


For other ultrasound focused cases please see our Ultrasound Archives.
A woman in her 60’s presents to the emergency department on her 7th post-operative day feeling nauseous, vomiting, weak and dizzy. She has just recently underwent a open left hemi-colectomy, end-colostomy formation for recurrent diverticulitis. . Her past medical history is only significant for type 2 diabetes, and her only medications are ASA and metformin.
On initial presentation to the ED her examination is as follows:
Temp 36.7. BP 75/53. HR 107. Sa02 98% on RA. RR 16
GENERAL: Awake, alert and oriented X3. No acute distress
CVS: JVP (flat) N S1+S2, no EHS, II/VI SEM at the upper sternal borders, Trace peripheral edema.
RESP: chest clear
ABD: Soft, tender diffusely, non-distended. Colostomy bag in place filled with normal stool and gas.
Extremities: warm, perfused, trace edema
Investigations are ordered and resuscitation is started with intravenous fluids.
What’s your differential?
Now is the time to consider your differential for this patient. She is post-op day 7 from a large, open intra-abdominal surgery presenting hypotensive and tachycardic. Go through your differential for SHOCK.
- Distributive
- Sepsis: has to be ruled out in this patient. Likely sources include intra-abdominal, urinary, pulmonary.
- Neurogenic: unlikely in this patient
- Adrenal: has she been on long-term steroids and was not stress dosed? She hadn’t, but need to think of this as a cause.
- Anaphylactic: No physical signs of anaphylaxis, no recent new medications other than the antibiotics she got pre-operatively.
- Toxicological: No new medications or exposures.
- Hypovolemic
- Hemorrhage: She’s post-operative day 7. Possible, but unlikely to occur this late.
- Fluid losses from vomiting, high output stoma: stoma output normal, minimal vomiting
- Obstructive
- Massive PE: potentially. No chest pain but needs to be high on the differential.
- Tamponade
- Pnemothorax
- Cardiogenic
- Perioperative MI
- Myocarditis
- Cardiomyopathy
- Malignant dysrhythmia
Due to her recent surgery, intra-abdominal sepsis is thought to the be the most likely diagnosis. She is started on broad-spectrum antibiotics, given IV fluids and an abdominal CT scan is ordered.
Her initial labs are as follows:
CBC: WBC 20.9, Hgb 96, Plt 524
Electrolytes and Renal Function: Na 139, K 4.8, Urea 6.7, BUN 63
Lactate 1.6
Venous Gas: 7.43, pCO2 41, HCO3 28
LFT, lipase and TSH NORMAL
Blood Cultures x 2 sent
Urine dip NEGATIVE
A troponin is ordered, but unfortunately it is not recognized and not completed.
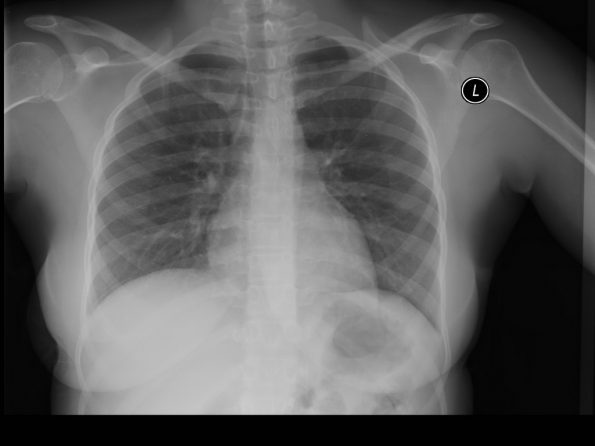
CXR:
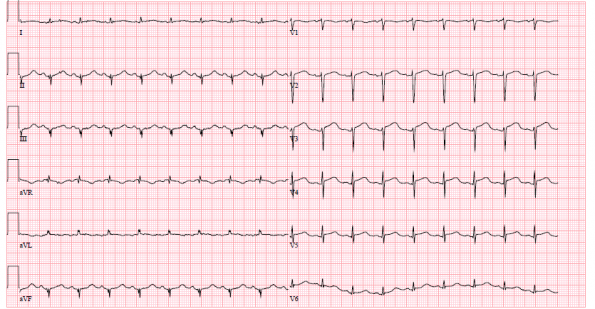
ECG:
Case Progression
The patient is handed over to the evening team. Her vitals improved to HR 94, BP 85/60, RR16, SpO2 94%, T 36.7. She is awaiting a CT scan of her abdomen to assess for closed loop obstruction or intra-abdominal abscess. The general surgery team is aware and are coming to assess. She has ongoing fluids ordered. Follow up on the CT scan.
The evening team goes on about their shift, seeing other patients. Unfortunately, after multiple fluid boluses the attending nurse is unable to raise the patient’s blood pressure any higher than 85-90 systolic. Pre-operatively the patient was known to have uncontrolled HTN. She is unable to get a hold of the general surgery team because they are busy with a big case in the OR. She, therefore, asks the evening team to take another look at the patient and review the CT report.
CT abdomen/pelvis:
1. Status post partial colectomy with an end colostomy in the left lower quadrant. No visible residual obstruction.
2. Mild inflammatory changes in the transverse colon leading to the ostomy, likely postoperative inflammation. No visible abnormal enhancement.
3. Trace volume ascites in the peritoneum.
No intra-abdominal source, no pulmonary source, no urinary source. Maybe this isn’t sepsis. At this point a focussed point-of-care ultrasound is done to determine the cause of this patient’s undifferentiated shock.
The RUSH Exam
First introduced by Scott Weingart et al. in 2006, the RUSH protocol is designed to rapidly assess and diagnose medical patients in undifferentiated shock. It consists of three components1–3:
- Evaluation of the TANK (the fluid status)
- The PIPES (the vessels)
- The PUMP (the heart)
It can be completed using the acronym HI-MAP
- Heart
- IVC
- Morrison’s pouch/FAST
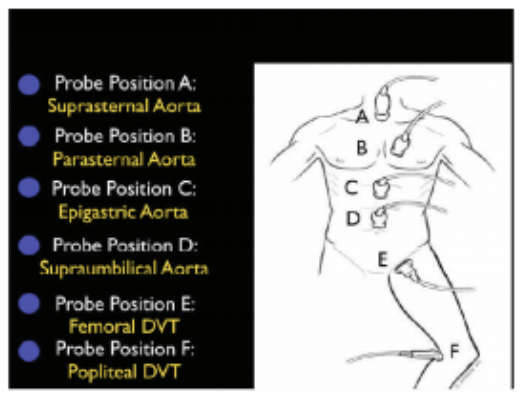
- Abdominal Aorta
- Pulmonary/Pneumothorax
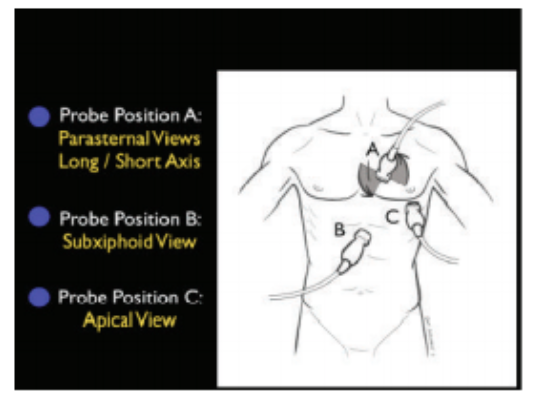
Evaluation of the PUMP1 |
 |
Evaluation of the TANK1 |
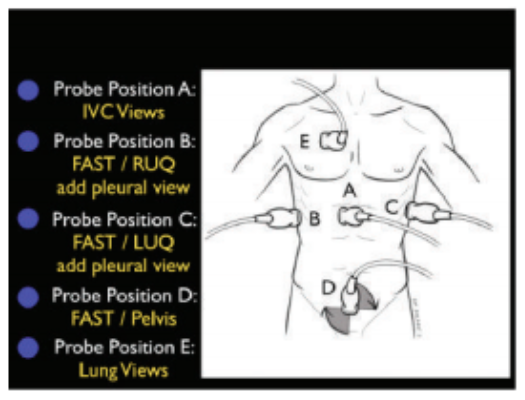 |
Evaluation of the PIPES1 |
 |
On to the bedside scan!
The cardiac views for this patient are as follows, attempt to generate an interpretation and next steps.
PSLA
PSSA
A4C
These images demonstrate regional wall motion abnormalities in the septum and the apex of the heart. It also appears to show dynamic obstruction of the LVOT via the contracting myocardium.
How does this change our management in this situation?
With this new information, you have to be thinking of cardiac ischemia, specifically ischemia in the territory of the LAD. If you find the territories of the coronary vessels difficult to recall, use this colour coded diagram on your next shift:
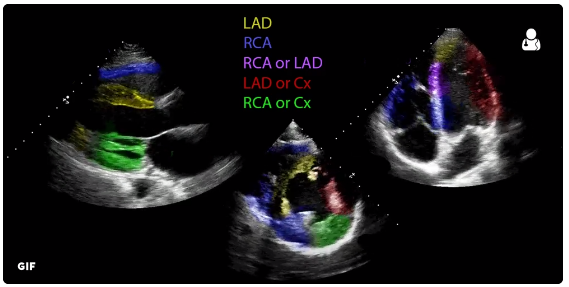
Reproduced with permission from https://twitter.com/UltrasoundJelly/status/855469000465285120
Image and gif produced by Dr. Ben Smith of ultrasoundoftheweek.com.
As you can see above, of all the views the parasternal short angle is the highest yield, considering it demonstrates almost all vessel territories.
In our patient, however, if you look closely you can also see some akinesis at the apex of the right ventricle as well, which is not in keeping with a LAD lesion. Considering the akinesis appears to be mostly apical one could consider a stress-induced or Takotsubo cardiomyopathy as well.
What’s the TNI?
With the new POCUS findings a set of cardiac biomarkers were ordered which returned at 4320 ng/L. In lieu of general surgery, cardiology was asked to urgently assess the patient. The report of their POCUS exam reported a hyperdynamic base, apical akinesis to dyskinesis and there appears to be a gradient across the LVOT/hyperdynamic base. She was treated with ASA, clopidogrel and metoprolol and admitted for urgent cath.
Case Resolution
Coronary catheterization demonstrated only 30% stenosis of the distal LAD without any other coronary irregularities. LVEF by ventriculography demonstrated severely reduced LV function at around 25%. On echocardiogram, LVEF estimated at 55% with apical akinesis consistent with Takotsubo cardiomyopathy. The patient was maintained on cardio-protective agents however blood pressure remained low throughout her stay.
Discussion
This case demonstrates the utility of POCUS in undifferentiated hypotension. If a patient is not responding to IV fluids or usual resuscitative maneuvers the next step is to assess for a cause. This does not need to be the entire RUSH exam every time however taking a look at the heart, the IVC and generating a pulmonary baseline is always useful in these patients. For this patient in particular, cardiac POCUS completely changed her management and she was able to be re-directed to the appropriate service for ongoing care.
This case also highlights the fragility and perilousness of the ED handover and the importance of structured handover tools, handover preparation and careful review of each handed over patient.

