

Urgent care presents a specific set of challenging clinical questions for the emergency physician. Often, seemingly mundane presentations will leave us questioning whether or not we have managed a case appropriately. Our decision-making can be highly influenced by the long lasting effects of dogma, clinical anecdotes, or historical studies of limited methodological quality. In many cases, no evidence exists to help guide our practices. This often leads to huge variation in management strategies in these patients. Here, we seek to further explore the existing evidence for the management of three common urgent care presentations with evolving or controversial clinical approaches.
1) Review of basics and “can’t miss” diagnoses
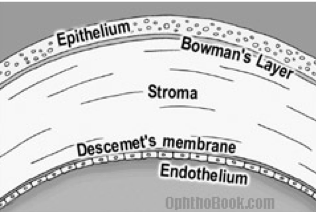
- The cornea:
- Acts as the primary infectious and structural barrier to the eye
- Is a multi-layered structure thinnest at its centre (approximately 0.5mm) and gradually increases in thickness to the periphery
- Is a five layer structure:
- The outermost layer is epithelium that is easily abraded but heals quickly without scarring
- Bowman’s layer is just deep to this and separates the epithelium from the underlying stroma.
- The stroma makes up approximately 90% of the cornea and when involved in injury, scarring can result.
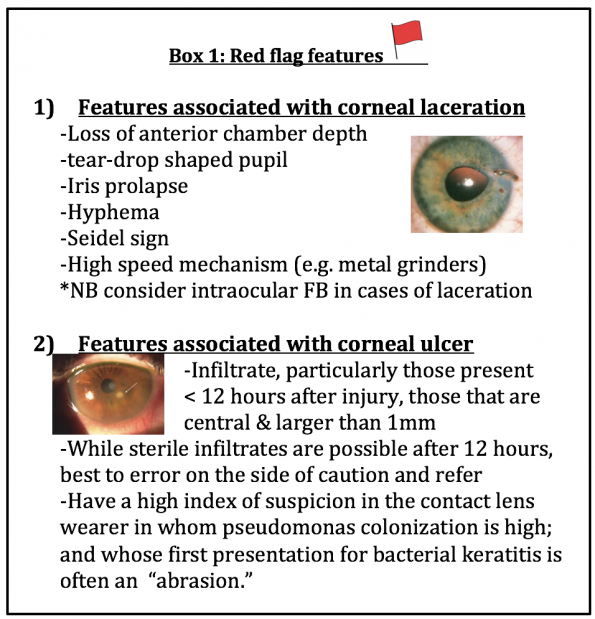
- Apart from the standard eye and slit lamp examination, providers should take special care to ensure several features are not present which may suggest more ominous pathology. (Box 1)
- Foreign bodies and retained rust rings can be removed by irrigation, moistened cotton tip, 18g needle tip or motorized burr
- Consider bringing the patient with retained rust ring back in 24 hours, as the cornea softens which facilitates removal
2) Antibiotic prophylaxis
Most texts and resources will recommend the provision of topical antibiotics to all corneal abrasion patients to limit infectious ulceration.
| Kruger et al. 1990 6 | • 94 patients (>50% had FB removed)
• Randomized to topical antibiotic or saline • No difference in infection rates, corneal healing, visual acuity or persistence of symptoms |
| King et al. 1993 7 | • 351 patients
• Included: metal and vegetative FB, fingernail abrasion, chemical, and flashburn • No antibiotics • Found 0.7% rate of infectious corneal ulcer overall |
| Upadhyay et al. 2001 8 | • Rural Nepal; 7x higher rate of corneal ulceration
• Topical antibiotics provided to all corneal abrasions at presentation • Late presentation / receipt of antibiotic after 18 hours associated with higher risk of infection |
This practice is not supported by evidence. To date in the literature, there is only one small RCT from 1990, and two observational studies looking at this issue.6-8 Of these, the only study in favour of utilizing antibiotics has significant methodological limitations that need to be considered.8
It is important to note that all studies demonstrating safety in omission of antibiotics have excluded the contact lens wearer who is at higher risk of pseudomonas colonization and bacterial keratitis.
Thus, in summary
- Provision of topical antibiotics likely provides limited benefit to the non-contact lens wearer
- Corneal abrasions in the contact lens wearer warrant prophylactic antibiotics that provide pseudomonal coverage. 6,7,9
3) a) Topical analgesics: Opthalamic NSAIDS
Several RCTs have evaluated the use of ophthalmic NSAIDS in the management of corneal abrasions. The majority have been small but positive trials for NSAIDs in their ability to reduce patient reported pain when compared to placebo or co-intervention. Unfortunately, the measured outcomes amongst the studies are very heterogeneous. Some groups identified primary outcomes of patient-reported pain by visual analogue scale, others by verbal pain scale; and some by surrogate markers, such as the need for breakthrough oral analgesics. This heterogeneity has made it very difficult for subsequent authors to pool study results.
Despite this, three fairly recent systematic reviews have been published.
- In 2005, our very own Dr Lisa Calder published a meta-analysis of 11 RCTS evaluating NSAIDs in corneal abrasion pain. Unfortunately only three of these RCTS could actually be included in the pooled effect calculations due to the fact that pain measurement occurred at different time intervals. A weighted mean difference of -1.30cm (-1.03 to 1.56) on the 10cm visual pain scale was demonstrated for ophthalmic NSAIDs when compared to placebo at the 24-hour mark. Based on existing literature, the authors concluded that this finding represented statistically and clinically significant pain reduction in the ED. It is important to note however that when sensitivity analyses were conducted to account for studies with design limitations, all significant findings were lost.10
In March and May of this year, two new systematic reviews were published. The first was conducted by a group of ED physicians in Florida and the second, was published by the Cochrane group.
- The initial review, like Dr Calder’s group, concluded that NSAIDs were efficacious in reducing patient-reported pain and found no increased risk of adverse outcomes. Their report was a qualitative summary and made no attempts at estimating pooled effect sizes.
- The Cochrane group evaluated a total of 9 RCTS. They had determined a priori that clinically significant reductions of pain would need to be 30% or 50% at 24 hours. None of the studies included this as a primary end point and they could therefore not draw conclusions on their primary outcome. They did however pool the results of four studies (N=481 patients) that utilized the need for “rescue analgesia” as a proxy for pain control. A statistically significant reduction in the need for oral analgesic breakthrough was demonstrated in the NSAID group (RR= 0.46; CI 0.34-0.61) when compared to placebo. While this was a statistically significant result, the authors felt that the quality of evidence was too poor to recommend ophthalmic NSAIDs in the management of corneal abrasion pain.12
Interestingly, no new studies have been published since 2001, and therefore all three of these systematic reviews have drawn somewhat different conclusions from the very same body of literature. Considering this, as well as the cost of the medication (40-60$ / bottle), it makes it difficult to suggest NSAIDs as a first line strategy.
3)b) Topical cycloplegics
Topical cycloplegics are often recommended in the management of corneal abrasions. In fact, they appear in both Tintinalli and Rosen’s as recommended treatment strategies. The proposed mechanism of action in reducing ocular pain is by eliminating ciliary spasm. While it is possible to develop flare or mild anterior chamber inflammation after 12-24 hours following corneal abrasions, there has never been published evidence to support that ciliary spasm is a significant contributor to pain in this patient population.
To date, a single RCT evaluating cycloplegia in corneal abrasion pain exists.
- Meek et al. published a triple blind RCT in 2010 comparing homatropine 5% to placebo eye drops. They took a convenience sample of 40 patients presenting with corneal abrasion associated with mechanical trauma within 12 hours of injury. All patients also received oral Tylenol and chloramphenicol. They obtained visual analogue scale at 0,6,12 and 18 hours. 50% of patients in the homatropine group and 60% of patients in the placebo group obtained a VAS greater than 20mm at 12 hours, however the reductions in both groups were not significantly different at any point in time. Overall, they did not feel that cycloplegia offered benefit in reducing pain in corneal abrasions.13
3)c) Topical anaesthetics
Topical anesthetics are effective agents for managing pain related to simple corneal abrasions. This is evidenced by the great relief patients experience within moments of instilling 1-2 drops of an anesthetising agent in the eye. We are taught however that use of these medications outside of the examination period should be strictly avoided due to potential for corneal toxicity and devastating corneal ulceration.
This topic has gained considerable attention in the FOAMed world over the past 1-2 years. Several groups have argued that the literature defending the harms of topical anesthetics is scant at best and originates namely from case series, case reports, and animal models.14, 25, 26
When examining the primary literature it becomes immediately apparent that this is true. The vast majority (if not all) of the evidence draws from individual cases of patients who have grossly abused topical anaesthetics for weeks to months. Some of these patients utilized high dose anaesthetics (e.g. 5% tetracaine), while others self-administered the medication prior to proper medical evaluation. Most cases continued to use the topical anaesthetic even once complications were identified and they were advised to stop. In several case series, psychiatric comorbidity was also at play.15-19
While more studies are required to comprehensively evaluate the safety and effectiveness of short-term topical anesthetics, the few trials that exist in the ophthalmology and emergency medicine literature are promising and offer a considerably higher hierarchy of evidence when compared to the evidence against topical anesthetic use.
In the Ophthalmology literature, topical anaesthetics are being evaluated for pain control after photorefractive keratectomy in which a surgically induced corneal defect results.20-22 While not identical to traumatic corneal abrasions, these sterile lesions are functionally similar to a corneal abrasion. Key studies are summarized below:
| Verma et al. 1995 and 1997 | 1995: Randomized, double blind placebo-controlled RCT including 44 post-operative PRK patients who received 1% tetracaine or placebo X 24h.
• Tetracaine group had VAS reduction of 7.5cm • Placebo group had VAS reduction of 3.5cm • All patients in both groups had full epithelial closure at 72 hours 1997: Follow up prospective RCT of 38 patients comparing 1% tetracaine to 0.75% bupivacaine. No difference in pain control between either group but full epithelial closure in all patients. |
| Shahinian et al. 1997 | Randomized double blind, placebo controlled trial including 34 patients post PRK who received proparacaine 0.05% or placebo for 1 week as needed. Patients in treatment group had statistically significant reduction in pain than did controls. No significant difference in number of days required to achieve complete corneal healing. |
Piggy backing on these post-operative studies showing safety and efficacy in pain management, studies have started to emerge in the ED setting for simple corneal abrasions.23-25
The primary literature is summarized below:
| Waldman et al. 2014
|
Randomized, double blind, placebo-controlled trial (n=116). Patients with *simple corneal abrasion randomized to 1% tetracaine q30 mins vs placebo drop for 24 hours.
While hourly VAS scores did not differ between groups, patients rated tetracaine a 7.7/10 in effectiveness vs 3.3/10 for placebo at study conclusion. No complications or delays in corneal healing at 48 hour slit lamp examination (SLEX). Equal retained rust rings in both groups. |
| Ball et al. 2009 | Very small randomized, double blind, placebo controlled trial (n=33) comparing placebo vs proparacaine 0.05% 2-4 drops PRN X 7 days. Total of 40 ml provided.
VAS scores taken 5mins after administration showed greater reduction in pain in anaesthetic group (-3.9cm in proparacaine group vs -0.6cm in placebo group). Higher reports of patient satisfaction in anaesthetic group. Follow up with optho-conducted SLEX at days 1, 3 & 5 demonstrated no delayed healing or complications. |
| Waldman et al. 2017 | Retrospective cohort study conducted in a New Zealand ED to assess safety of 24 hour tetracaine (1%) supply. In this study, a portion of ED physicians had implemented the use of topical anesthetics into their practice.
Study retrospectively compared patients with *simple corneal abrasion receiving 1% tetracaine drops q30 mins X 24 hours (1.5ml total) versus standard care. Patients monitored for number of ED rechecks, persistent fluorescein uptake, ophthalmology referrals, and complications. Results showed no significant difference in ED rechecks, ophthalmology clinic referrals or persistent fluorescein uptake in the simple abrasions treated with tetracaine. No serious complications noted. However, a large number of patients who had diagnoses other than simple corneal abrasion also received tetracaine (including those with retained rust rings, herpes keratitis, episcleritis, pediatric patients, etc.) In this group, there was an increased chance of ED recheck or persistent fluorescein uptake. This was likely due to the underlying pathology rather than the tetracaine. There was no significant increase in referrals to ophthalmology. Most importantly, no significant complications were seen in this more complex group. |
*Simple corneal abrasion: 18+ years, presented within 36 hours of injury, unilateral injury, non-contact lens wearer, no concurrent ocular infection or herpes keratitis, no injury requiring immediate ophthalmologic assessment, able to follow up at 48 hours, had grossly contaminated foreign body
In summary:
- The dogma of avoiding topical anaesthetics for symptom control in corneal abrasions has been driven by case reports and case series of topical anaesthetic abuse
- New evidence is emerging for the provision of a limited supply of topical anesthetics following photorefractive keratectomy and simple corneal abrasions in the ED 20-26
- While the samples sizes are small, the methodological designs are of much higher quality than any of the evidence against their use
- No adverse outcomes have been observed thus far, however safety cannot be concluded with small sample sizes
- The most recent analysis highlights the importance of a thorough clinical examination and appropriate diagnosis. (Although, in some respects, this study also highlights the fact that no adverse events were seen in this more complex group of patients either)
- Ongoing good quality data is required to ensure safety, however the adoption of brief anesthetic use is already occurring!
- It is imperative not to supply large amounts to patients and to discuss the devastating adverse effects associated with prolonged topical anesthetic abuse.
Anatomy and physiology of the fingertip and nail complex
Fingertip injuries are one of the most common presentations of hand trauma seen in the ED in both the adult and pediatric populations. In order to appropriately manage fingertip injuries, a good understanding of the anatomy and physiology of the distal finger and nail complex are required.
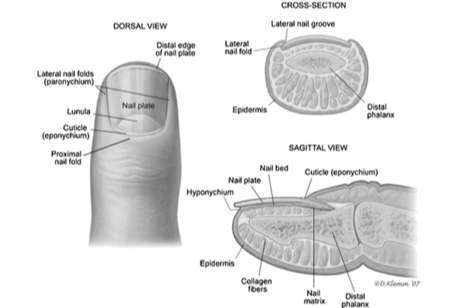
- The nail plate is a hard, keratinized structure that forms from cell division and apoptosis of the underlying nail bed.
- The nail bed is made up of the germinal matrix proximally, and the sterile matrix
- The germinal matrix is responsible for 90% of the nail growth. It arises from just distal to the extensor tendon insertion and extends to the lunula (white crescent seen under the nail).
- The sterile matrix extends distally from the lunula. It is responsible for the remaining 10% of nail growth and contributes to nail adherence.
- The borders of the nail bed include:
- The lateral folds of the nail or paronychium
- The eponychium or cuticle, proximally
- The hyponychium is the most distal border and meets the sterile matrix of the nail bed
When injury to the nail complex exists, general principles to consider include:
- The nail bed should be smoothed and re-approximated to limit nail deformity
- Ensure the germinal matrix is not entrapped within fracture fragments which can lead to higher rates of non-union and infection
- Consider the functionality of remaining nail complex structures in partial amputations (e.g. painful nail spikes can result from small remnants of germinal matrix
Subungual Hematomas
- Subungual hematomas often result from blunt trauma or crush injury to the distal phalanx with bleeding from the underlying vascular nail bed. Bleeding under the nail plate causes increasing pressure and pain and can also contribute to separation of the nail plate.3 Pain control and minimizing the potential for chronic nail deformity guides management strategies.
Some groups have argued that nail plate removal and exploration of the underlying nail bed should be based on the size of hematoma and the presence of an associated distal phalanx fracture. Simon and Wolgin’s work appears to be most frequently quoted in the literature to support this notion.
- They conducted a prospective observational study of 47 consecutive patients with subungual hematoma. All patients had an x-ray and subsequent nail plate removal with exploration, +/- suture repair of the underlying nail bed.
- They found that 60% of patients with a hematoma larger than half of the nail bed had lacerations requiring repair (>2-3mm). This number increased to 95% when they included those who also had underlying tuft fracture.
- They suggested that all patients with hematoma greater than half of the nail bed (and especially those with underlying phalanx fracture) should have the nail bed explored and repaired.
- They did not conduct any long term follow up on these patients and no comparison group was included
Since this was published, a number of observational studies followed with the hypothesis that nail bed exploration was actually not necessary and associated with higher costs. No RCTs have ever been conducted to compare the two strategies. Dean et al. summarized the literature in a 2012 systematic review. 5
- Included in their analysis were 4 observational studies that enrolled patients with subungual hematoma regardless of size or underlying phalanx fracture.
- Important exclusion criteria consistent across all studies were: cases with lacerated nail folds, a disrupted nail plate, and significantly displaced fracture fragments
- Three of the four studies treated all patients with trephination and obtained x-ray. Only one study prospectively enrolled patients to receive trephination versus nail plate removal and suture repair. In this study, nearly half of the patients enrolled to the trephination group actually refused care and were simply observed without intervention.
- In all studies, no significant complications or nail deformities were appreciated.
- Transient nail depressions were actually higher in those treated with nail plate removal and suture repair, but none of the deformities were long lasting.
- The cost of nail plate removal and suture repair was 4x higher than trephination!
In summary:
- While literature is limited, there does seem to be sufficient evidence to support trephination of ALL subungual hematomas regardless of size or associated phalanx fracture.
Exceptions to this rule include:
- Complicated subungual hematoma. i.e. injuries with laceration involving the nail folds or a disrupted nail plate
- Displaced distal phalanx fracture requiring surgical pinning (rare)
Trick of the trade: Tissue adhesive for nail bed laceration repair
Traditionally, lacerations of the nail bed are restored by meticulous re-approximation of the tissues using absorbable 6.0-7.0 suture. Recently however, studies have evaluated the use of tissue adhesives as an alternate technique. 6,7 In this technique, the nail bed tissues are reapproximated and subsequently a single layer of dermabond is applied. The nail plate itself is then placed back under the eponychial fold as a stent and glued into place. The trials have been conducted in both the adult and pediatric populations and have included complicated injuries including those with non-displaced phalanx fractures as well as large lacerations extending to the pulp. While the trials are small, they have demonstrated excellent cosmesis and no adverse events. They have also demonstrated a significant reduction in procedure length (approximately 9 vs 27 minutes). 6,7
4) Distal Phalanx Fractures
a) Prophylactic antibiotics
Distal phalanx fractures account for up to 30% of all hand injuries and 67% of all open hand fractures seen in the ED. In general, open fractures are considered to be at higher risk for infection and wound complications; however most of the evidence to support this notion comes from studies evaluating long bone fractures and injuries at sites other than the hand.8 The role of prophylactic antibiotics in distal phalangeal fractures (and in hand trauma in general) is highly controversial. Many have argued that several factors make these injuries low risk for infection. These factors include:
- The high vascularity of the hand
- Mechanism of injury (generally crush or clean incision) which is associated with less periosteal stripping
- Ability to rapidly achieve anesthesia by regional block allowing timely irrigation and debridement
A 2016 meta-analysis was published in The Journal of Hand Surgery that evaluated the need for prophylactic antibiotics in open distal phalanx fractures. It analyzed 4 RCTS which included a total of 353 fractures.8
- There was a great deal of heterogeneity in study design.
- The authors concluded that there was no statistically significant increased risk of superficial infection in patients who received placebo vs antibiotics. There were no cases of osteomyelitis or deep infection reported in either group. They felt this finding persisted when only the two most recent and highest quality trials were included.
It is important to consider that all four studies emphasized copious wound irrigation and wound debridement. Only one study actually spells out how much volume they used (500cc). In speaking with various plastic surgery residents, 500cc would be the minimum irrigation volume.
Additional considerations to keep in mind regarding the 2016 metanalysis are the exclusion of patients with peripheral vascular disease and diabetes. The largest and most robust trial excluded this patient population and the second largest trial was conducted in the pediatric population where PVD and DM is not well represented. This leaves us with a true paucity of evidence to guide management in these possibly higher risk individuals.
b) Special Circumstances
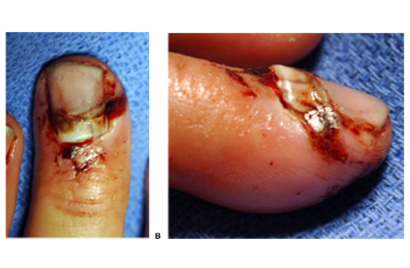
- Transverse fracture pattern with dorsal displacement
- Most distal phalanx fractures are minimally displaced requiring simple splint for 2-3 weeks
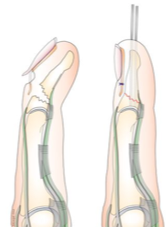
- However some transverse distal phalanx fractures, particularly those that are more proximal along the phalanx, have the potential to displace dorsally and herniate through the sterile matrix.
- Often, one will see the nail plate avulsed from under the eponychial fold in these injuries (image on below)
- The germinal matrix in these cases is often rolled up proximally or tucked between bony fragments. 2
- Without proper anatomic reduction and freeing the fracture site of the germinal matrix, patients can end up with non-union, chronic osteomyelitis, nail deformity, or painful inclusion cysts.
- Seymour Fractures
- This fracture pattern is seen in the skeletally immature and is often under-recognized by the ED physician
- It is a juxta-epiphyseal fracture of the terminal phalanx in conjunction with laceration of the nail bed, subungual subluxation, and flexion deformity
- Seymour fractures are at increased rates of complications including: infection, growth plate arrest, and chronic osteomyelitis.
- The injury resembles a mallet finger deformity however the mechanism of deformity is actually due to the forces exerted by the extensor and flexor tendons across the fracture site
- Often, these injuries require surgical exploration to free the germinal matrix from the fracture site as well as K-wire pinning
- Emerging literature shows that early surgical intervention and prophylactic antibiotics are warranted because of their high infection and complication rates.

In summary:
- Antibiotic prophylaxis in hand trauma and in particular open distal phalanx fractures continues to be a controversial topic with limited objective data to support decision making
- Local practices lean towards omission of antibiotics with a few exceptions:
- Grossly contaminated and bite / puncture wounds
- Seymour fractures
- Case by case consideration in patients with significant peripheral vascular disease or immune suppression
- Proper irrigation and wound debridement is an essential component of management
- Beware Seymour fractures and distal phalanx fractures with dorsal displacement of the nail plate which can be at increased risk of infection and may require surgical intervention
Evidence for topical vasoconstrictors
Despite being a common ED complaint, there is a large paucity of evidence available to guide clinicians in their selection between various epistaxis management techniques. This lack of evidence is particularly true of the use of topical vasoconstrictors that are often employed as some of the first line strategies. No RCTs have ever been conducted to show superiority of one agent over another. In fact, no RCTS evaluating vasoconstrictors in the ED setting actually exist!
One of the only ED based studies that supports vasoconstrictor use was conducted by Matoo et al. in 2011.
- They prospectively evaluated efficacy of silver nitrate cautery when paired with one of: manual pressure X 10 min, topical 0.05% xylometazoline, or topical epinephrine (1:10 0000) in patients presenting to the ED with idiopathic epistaxis
- The outcomes measured included achievement of hemostasis in the ED and re-bleeding at 1 hour and 4 days.
- By the 4 day mark, authors found 34% success rate with manual compression, 86% with xylometazoline, and 90% epinephrine when paired with silver nitrate cautery
Many have extrapolated from studies evaluating epistaxis prevention in nasal intubation or endonasal surgical procedures. 2,3 For the most part, these studies have found that xylometazoline is as effective as cocaine and perhaps slightly more effective than epinephrine in its ability to prevent epistaxis.
When one considers this lack of evidence as well the addictive nature, cost, and possible cardiotoxic effects of topical cocaine or epinephrine, the use of xylometazoline as a first line agent appears most reasonable. It is important to remember however, that xylometazoline does not provide analgesia if cautery or packing are required!
Emerging therapies: topical tranexamic acid
Tranexamic acid (TXA) is an antifibrinolytic agent that functions through competitive binding for lysine on plasminogen. This binding prevents activation of plasminogen to plasmin, thereby blocking clot breakdown.4 The use of TXA has gained considerable attention in recent years in the trauma and surgical literature.
Cochrane reviews of both intravenous and topical application of TXA in the surgical setting has demonstrated significant reduction in bleeding and need for peri-operative transfusion. This emerging evidence has driven optimism about the use of topical tranexemic acid in non-surgical entities, including epistaxis.
The literature supporting TXA use in epistaxis is still early in its development, but more data continues to emerge at this time. A 2016 systematic review summarized the existing literature for TXA in epistaxis patients.
They identified a total of 5 RCTs. Three studies were conducted in the setting of idiopathic anterior epistaxis and employed oral or topical TXA to achieve hemostasis (see table below). The additional studies reviewed TXA for epistaxis prevention in patients with hereditary haemorrhagic telangiectasia.
| Study | Interventions: | Outcomes measured: | Results: | Comments:
|
| Zahed et al. 7 (2013)
Exclusions: Posterior epistaxis, coagulopathies, INR >1.5, visible bleeding vessel |
Randomization of 224 patients with epistaxis in the ED to 15cm cotton pledget soaked in 500mg TXA (5ml of injectable drug)
vs Standard anterior packing with multiple cotton pledgets after 10min premedication of epinephrine (1:100 000) and 2% lidocaine
|
Bleeding arrest at 5 minute intervals, duration of time spent in ED, patient satisfaction, frequency of re-bleeding at 24 hours and 7 days | 71% of TXA patients had hemostasis achieved within 10 minutes compared to 31% in anterior nasal pack group
95% of TXA patients discharged < 2 hours compared to 6% in anterior nasal pack
Higher patient satisfaction in TXA group
Rates of bleeding reduced at 24 hours (4.7% vs 12%) and 7 day mark (2.8 vs 11%) |
Lack of true blinding to physicians because of look and smell of various pledgets
Somewhat unclear methods reassessment for bleeding amongst groups
All TXA pledgets removed prior to ED discharge vs all anterior packs left in place for removal at later date despite assessment of bleeding |
| Tibbelin et al. 8 (1995)
Excluded: Children, impaired hemostasis, fractured skull or nose, perforated septum |
68 adult patients with ongoing epistaxis in ED randomized to receive 15ml of 10% TXA gel versus 15ml placebo gel administered intranasal by syringe.
No manual pressure or packing applied in either group. |
Measured ongoing bleeding at 30 minutes, percentage of re-bleeding at 10 days and patient satisfaction. | TXA group at baseline (prior to intervention) had significantly higher rate of moderate to severe bleeds.
No difference for ongoing bleeding at 30 minutes or re-bleeding at 10 days |
High risk of bias, limited description of study protocol available. |
| White et al. 9 (1987)
Excluded: History of VTE, on OCP, renal insufficiency, on antiplatelet or anticoagulation |
89 adults patients requiring admission to hospital for epistaxis.
Randomized to receive oral TXA at 1000mg TID or placebo tablets X 10 days.
Balanced for initial treatment strategies (i.e. cautery vs ant/post packing) |
Daily assessment for ongoing bleeding. Review for re-bleeding at 3 week post discharge. |
No difference in length of hospital stay between the two treatment groups.
Rate of re-bleeding 45% in placebo group versus 31% in TXA group (not statistically significant)
|
Low risk of bias.
Underpowered by approximately half.
|
Since the 2016 systematic review, an additional RCT by Zahed et al. has been published.10 They utilized the same study design as their 2013 publication 7 (included in table above). Only this time, they selected patients on one or more anti-platelet agents. Findings are summarized below:
- 73% of TXA patients had hemostasis achieved at 10 minutes versus 29% in the anterior nasal pack group (ANP)
- Rates of re-bleeding at day 1: 5% w/ TXA versus 10% w/ ANP
- Rates of re-bleeding at day 7: 5% w/ TXA versus 21% w/ ANP
- Patients discharged <2 hours: 97% w/ TXA versus 13% w/ ANP
- Patient satisfaction: 9/10 w/ TXA versus 4/10 w/ ANP
While these findings are again very impressive, the same limitations of study design seen in the 2013 trial apply!
Nasal packing and prophylactic antibiotics
The use of prophylactic antibiotics in nasal packing has been one of the traditional teachings of epistaxis management. Both Tintinalli and Rosen’s will advocate for antibiotic use whilst also acknowledging lack of evidence.
The basis for this recommendation is to prevent complications related to staph aureus and strep pyogenes including toxic shock syndrome (TSS), otitis media, and sinusitis. Amongst these complications, TSS is the most feared complication. There has however, never been a case report of TSS after anterior nasal packing in epistaxis. Rare case reports of TSS do exist in patients receiving anterior nasal packing after sinus surgery.
To say evidence is lacking to guide management in this area is truly an understatement.
There is not a single ED based study that exists despite the fact that most anterior nasal packs are being managed by ED physicians from start to finish!
The only evidence that exists is from small retrospective or prospective observational studies in admitted patients with epistaxis.
The largest of these studies was conducted in 2012 by Peper et al. and was a before-and-after non-randomized, non-blinded trial. 13
- 149 patients requiring anterior packing and admission for primary idiopathic epistaxis were included.
- The first 78 received oral clavulin X 5 days (macrolide in the case of pencillin allergy). The subsequent 71 patients received placebo.
- All patients had packs for at least 24-36 hours
- No infectious complications developed in either group.
Another interesting study from 1989 randomized 20 patients with posterior nasal packs to IV cefazolin versus placebo. All patients had antibiotic impregnated packs that were kept for 72 hours. 14
- They monitored for outcomes of infection and also took swabs of the nasal passages upon removal of the packs
- Those that received cefazolin had growth of a single organism, while those who received placebo had heavy growth of multiple organisms
- Despite this, neither group had any infectious complications.
- In the realm of growing antibiotic resistance, the fact that there was selection for a single organism in the antibiotic group is actually quite worrisome!
Anecdotally, at our own institution, most ED physicians are NOT providing antibiotics in anterior nasal pack patients without sequelae. While this is likely safe and most appropriate in terms of antibiotic stewardship, there is a lack of evidence to actually support this practice. Dr Cohn, an emergency physician who published a best available evidence review in the Annals of Emergency Medicine in 2015 summarized this issue best in his statement…
“Although there is no compelling evidence to refute the utility of prophylactic antibiotics in [anterior nasal packing], there is also no evidence that withholding antibiotics causes harm”
In summary, additional study of this very common ED presentation is essential and could have the potential to widely change practice patterns of ED physicians and ENTs alike!
References
- Stapczynski, J. S., & Tintinalli, J. E. (2011). Tintinalli’s emergency medicine: A comprehensive study guide(7th ed.). New York, N.Y.: McGraw-Hill Education LLC..
- Marx, J. A., & Rosen, P. (2014). Rosen’s emergency medicine: Concepts and clinical practice(8th ed.). Philadelphia, PA: Elsevier/Saunders.
- Root, T. Opthobook. Online access: https://timroot.com/anatomy/
- DelMonte, D. & Kim, T. Anatomy and physiology of the cornea. J Cataract Refract Surg 2011; 37: 588-598.
- Calder, L., Balasubramanian, S., Stiell, I. Lack of consensus on how to treat corneal abrasions: results of a national survey. Can J Emerg Med. 2004; 6: 402-407.
- Kruger RA, Higgins, J., Rathford S., et al. Emergency eye injuries. Aust Fam Physician 1990; 19:934-8.
- King, J. & Brison, R. Do Topical Antibiotics Help Corneal Epithelial Trauma? Canadian Family Physician 1993; 39: 2349-2352.
- Upadhyay, M., Karmacharya, P., Koirala, S, et al. The Bhaktapur eye study: ocular trauma and antiobiotic prophylaxis for the prevention of corneal ulceration in Nepal. Br J Ophthalmol, 2001, 85, 388-392.
- Mackway-Jones, K. Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. Antibiotics and corneal abrasion. J Accid Emerg Med 1998; 15:353-355.
- Calder, L., Balasubramanian, S. & Fergusson, D. Topical Nonsteroidal Anti-inflammatory Drugs for Corneal Abrasions: Meta-analysis of Randomized Trials. Acad Emerg Med 2005, 12; 467-473.
- Thiel B, Sarau A, Ng D. Efficacy of Topical Analgesics in Pain Control for Corneal Abrasions: A Systematic Review. Cureus 2017, 9(3): e1121.
- Wakai A, Lawrenson JG, Lawrenson AL, Wang Y, Brown MD, Quirke M, Ghandour O, McCormick R, Walsh CD, Amayem A, Lang E, Harrison N. Topical non-steroidal anti-inflammatory drugs for analgesia in traumatic corneal abrasions. Cochrane Database of Systematic Reviews, 2017, 5,
- Meek, R., Sullivan, A., Favilla, M., et al. Is homatropine 5% effective in reducing pain associated with corneal abrasion when compared with placebo? A randomized controlled trial. Emerg Med. 2010;22(6):507–513
- Rezaie, S. Topical Anesthetic Use On Corneal Abrasions. Rebel EM, 2017, published online: http://rebelem.com/topical-anesthetic-use-corneal-abrasions/24730399/
- Epstein, D. & Paton, D. Keratitis from misuse of corneal anaesthetics. N Engl J Med 1968; 279: 396-399.
- Patel, M. & Fraunfelder, F. Toxicity of topical ophthalmic anaesthetics, Expert Opinion on Drug Metabolism and Toxicology, 2013; 9, 983-988.
- Chen H, Chen K, Hsu W. Toxic keratopathy associated with abuse of low-dose anesthetic. Cornea2004;23(5):527-9
- Varga J, Rubinfeld R, Wolf T, et al. Topical anaesthetic abuse ring keratitis: report of four cases. Cornea1997;16(4):424-9
- Erdem, E., Undar, I.H., Esen, E. et al, Topical anesthetic eye drops abuse: are we aware of the danger?. Cutan Ocul Toxicol. 2013;32:189–193.
- Verma, S., Corbett, M., Marshall, J. A prospective, randomized, double-masked trial to evaluate the role of topical anesthetics in controlling pain after photorefractive keratectomy. Ophtalmology, 1995, 102: 1918-1924.
- , S., Corbett, M., Patmore, A., et al. A comparative study of the duration and efficacy of tetracaine 1% and bupivacaine 0.75% in controlling pain following photorefractive keratectomy. Eur J Opthalmol. 1997: 7: 327-333.
- , L., Jain, S., Jager R., et al. Dilute topical proparacaine for pain relief after photorefractive keratectomy. J Refract Surg. 2000; 16: 444-447.
- Waldman, N., Densie, I., Herbison, P. Topical tetracaine use for 24 hours is safe and rated highly effective by patients for the treatment of pain caused by corneal abrasions: A double blind randomized clinical trial. Acad Emerg Med. 2014: 21: 374-382.
- , I., Seabrook, J., Desai, N., et al. Dilute proparacaine for the management of acute corneal injuries in the emergency department. CJEM. 2010: 12: 389-394.
- Waldman, N., Winrow, B., Densie, I., et al. An observational Study to Determine whether routinely sending patients home with a 24-hour supply of topical tetracaine from the Emergency Department for Simple Corneal Abrasion Pain is Potentially Safe. Ann Emeg Med,2017, 1: 1-12
- Swaminathan, A., Otterness, K., Milne, K., et al. The safety of topical anesthetics in the treatment of corneal abrasions: a review. J Emerg Med. 2015; 49, 810-815
- Puls, H., Cabrera, D., Murad, M. et al. Safety and effectiveness of topical anesthetics in corneal abrasions: systematic review and meta-analysis. J Emerg Med. 2015; 49: 816-824.
- Matoo, O., Yousuf, A., Mir, A., et al. Control of Anterior Epistaxis: A comparative Analysis of the Decongestive Effect of Xylometazoline and Adrenaline in Idiopathic Epistaxis in Emergency Settings. Clinical Rhinology: An International Journal, 3: 130-135.
- Campbell, J., Campbell, C., Warren, D. et al. Comparison of the vasoconstrictive and anesthetic effects of intranassaly applied cocaine vs xylometazoline/lidocoaine solution. Otolyarngol Head Neck Surg, 5: 607-700.
- Katz, R., Hovagim, A., Finkelstein, H. et al. A comparison of cocaine, lidocaine with epinehrine and oxymetazoline for prevention of epistaxis on nasotracheal intubation. Journal of Clinical Anesthesia, 2, 16-20.
- Ker K, Prieto-Merino D, Roberts I. Systematic review, meta-analysis and meta-regression of the effect of tranexamic acid on surgical blood loss. British Journal of Surgery 2013, 10,1271-1279.
- Ker K, Beecher D, Roberts I. Topical application of tranexamic acid for the reduction of bleeding. Cochrane Database Syst Rev 2013;7:CD010562.
- Kamieh, Y. & Fox, H. Tranexamic acid in epistaxis: a systematic review. Clin Otolaryngol, 41, 771-776.
- Zahed R, Moharamzadeh P, Alizadeharasi S, Ghasemi A, Saeedi M. A new and rapid method for epistaxis treatment using injectable form of tranexamic acid topically: a randomized controlled trial. Am J Emerg Med 2013;31:1389-92
- Tibbelin A., Aust R., Bende M. et al. (1995) Effect of local tranexamic acid gel in the treatment of epistaxis. ORL 57, 207–209
- White A., O;Reilly F. Oral tranexamic acid in the management of epistaxis. Clin Otolyarngology 1988: 13, 11-16.
- Zahed, R., Hossain, M., Jazayer, M. Topical Tranexamic Acid compared with anterior nasal pack for treatment of epistaxis in patients taking antiplatelet drugs: Randomized Control Trial. Journal of the Society for Academic Emergency Medicine, 2017: epub ahead of print.
- Biswas D., Mal, R. Are systematic prophylactic antibiotics indicated with anterior packing for spontaneous epistaxis. Acta Oto-Laryngologica, 2009, 129: 179-181.
- Biggs, TC et al. Should prophylactic antibiotics be used routinely in epistaxis patients with nasal packs? Ann R Coll Surg Eng 2013, 95: 40-42.
- Peper, C. et al. Prospective study of the risk of not using prophylactic antibiotics in nasal
- packing for epistaxis. J Laryng Otology 2012: 257-259.
- Derkay, C. et al. Posterior nasal packing. Are intravenous antibiotics really necessary? Arch Otolaryngol, 1989, 115: 439-441
- Cohn, B. Are prophylactic Antibiotics Necessary for Anterior Nasal packing in Epistaxis? Annals of Emergency Medicine, 65, 109-111.
- Patel, L. Management of Simple Nail Bed Lacerations and Subungual Hematomas in the Emergency Department. (2014). Pediatric Emergency Care, 30, 742-745
- Rozmaryn, L. Chapter 3: Distal phalangeal and fingertip injuries. Accessed online: Nov 2017.
- Batrick, N., Hashemi, K., Freij, R. et al. Treatment of uncomplicated subungual hematoma. Emergency Medicine Journal, 2003, 20, 65.
- Simon, R., Wolgin, M. Subungual hematoma: association with occult laceration requiring repair. Am J Emerg Med. 1987: 5: 302-304.
- Dean, B., Becker, G., Little, C. The Management of the Acute Traumatic Subungual Haematoma: A Systematic Review. (2012). Hand Surgery, 17, 151-154.
- Strauss, E., Weil, W., Jordan, C. et al. A prospective randomized controlled trial of 2-octylcyanoacrylate versus suture repair for nail bed injuries. J Hand Surg Am. 2008; 33: 250-253.
- Langlois, J., Thevenin, Lemoin, C., Rogier, A., et al. The use of 2-octylcyanoacrylate for the treatment of nail bed injuries in children: results of a prospective series of 30 patients. J Child Orthop. 2010; 4: 61-65.
- Metcalfe, A., Aquilina, L., Hedley, M. Prophylactic antibiotics in open distal phalanx fractures: systematic review and meta-analysis. 2016; 4, 423-430.
- Sloan, JP, Dove, AF, Maheson, M.Antibiotics in open fractures of the distal phalanx? J Hand Surg Br. 1987, 12: 123–4.
- Suprock, MD, Hood, JM, Lubahn, JD.Role of antibiotics in open fractures of the finger. J Hand Surg Br. 1990, 15: 761–4Stevenson, J., McNaughton, G., Riley, J. The use of prophylactic flucloxacllin in the treatment of open fractures of the dsital phalynx within an accident and emergency department: a double blinded randomized placebo-controlled trial. J Hand Surg Br. 2003; 112: 337-338.
- Albergott, C., Garcia, F., Nager, A. Pedatric fingertip injuries: do prophylactic antibiotics alter infection rates? Pedatr Emerg Care. 2008: 24: 148-152.
- Krusche-Mandl, I., Kottstorfer, J., Thalhammer, G. Seymour Fractures: Retrospecive Analysis and Therapeutic considerations. J Hand Surg AM, 2013, 38(2):258-64.
- Abzug, J. & Kozin, S. Seymour fractures. J Hand Surg AM, 2013, 38(11):2267-70.


Trackbacks/Pingbacks