdf/Clinical%20Faily%20Scale.pdf
Once we appreciate what frailty is and why it is important to recognize in the ED, we can intervene upon it in several ways. Frail or pre-frail patients should be considered for intensified community supports and programs. In addition, we should start thinking about what treatments are inappropriate for patients based on frailty. The Palliative and Therapeutic Harmonization (PATH) clinic in Halifax assesses patients and has made evidence-based recommendations on what treatments are not advised for frail patients; with our aging population, this type of approach will become increasingly important 14.
Falls in the older ED patient
Falls are a sentinel event in an older person’s life. Between 20-30% of Canadian seniors fall each year, and 2 of every 3 patients who fall are assessed in our EDs 15. The recent finding that the Champlain LHIN has the highest fall-related hospitalization rate in the province led to the institution of a comprehensive fall prevention strategy in the community. But what can we do in terms of falls assessment among our elderly ED patients?
First, start by asking yourself if the patient in front of you would have fallen if he or she was 20 years old 16? Many patients in our EDs are labelled as having a “mechanical” fall, but there are often modifiable causes of falls that we can, and should, identify.
For history, the following risk factors have been found to be predictive of falls specifically in ED populations 17–19:
- History of falls
- Poor foot care: inability to cut one’s toenails, non-healing foot sores
- Depression
- Multiple medications
For your physical exam, although orthostatic vitals have been much-maligned over the past several years, you should be looking for orthostatic hypotension or dizziness in your elderly falls patient. Orthostatic hypotension is associated with several of the medications that older patients may be taking and is associated with an approximately doubled risk of falls in outpatient studies 20,21.
Our professional societies recommend orthostatic vitals and a gait assessment as part of your standard falls assessment in the ED 16. For gait assessment, you can use the Timed Up-and-Go test, or a non-timed test if you prefer, but the most important take-away is that you should be watching the patient walk, instead of simply ordering it.
Pain Management in the older ED patient
Older patients with pain are unfortunately much more likely to be under-treated than our younger patients – in multiple studies, less than 50% of older patients received analgesia for their pain 22,23! In fact, untreated pain is more strongly associated with delirium than the opioids that we are so reluctant to prescribe in older patients. In one American study of inpatients with hip fracture, severe pain was very strongly associated with delirium, and patients who received the lowest total daily opioid doses were the most likely to be delirious 24.
Part of the problem may be that we have difficulty assessing pain in the older patient who is delirious or very demented and cannot communicate pain to us. Fortunately, there are tools to help us assess pain even in these patients, such as the PAIN-AD algorithm 25.
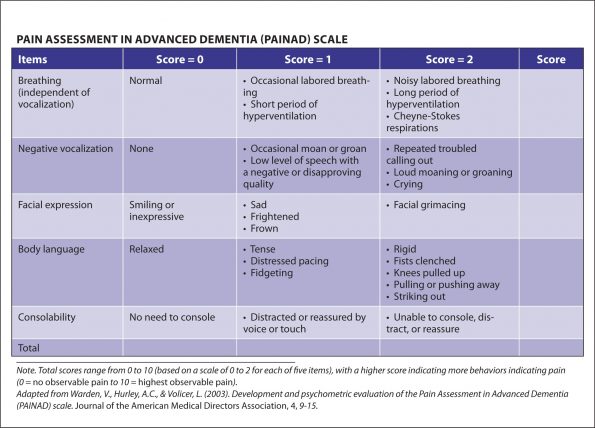
Pain Assessment in Advanced Dementia Cheat Sheet by Davidpol. Cheatography. https://www.cheatography.com/uploads/davidpol_1460700624_PainAD%20Scale.jpg
There are no ED-based guidelines on acute pain management in the elderly patient, but we can take useful recommendations from the Beers Criteria, produced by the American Geriatrics Society 26. In general, for our older ED patients:
- Acetaminophen should be first-line for foundational analgesia and should be prescribed at regular intervals
- Nonsteroidals should be used with caution
- Ketorolac is to be avoided due to its higher risk for gastric ulcers
- A short-term course of NSAIDs may be appropriate in the right patient (i.e. one who has no other contraindications to using NSAIDs)
- Opioids are the still standard of care for the older patient with severe, acute pain
- Doses should be reduced by 25-50%
- Consider the use of hydromorphone which does not have active metabolites that require renal clearance (as morphine does)
- While many of us seem to favour prescribing Tramadol, the side effects are stacking up against it (interaction with serotonergic medications, hypoglycemia, and others) 27
- Remember also that your opioid prescription should be accompanied by a bowel regimen
- Optimize local analgesics, for example nerve blocks for hip fracture, whenever appropriate
Summary: Recommendations
- Recognize that frailty is an actual independent syndrome, associated with high morbidity and mortality, and that we should both recognize and intervene upon it
- Take falls, even ones resulting in very minor injury, seriously in the older patient. Ask them about fall history, depression, and medications. Perform orthostatic vitals, and watch them walk as part of your assessment!
- Use validated tools (PAIN-AD/FACES) to assess pain even in very demented or delirious patients and explore your options for pain management – including low-dose opioids for moderate to severe pain
References
- Statistics Canada. Population Projections: Canada , the Provinces and Territories , 2013 to 2063.; 2014.
- Canadian Institute for Health Information. Emergency Department Visits in 2014 – 2015.; 2015.
- Aminzadeh F, Dalziel WB. Older adults in the emergency department: A systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med. 2002;39(3):238-247. doi:10.1067/mem.2002.121523.
- Rockwood K. Frailty and its definition: A worthy challenge. J Am Geriatr Soc. 2005;53(6):1069-1070. doi:10.1111/j.1532-5415.2005.53312.x.
- Ensrud KE, Ewing SK, Taylor BC, et al. Frailty and risk of falls, fracture, and mortality in older women: The study of osteoporotic fractures. Journals Gerontol – Ser A Biol Sci Med Sci. 2007;62(7):744-751. doi:62/7/744 [pii].
- Salvi F, Morichi V, Grilli A, et al. Screening for frailty in elderly emergency department patients by using the identification of seniors at risk (ISAR). J Nutr Heal Aging. 2012;16(4):313-318. doi:10.1007/s12603-011-0155-9.
- Fried L, Tangen C, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol. 2001;56A(3):M146-M156.
- Blaum CS, Xue QL, Michelon E, Semba RD, Fried LP. The association between obesity and the frailty syndrome in older women: The Women’s Health and Aging Studies. J Am Geriatr Soc. 2005;53(6):927-934. doi:10.1111/j.1532-5415.2005.53300.x.
- Provencher V, Sirois MJ, Ouellet MC, et al. Decline in activities of daily living after a visit to a Canadian emergency department for minor injuries in independent older adults: Are frail older adults with cognitive impairment at greater risk? J Am Geriatr Soc. 2015;63(5):860-868. doi:10.1111/jgs.13389.
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. 2004;59(3):255-263. doi:10.1093/gerona/59.3.M255.
- Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489-495. doi:10.1503/cmaj.050051.
- Ensrud KE, Ewing SK, Taylor BC, et al. Comparison of 2 Frailty Indexes for Prediction of Falls, Disability, Fractures, and Death in Older Women. Arch Intern Med. 2008;168(4):382-389. doi:10.1001/archinternmed.2007.113.
- Sirois M-J, Griffith L, Perry J, et al. Measuring Frailty Can Help Emergency Departments Identify Independent Seniors at Risk of Functional Decline After Minor Injuries. J Gerontol A Biol Sci Med Sci. 2015;72(1):glv152-. doi:10.1093/gerona/glv152.
- Moorhouse P, Mallery LH. Palliative and therapeutic harmonization: A model for appropriate decision-making in frail older adults. J Am Geriatr Soc. 2012;60(12):2326-2332. doi:10.1111/j.1532-5415.2012.04210.x.
- Public Health Agency of Canada. Seniors’ Falls in Canada: Second Report: Key Highlights.; 2014.
- ACEP. Geriatric Emergency Department Guidelines. 2013.
- Carpenter CR, Avidan MS, Wildes T, Stark S, Fowler SA, Lo AX. Predicting Geriatric Falls Following an Episode of Emergency Department Care: A Systematic Review. Acad Emerg Med. 2014;21(10):1069-1082. doi:10.1038/jid.2014.371.
- Carpenter CR, Scheatzle MD, D’Antonio JA, Ricci PT, Coben JH. Identification of fall risk factors in older adult emergency department patients. Acad Emerg Med. 2009;16(3):211-219. doi:10.1111/j.1553-2712.2009.00351.x.
- Tiedemann A, Sherrington C, Orr T, et al. Identifying older people at high risk of future falls: development and validation of a screening tool for use in emergency departments. Emerg Med J. 2013;30(11):918-922. doi:10.1136/emermed-2012-201783.
- Ooi WL, Hossain M, Lipsitz LA. The association between orthostatic hypotension and recurrent falls in nursing home residents. Am J Med. 2000;108(2):106-111. doi:10.1016/S0002-9343(99)00425-8.
- Momeyer MA. Orthostatic hypotension in older adults with dementia. J Gerontol Nurs. 2014;40(6):21-22. doi:10.3928/00989134-20140421-01.
- Hwang U, Platts-Mills TF. Acute Pain Management in Older Adults in the Emergency Department. Clin Geriatr Med. 2013;29(1):151-164. doi:10.1016/j.cger.2012.10.006.
- Platts-Mills TF, Esserman DA, Brown DL, Bortsov A V, Sloane PD, McLean SA. Older US emergency department patients are less likely to receive pain medication than younger patients: results from a national survey. Ann Emerg Med. 2014;60(2):199-206. doi:10.1016/j.annemergmed.2011.09.014.
- Morrison RS, Magaziner J, Gilbert M, et al. Relationship between pain and opioid analgesics on the development of delirium following hip fracture. Journals Gerontol – Ser A Biol Sci Med Sci. 2003;58(1):76-81. doi:10.1093/gerona/58.1.M76.
- Warden V, Hurley AC, Volicer L. Development and Psychometric Evaluation of the Pain Assessment in Advanced Dementia (PAINAD) Scale. J Am Med Dir Assoc. 2003;4(1):9-15. doi:10.1097/01.JAM.0000043422.31640.F7.
- Samuel MJ. American Geriatrics Society 2015 Updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227-2246. doi:10.1111/jgs.13702.
- 27. Fournier J-P, Azoulay L, Yin H, Montastruc J-L, Suissa S. Tramadol use and the risk of hospitalization for hypoglycemia in patients with noncancer pain. JAMA Intern Med. 2015;175(2):186-193. doi:10.1001/jamainternmed.2014.6512.

