

In this post, we take a deep dive into the ever-present issue of ED crowding, going beyond the basic input-throughput-output model and focusing on institutional and provincial strategies for managing patient flow and overcrowding. We will cover the following objectives:
- Going beyond input – throughput – output: Understanding ED crowding and contributors
- It’s not just us: Provincial initiatives and solutions in Ontario
- Boots on the ground: Discuss personal strategies on how to function safely and still teach in a crowded department
ED crowding harms and kills patients
- Bernstein et al. (2009) is a review article that examined 41 studies on ED crowding.1 Highlights of the paper include that ED crowding is associated with:
- Delays in antibiotics administration
- Delays in analgesia, and
- Decreased patient satisfaction
- Pines (2018) found higher rates of heart failure, hypotension, and dysrhythmias in AMI patients presenting to the ED during a period of crowding.2
- Sprivulus et al. (2006) and Richardson (2006) are two Australian studies which showed increased mortality in periods of ED crowding.3,4
- In Ontario, Guttmann (2011) highlighted an increased mortality in discharged patients during periods of crowding.5
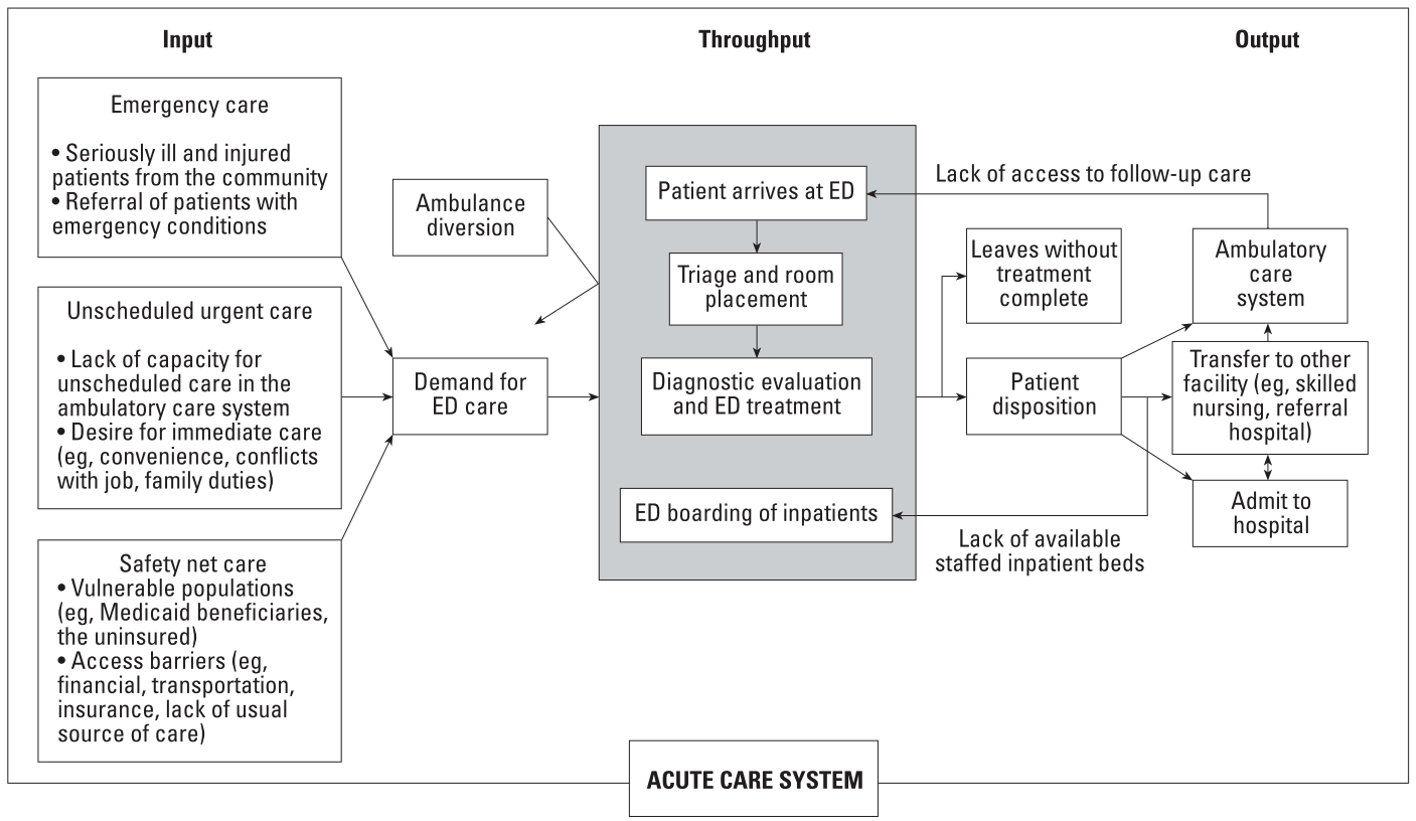
Input – Output – Throughput
• Created in 2003 by Asplin et al. as a framework to conceptualize contributors to ED crowding.6
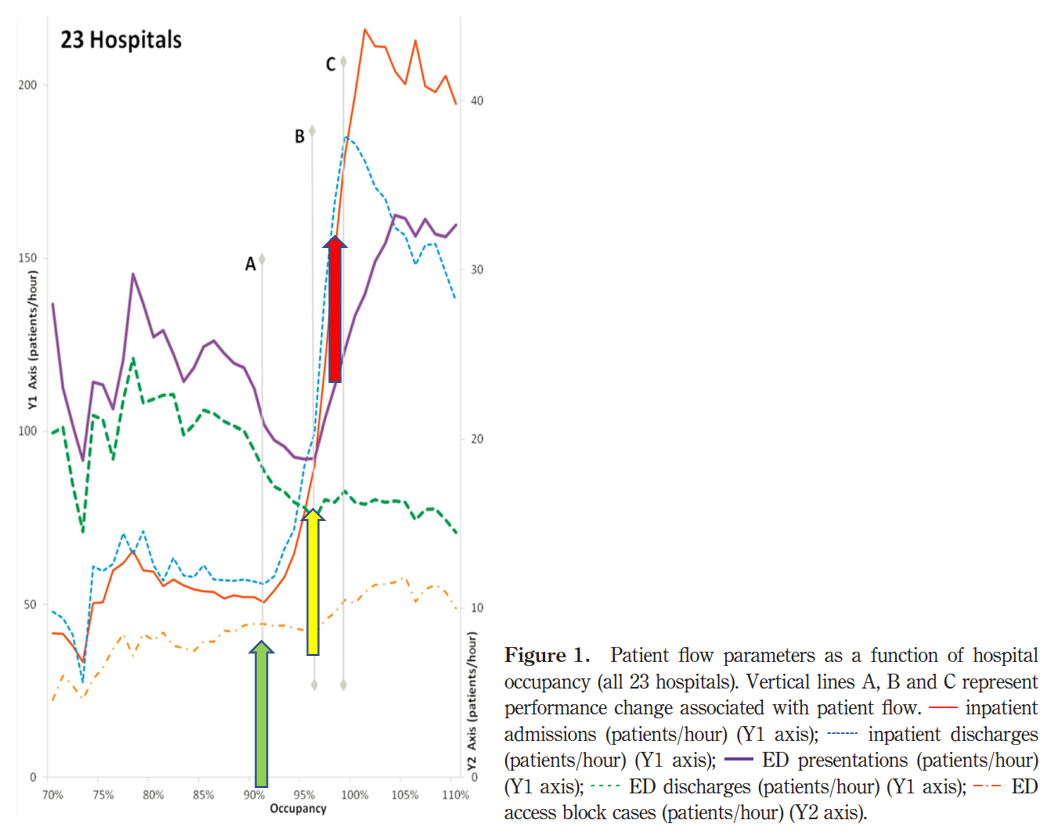
- There appear to be “tipping points” where ED throughput is significantly affected.
- Khanna et al. 2012 showed three separate “choke points” where hospital capacity had significant impact on crowding:7
- 91% hospital capacity “Chokepoint A”:
- Drastic increase in inpatient admissions and discharges
- 96% hospital capacity “Chokepoint B”:
- Drastic increase in ED LOS due to increasing ED presentations and decreasing ED discharges (AKA. A crowded ED)
- 99% hospital capacity “Chokepoint C”:
- Inpatient discharges drop off relative to inpatient admissions (AKA. A crowded hospital)
- 91% hospital capacity “Chokepoint A”:
- Khanna et al. 2012 showed three separate “choke points” where hospital capacity had significant impact on crowding:7
It’s not just us: Ontario ED Crowding
- In 2008, the Ministry of Health in Ontario introduced $500 million over three years to realign incentives to address healthcare performance metrics across the province.
- Dr. Alan Hudson, one of the architects of the plan, described it as “Data, Money, and Shame:”8
- Data: Monthly reports by hospitals to the government on health performance metrics
- Money: “Pay 4 Results” was introduced → Hospitals were given incentives for meeting certain governmental targets
- Shame: Hospital performance was publicly reported and ranked against other participating hospitals
- Initiatives in Ontario to address ED crowding include:
- Input:
- Family Health Teams with After Hours clinics
- Has not been shown to decrease ED visits. In fact, these patients present more to the ED than comparable Fee-For-Service patients.9
- Telehealth
- Family Health Teams with After Hours clinics
- Input:

- Throughput:
- Pay 4 Results
- Shown to have modest improvement on ED crowding without affecting patient care10
- Clinical Decision Units (CDU)
- Decreased LOS in CDU group by approx. 10 minutes11
- Decreased admission rates in CDU group11
- Rapid Assessment Zones
- Ambulance offload nurses
- Dynamic staff scheduling
- Pay 4 Results
- Output:
- Most hospitals in Canada function at greater than 95% capacity. This results in a persistent shortage of inpatient beds causing prolonged waiting periods in the ED for admitted patients to go to the floor.12
- Many of those inpatient beds are occupied by ALC patients waiting for space in long term care (LTC) facilities or rehabilitation programs. In Ontario, ALC patients occupy 13.7% of all “total inpatient days” in the hospital.13
- ALC patients are 6.6x more expensive than LTC patients ($842/day vs. 126$/day).14
- Barriers to building more Long Term Care facilities15
- Construction cost inflation exceeding funding initiatives
- 50% of current LTC beds require renovations or rebuilds
- Municipal fees can be up to $35,000 per bed/suite
Boots on the Ground
• Seven Strategies for managing a busy emergency department:16
 |
Managing Risk → Tailor investigations to risk stratification of patients and ensure that it will affect your management. Utilize clinical decision rules to defend decisions where applicable. |
 |
Communicate with patients → Make multiple quick visits with the patient for updates, especially if they will likely be discharged. This allows you to plant the idea early for them to get used to it. Utilize patient handouts. |
 |
Consultant Professionalism → Get to know your consultants. Be clear, concise, and appropriate to build up a bank of goodwill. |
 |
Monitor Department Flow → Communicate with your Charge Nurse regularly. Ensure “Direct to service” patients do not languish in your ED for extended periods of time. Prioritize reassessments that will affect disposition. |
 |
Manage your Time → Consider doing procedures at the end of your shift. Write your chart in the room while you are taking the history. |
 |
Be an Administrator and Delegator → Get to know your ED staff. Delegate tasks to allied healthcare when possible. Keep shifts for clinical work and clinical teaching, don’t perform other administrative or academic duties while on shift. |
 |
Some patients can’t be rushed → Be prudent with Chest Pain, Foreign Bodies, and Fractures. Additionally, be careful with patients who have bounced back to the ED or have been handed over. |
Strategies to Teach in a Crowded ED:
- ED STAT! is a framework developed to enhance clinical teaching on shift specifically for Emergency Physicians
- https://www.researchgate.net/publication/255629927_Welcome_to_ED_STAT_Strategies_for_Teaching_Any_Time
- Announce the teaching moment, empower the learner to develop their own learning objectives, and build teaching files to be able to provide high level teaching with minimal effort (after the creation of the file itself).17
Closing Thoughts
“Perhaps the greatest barrier to solving ED overcrowding is an attitude of nihilism, that nothing can be done. Efforts at the individual unit and hospital level to improve flow are to be supported, reported, and celebrated.” –Dr. H. Ovens8
References
1. Bernstein SL, Aronsky D, Duseja R, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med. 2009;16(1):1-10. doi:10.1111/j.1553-2712.2008.00295.x.
2. Pines JM, Pollack C V, Diercks DB, Chang AM, Shofer FS, Hollander JE. The Association Between Emergency Department Crowding and Adverse Cardiovascular Outcomes in Patients with Chest Pain. doi:10.1111/j.1553-2712.2009.00456.x.
3. Sprivulis PC, Da Silva J-A, Jacobs IG, Frazer ARL, Jelinek GA. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust. 2006;184(5):208-212. http://www.ncbi.nlm.nih.gov/pubmed/16515429. Accessed March 15, 2018.
4. Richardson DB. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust. 2006;6(5). https://search-proquest-com.proxy.bib.uottawa.ca/docview/235763873/fulltextPDF/5B9C654D74C463DPQ/1?accountid=14701. Accessed February 12, 2018.
5. Guttmann A, Schull MJ, Fund C, Vermeulen MJ, Stukel TA. Association between waiting times and short term mortality. Br Med J. 2011. doi:10.1136/bmj.d2983.
6. Asplin BR, Magid DJ, Rhodes K V, Solberg LI, Lurie N, Camargo CA. A Conceptual Model of Emergency Department Crowding. Ann Emerg Med. 2003;42:173-180. doi:10.1067/mem.2003.302.
7. Khanna S, Boyle J, Good N, Lind J. Unravelling relationships: Hospital occupancy levels, discharge timing and emergency department access block. Emerg Med Australas. 2012;24(5):510-517. doi:10.1111/j.1742-6723.2012.01587.x.
8. Ovens H. ED Overcrowding: The Ontario Approach. Acad Emerg Med. 2011;18(12):1242-1245. doi:10.1111/j.1553-2712.2011.01220.x.
9. Glazier RH, Zagorski BM, Rayner J. Comparison of Primary Care Models in Ontario by Demographics, Case Mix and Emergency Department Use, 2008/09 to 2009/10.; 2012. doi:doi:10.1201/9780203503942.ch2.
10. Vermeulen MJ, Stukel TA, Boozary AS, Guttmann A, Schull MJ. The Effect of Pay for Performance in the Emergency Department on Patient Waiting Times and Quality of Care in Ontario, Canada: A Difference-in-Differences Analysis. 2016. doi:10.1016/j.annemergmed.2015.06.028.
11. Schull MJ, Vermeulen MJ, Stukel TA, et al. Evaluating the Effect of Clinical Decision Units on Patient Flow in Seven Canadian Emergency Departments. Acad Emerg Med. 2012;19(7):828-836. doi:10.1111/j.1553-2712.2012.01396.x.
12. Affleck A, Parks P, Drummond A, Rowe BH, Ovens HJ. Emergency department overcrowding and access block. Can J Emerg Med. 2013;15(6):359-370. doi:10.2310/8000.CAEPPS.
13. Health Quality Ontario. Under Pressure Emergency Department Performance in Ontario Why It Matters System Performance Reporting. Toronto; 2016. http://www.hqontario.ca/portals/0/Documents/system-performance/under-pressure-report-en.pdf. Accessed November 22, 2017.
14. Home Care Ontario. Facts & Figures – Publicly Funded Home Care. http://www.homecareontario.ca/home-care-services/facts-figures/publiclyfundedhomecare. Published 2014. Accessed November 22, 2017.
15. Ontario Long Term Care Association. Building Better Long-Term Care.; 2017. http://www.oltca.com/OLTCA/Documents/Reports/2017OLTCABudgetSubmission.pdf. Accessed November 22, 2017.
16. Campbell SG, Sinclair DE, contributors TCA of EPFM. Strategies for managing a busy emergency department. CJEM. 2004;6(4):271-276. doi:10.1017/S1481803500009258.
17. Lin M, Taira T, Promes S, Regan L. Educational Excellence in a Crowded Emergency Department: Consensus Recommendations From the Council of Emergency Medicine Residency Directors 2010. J Grad Med Educ. 2011;3(2):249-252. doi:10.4300/JGME-D-10-00137.1.

