
In this post, we’ll explore the many exciting applications that concepts borrowed from industrial engineering can have on ED efficiency and workflow. To help build a framework for further discussion, we will define industrial engineering, describe the ED as a complex system, and finally highlight applications of industrial engineering in the ED.
Industrial Engineering
The branch of engineering which deals with the optimization of complex processes, systems, or organizations. Industrial engineers work to eliminate waste of time, money, materials, person or machine-hours, energy, or any resource that does not generate value.
Complex System
A complex system is one that involves many components interacting amongst each other, so that the behaviour of each is dependent upon their interactions.
Engineering the Emergency Department
1. Human-Machine Integration
The purpose of which is human and machine interacting efficiently to serve a common purpose.
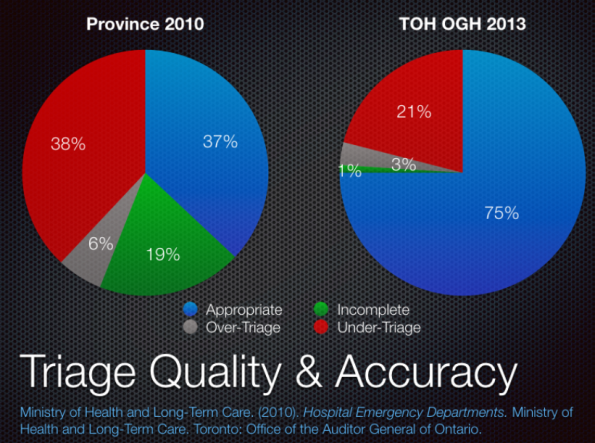
As a particular example, electronic triage has been proposed as a way of combating provincial audits showing mistriage rate and a significant number of triage reports being illegible or incomplete. Research from the University of Alberta has demonstrated that electronic triage support tools were reliable (Dong et al., 2006) and potentially more accurate (Dong et al., 2005) in comparison to expert nurse triage auditors. The provincial government commissioned the development of an electronic triage support tool, titled eCTAS, under the guidance of Cancer Care Ontario. Initial reports from this show an increase in inter-rater reliability from 73% to 93% and a decrease in the under-triage rate from 13% to 3%. Triage times increased by approximately 1.2 minutes per patient (Cancer Care Ontario, 2017). The government subsequently hopes to have all hospitals implementing eCTAS by the end of 2018.
2. Workflow Design
Workflow design is a series of tasks to produce a desired outcome, usually involving multiple participants and several stages in an organization.
Analyzing the process steps that a patient flows through in the ED helps to identify areas for improvement. We have already done this in a number of time-sensitive diagnoses like stroke and sepsis. Since the research surrounding the utility of tPA, stroke workflow has changed significantly. Time to treatment has been improved by having EMS patching and bypassing to stroke centres, “code stroke” paging protocols in hospitals, holding CT scanners for stroke patients, and taking measures to improve time to tPA delivery throughout the hospital. This has resulted in significant improvements in time-to-MD assessment and time-to-tPA.
3. Process Automation
To decrease human workload, technology-enabled automation of business processes allows an increase in service quality, improved safety, and constraint of costs.
Computer-based Physician Order Entry (CPOE) is slowly becoming the standard of most hospital functions. This represents an example of process automation, as it removes nursing workload for commonly ordered things such as medication, blood work, and imaging, and results in improved efficiency and safety. The impacts that automating this process has on nursing workflow is shown here:
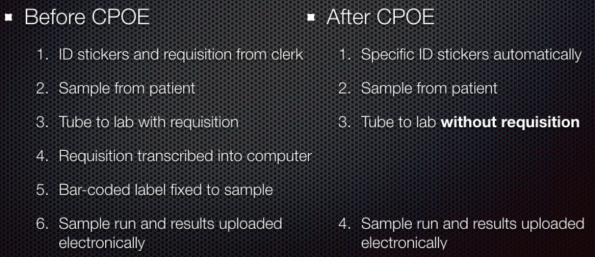
Research has varied in showing improved efficiency, with some studies demonstrated decreased times to physician-ordered medications by ~25 minutes, but increased times to physician-ordered blood work and imaging results by ~5-10 minutes, respectively (Syed, 2013). Other large studies have looked at overall ED length of stay, with some showing an impressive ~20-minute decrease (Spalding, 2011).
4. Capacity Planning
Capacity planning considers the production capacity needed by an organization to meet changing demands for its products.
Capacity planning is a critical step in deciding how to invest healthcare dollars within the hospital infrastructure. Short stay units (SSUs) have been proposed as a means of containing health care costs, buffering admitted patients from the ED, or avoiding admission to hospital. Many institutions use these SSUs differently and as such, the research surrounding them is quite heterogeneous. Most research seems to confirm that they are cost effective, but results vary as to ED length of stay (Galipeau, 2015).
The size of the SSU and how it functions within the hospital have important implications on its utility. Some act as overflow wards and others act as observation units for ED patients. Some industrial engineers have attempted to model the effect of implementing an SSU in a theoretical hospital (Zonderland, 2015):
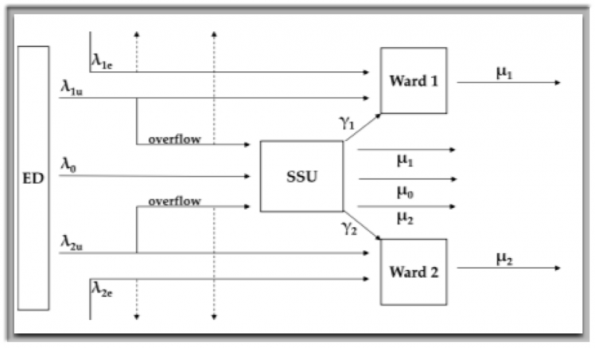
In this model, admission rates for both elective and urgent patients (λe and λu) of both medical (Ward 1) and surgical (Ward 2) patients are added along with the average length of stay for these patients (μ1 and μ2). The output studied was the effect on annual elective and urgent admissions to the hospital. Unsurprisingly, adding capacity for urgent admissions from the ED decreased the capacity for elective admissions, as there are now more of these patients competing for the available ward beds. The size of the SSU impacted the admissions as below:

Using mathematical modeling to predict the utility and impact of an SSU is a critical step that should be undertaken before adding this to a hospital.
5. Staff Scheduling & Optimization
The process of arranging, controlling, or optimizing work and workloads in a production process.
Traditionally, determination of nursing requirements has been made based on the size and volume of a particular department. Often, nursing ratios exist as a way of ensuring safety within the patient care setting, varied by level of monitoring required. A group out of Switzerland (Graff et al, 2016) looked at a new model whereby they devised a formula to calculate nursing need using both volume and acuity. They first calculated how much nursing time was required to care for a patient at each triage level and then mapped out how many patients arrived by hour, broken down by triage level. Using this equation, they were able to calculate the nursing needs for any given hour on any given day, using the data they input. This was extrapolated to predict the nursing needs of this particular 20,000 patient/year department for a given year.
Conclussions
Industrial engineering is an important concept and consideration for improving optimization and flow in the Emergency Department. Increasing technologies may improve effiency and effectiveness of healthcare delivery, however, they need to be implemented appropriately, with careful consideration of workflow designs and process mapping.
References
- Ministry of Health and Long-Term Care. (2010). Hospital Emergency Departments. Ministry of Health and Long-Term Care. Toronto: Office of the Auditor General of Ontario.
- Dong, S., Bullard, M., Meurer, D., Blitz, S., Ohinmaa, A., Holroyd, B., et al. (2006). Reliability of Computerized Emergency Triage. Academic Emergency Medicine, 13(3), 269-275.
- Dong, S., Bullard, M., Meurer, D., Colman, I., Blitz, S., & Holroyd, B. R. (2005). Emergency Triage: Comparing a Novel Computer Triage Program with Standard Triage. Academic Emergency Medicine, 12(6), 502-507.
- Galipeau, J., Pussegoda, K., Stevens, A., Brehaut, JC., Curran, J., Forster, AJ. (2015). Effectiveness and Safety of Short-stay Units in the Emergency Department: A Systematic Review. Academic Emergency Medicine; 22(8): 853-907.
- Zonderland, M., Boucherie, R., Carter, M., Stanford, D. (2015). Modeling the effect of short stay units on patient admissions. Operations Research for Health Care: 5, 21-27.
- Rabenu, E., Aharoni-Goldenberg, S. (2017). Understanding the Relationship between Overtime and Burnout, International Studies of Management & Organization, 47:4, 324-335.
- Graff, I., Goldschmidt, B., Glien, P., Klockner, S., Erdfelder, F., Schiefer, J., et al. (2016). Nursing Staffing Calculation in the Emergency Department – Performance-Oriented Calculation Based on the Manchester Triage System at the University Hospital Bonn. PLoS ONE, 11(5), 1-11.
- Turcotte, S. (2017, August 1). ED Arrival Pattern. ED Arrival Pattern . Ottawa, Ontario, Canada: The Ottawa Hospital.
- Ontario Nurses Association. (2017). Collective Agreement. Ontario Nursing Association.

