
There is no denying that the evolution of technology will continue to alter our practice of Emergency Medicine; a prime example of this has come with the transition to electronic health information within our clinical environments. In seeking to better understand the effect of such a shift, this post aims to highlight three big-picture implications for today’s Emergency clinician by:
- Reviewing how Canada has transitioned to digital health information, discussing where we are now, and demonstrating why we need to advocate for better connectivity
- Highlighting the benefits and challenges that exist for Emergency physicians when interacting with electronic health information systems
- Exploring how the practice of Emergency Medicine may continue to evolve as electronic health information continues to advance
Behind the Curve of Technology
As technology has progressed, we have watched computers become staples in our businesses, hospitals, homes, and pockets. Each year, software and performance capabilities become more sophisticated and allow us to re-invent our everyday routines.
“Convenient. Efficient. Connected.”
These are three words that stand out when I think about computer technology and a lot of the personal software I interact with on a day-to-day basis.
But are these the same words that come to mind while interacting with technology in a Canadian hospital? Sometimes. Though there have been some incredible technological innovations in this setting, I cannot help but look around and feel like healthcare is 5-10 years behind – especially as it relates to transfer of basic patient information.
It seems ironic that I can access a point-of-care tool like UpToDate® or Dynamed® to look up the details about almost any health condition I encounter, but still, I have to rely on a patient’s verbal history to generate a list of their health conditions. Unfortunately, key information may be missed if patients cannot recall the full details of their history, withhold information that they deem unnecessary, or are unable to communicate a history due to the emergent nature of their presentation. A list of health problems is no more complicated to store digitally than a grocery list, but somehow this information is not reliably accessible. In some places there may be information for local patients but what about those visiting from out of town?
Similarly, though I can look up the mechanism of action, side effects, and dosing for any medication from my phone, I am not always guaranteed an up-to-date list of medications and doses when asking my patient. I often breathe a sigh of relief when a patient can provide the crinkled pharmacy paper stored in their wallet because it is often the quickest and most reliable way to get an up-to-date list of medications in many hospital settings. Although connected pharmacy portals are in creation, this is yet another area where I see technology lagging behind.
Anecdotally, we know that most health information has been converted to digital format at some point – it is 2018 after all. So why is it still so frequently inaccessible? And what is being done to help rectify this situation?
Digital Health Information in Canada – Connecting Silos
Data organization, storage, and accessibility, has a lot to do with how our health care system is organized. Because health care is delivered provincially, each province or territory also controls its own health information infrastructure as well.
When the health care field first began creating its own software solutions, developers were more than happy to move documentation, lab testing, and diagnostic imaging from paper to computer screens. Unfortunately, many of these programs were created in isolation and ideas like compatibility and data transfer became an afterthought.
Perhaps you have heard the analogy that health information is often stored in silos – that there are lots of individual repositories of data, but no communication between them. Because most computer solutions were not built with data exchange in mind, the digitization of health information simply transformed paper silos into new digital silos. Though some of these systems are more connected, lack of interoperability continues to prevent meaningful data exchange and remains a primary goal for improvement within Canadian health care informatics today. 1
Let’s use three provinces to highlight the challenge of data exchange and the ongoing efforts to rectify this problem.
A Tale of Three Provinces
Ontario – eHealth
eHealth Ontario is Ontario’s attempt to consolidate all of a patients’ most important health information into an Electronic Health Record (EHR). This is something that all provinces and territories have implemented or are moving toward in some fashion. In order to have a comprehensive patient record, it is necessary to compile a variety of different data points – laboratory values, diagnostic imaging, hospital discharge summaries, immunization records, etc. Unfortunately, the complexity of this task is not a small one.
Take laboratory data for example. Before creating a centralized database with this information, all the laboratories in the province must be contacted – private and public. Second, it is important to find out what computer software is already being used (because remember, everyone went out and bought their own solution already) and then discuss how data will be transferred and stored in a common format. This requires developing standards across the entire province so that meaningful data exchange can occur.
After repeating this process with hospital summaries, consultations, and diagnostic imaging, it becomes more understandable why a province with a population of over 13 million can be a challenging system to create. Although it has taken a long time, the Connecting Ontario Clinical Viewer now allows clinicians online access to these data repositories, but patients do not yet have online access to their personal record. 2
Nova Scotia – MyHealthNS
In Nova Scotia, they have more recently completed their own health information portal. One of the unique features within this project is that it provides patients with access to the same important reports and documentation as health providers and also engages patients by allowing them to act as collaborators and update their health profile with any information that is not captured from digital sources. Because this data is accessible to the patient anywhere they have an internet connection, they are able to share this with any provider by bringing it up on their smartphone or tablet – a truly portable solution even across the country. 3
Alberta – Netcare
Finally, there is Netcare, Alberta’s approach to consolidating patient information. Like the other systems, they have compiled all the key components expected of an EHR. Where it sets itself apart is that every Albertan has had a record since 2008 and the system has had most of its current capabilities since 2011. 4 Alberta was one of the earliest provinces to reach a level of data exchange that many other provinces and territories covet. Despite how connected Alberta is, Alberta Health Services (AHS) has noted that there are still more than 1300 systems operating and exchanging information within the province. Although they are well connected, there have still been challenges with data exchange and the province has concluded that this is not sustainable in the long run. In response, they have recently announced that they will be moving to a single platform for the entire province. They have called it a Clinical Information System with the branding “Connect Care”. It means the whole province will be rolling out an end to end electronic health system over the next 4-5 years provided by Epic Systems. 5 One record, for every patient, that is accessible to provider and patient and follows them wherever they receive care in the province – isn’t this what we wanted all along? What does this mean for all other provinces that have been trying to build “Netcare equivalents” – will they too become unsustainable? This begins a much larger discussion, but it is certainly worth thinking about.
Why Accessibility Matters
Why does the current state of data exchange in Canada matter to an Emergency physician? I would argue that there is nowhere else in medicine where timely access to patient information is as important as within the Emergency Department. The provincial initiatives that transfer patient information between providers are the systems that will help us to better understand and treat the patients in front of us.
Knowing if a patient has had recent testing in the community may give us helpful baselines to compare with today’s blood work. Alternatively, it may prevent us from doing investigations all together if they have been recently completed or are already in progress, thereby helping to expedite disposition.
As these systems continue to evolve, I think it is our responsibility as Emergency Physicians to advocate for how these systems are created and contribute suggestions for improved accessibility to the most relevant information that helps influence our care on the front lines.
Is a Digital Emergency Department a Better Department?
Despite the fact that many primary care settings like Family Medicine have transitioned to an electronic medical record, most Canadian Emergency Departments have yet to make the full transition to a completely electronic system with many departments still functioning in a hybrid model mixing paper and computer workflows.
When considering a transition to an all-digital Emergency Department, the frequent question asked is whether the transition to a fully electronic environment will enhance or hinder patient care and flow. Will it improve patient safety? Does it have the potential to improve patient outcomes? Will it reduce unnecessary testing? Will it allow for more timely access to care?
Variable Potential
The transition to electronic health information in an Emergency Department provides an opportunity to re-imagine everyday processes and flow of information. In many cases, workflows will be transferred from paper to computer but in other situations it will be possible to re-imagine a process altogether thanks to the technology that is now at our disposal. Whether this transfer to a digital format creates meaningful change in the quality of patient care is not a simple answer.
It definitely has the potential to improve patient safety, improve patient outcomes, reduce unnecessary testing, and allow for more timely access to care. Unfortunately, there are so many variables between systems, users, and hospitals that attribution for improved patient care is difficult to assign to the electronic health information system alone. Knowing this, it is probably more important to think about how these electronic systems can enable us to move toward delivering the features we associate with quality care. Similarly, it is also important to consider some of the new challenges that might accompany the transition to a digital workflow.
Safety
When it comes to patient orders, there has been no shortage of errors using a paper-based system due to incorrect dosing, lack of legibility, or ordering of a medication that has an unrealized interaction or adverse side effect with the patient’s other medications. By ordering electronically, doses can be suggested and screened for appropriateness, interactions and allergies can be automatically brought to the physician’s attention, and all the necessary components required for an order must be present before it is able to be processed. But imagine how a new digital system might affect us in the Emergency Department; we are never managing one patient at time. Previously, patients were separated by physical charts and order sheets, but within a fully electronic system they are now only separated by tabs on a digital screen. In this new setup, it is not difficult to imagine a situation where the provider accidentally clicks the wrong chart, orders a medication meant for another patient and rushes off to the resuscitation bay where a trauma patient has just arrived. Another possibility is that the system sends so many warnings about orders that alert fatigue sets in and the critical warning for a patient is clicked away as presumed white noise. Perhaps lack of familiarity with a new ordering system might cause problems around transition; despite confirming the right patient, dose, and medication, an order is submitted not realizing the default setting allows the dose to be repeated 3 times when the intention was to only give it once.
How about the importance of leaving a clear record documenting the patient’s emergency visit? Not only does this principle help medico-legally, but it also enhances handover to the next provider needing context or history. Naturally, an electronic record eliminates issues of legibility or the possibility of a lost chart. But similar to ordering the wrong medication for a patient, it may be just as easy to accidentally document on the wrong patient’s digital chart. When we talk about quality of a note, it is also hard to know whether reliability will decline as copying and pasting previous summaries or documentation becomes more pervasive. Although notes and charts will not go missing (hopefully) it is still possible that incomplete notes could become an issue. In a paper-based system, notes were often completed right away so that others could use the chart for orders or other documentation. Now that notes can be completed later, is there a risk of electronic notes being left incomplete? The flexibility offered by this setup certainly has advantages and disadvantages within the confines of the Emergency Department.
Speed
Because technology tends to improve efficiency and speed in most areas of our lives, a natural question is whether electronic health records will allow for faster care. If we see patients faster, and reach a disposition within a shorter time span, perhaps we can reduce the length of stay and improve time to assessment for additional patients waiting to be seen. There are obvious benefits to an electronic system like reduction in copying information to a written chart. But does elimination of redundant charting offset the new electronic work flow? How about some of the situations that are more unique to the Emergency Department – like a trauma or a resuscitation. Are electronic records nimble enough to capture the needed information or is paper still the best way to go in these scenarios?
In a study by Coffey et al. (2015) they looked at how well a digital record performed during trauma resuscitations in a level 1 pediatric trauma centre. They analyzed the records before and after implementation of an electronic template and found that in many aspects, the electronic form was able to more completely capture data from the trauma cases than paper records.
When looking more closely at this study, I believe the most important message was in the methodology. At this particular centre, collaboration took place between the trauma team and emergency nursing staff to create a tool that captured the most important data points for this record. A custom form was then created to accomplish their unique goals and designed in a way that was user friendly, quick, and efficient. Significant time also went into training the nursing staff on how to be competent with this new form. While it is great that they showed electronic records could perform as well or better than paper, what this study really highlights is something more significant. Many of today’s modern health information systems are very powerful and deliver a lot of potential to increase quality of care; however, this potential is only realized when all stakeholders get involved to learn the capabilities of a new system, develop new workflows, and continue to find ways that these new tools can be used to deliver safer and more efficient patient care.
Launching a Digital Department
Although it’s impossible to predict how the launch of a new electronic health information system will go for each Emergency Department, there are some strategies and experiences that have been shared in the literature.
Having all stakeholders engaged throughout all stages of implementation was a key feature identified to help promote a successful launch. With regards to the role of physicians, there is often a suggestion to have “electronic medical record champions” who have completed additional training and act as educators for their colleagues. 7 Additionally, some Emergency Department have also taken the steps to increase their staffing in order to mitigate the expected slow-down of a transition. 8 While most other areas of medicine may have a quieter time of year to help facilitate launch, we are all well aware that there is no true “slow season” in the ED, which adds another unique challenge. If there is no slow season, how much of a toll will transitioning to a fully digital department have on patient flow?
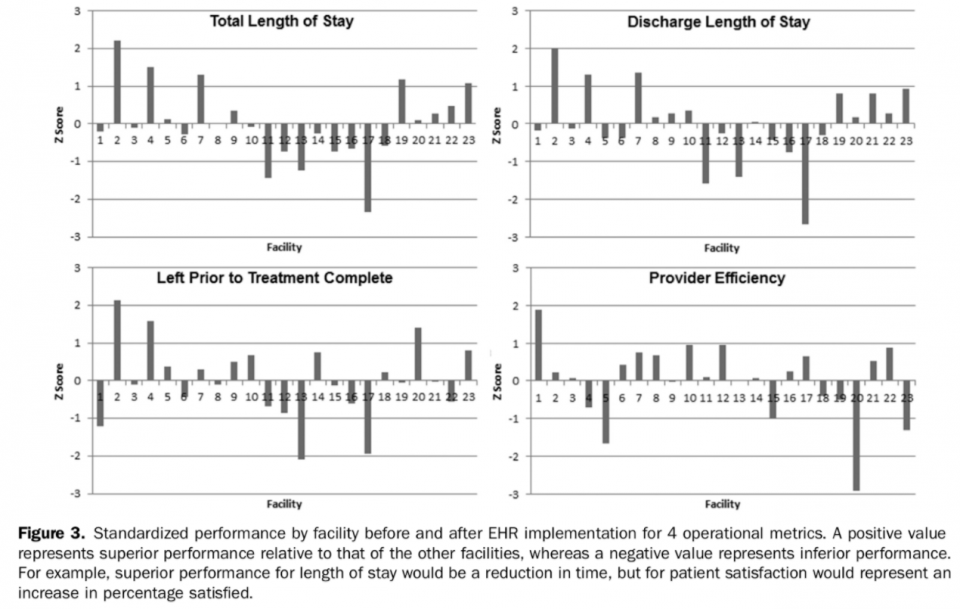
Ward et al. (2014) attempted to answer this question by sharing the experiences of 23 different community Emergency Departments as they launched a new electronic health information system. The focus of this study was around departmental flow during the transition, which was primarily measured by patient length of stay. Baseline performance was measured 6 months prior to implementation and compared with performance 12 months after implementation. There were 23 departments observed and 8 different electronic health solutions deployed, providing a somewhat heterogeneous collection of departments to account for real world variation. Previous studies of only a few hospitals had shown a slow-down period of approximately 6 months before return to baseline performance. 9 After averaging results from the 23 departments, the average slow-down of 6 months before a return to baseline remained similar. When looking more closely at the results by Ward et al. (2014), there were also some significant differences between individual departments as demonstrated by the bar graph below.
What’s Next?
What new knowledge can we generate with the capabilities of these new electronic systems? How will more prevalent electronic health information influence the patient’s coming to our department? How might technology allow us to better empower our patients? And finally, how might our workflow continue to transform?
Research
We know research is one of the ways we can continue to make a widespread impact on the Emergency Medicine community. As our information systems become more robust and connected, collaboration may allow us to identify some of the most common emergency presentations within a community, region, province, or even the country. If meaningful data can be captured on this scale, it may be possible to inform public health and primary care initiatives to reduce the prevalence of certain emergency presentations.
At a more focused institutional level, the improved search functions and ability to extract key information needed to answer clinical research questions will also be a valuable asset for local researchers. Integrating research projects within the electronic information system is yet another way to help investigate posed research questions and something that is encountered at The Ottawa Hospital any time a CT Head is ordered from the Emergency Department.
There has also been some recent exploration regarding how clinical decision rules can be incorporated into electronic ordering. In an observational study done by Bookman et al. (2017), they explored trends in ordering of CT Head, C-spine, and CT-PE before and after integration of clinical decision rules within an electronic ordering system. After implementation, the use of CT Head and CT C-spine decreased; CT-PE usage was statistically unchanged. CT usage among physicians who were the highest utilizers at baseline decreased by 14% for all three imaging studies, while average users did not change their practices, and low users increased usage for CT C- spine and CT-PE. As Heitz, Morgenstern, and Milne (2018) note, the absolute decreases were <1% and there is still no way to determine appropriateness of the scans that were eventually ordered. Regardless, in an era of Choosing Wisely and finding ways to reflect on our own practice of medicine, this is certainly an area for further research and evaluation moving forward.
Electronic Literacy
As we move toward a world of more predominant wearable technology and applications to track health, we may begin to see more patients presenting with concerns that we have not seen in the past.
Take for example the iWatch. It now has a feature that sends you an alert if you have tachycardia at rest for 10 minutes. Was it a tachyarrhythmia the watch picked up while they were asleep or just a really bad dream? Either way, they may be coming to the Emergency Department to talk with us about this.
As patients bring us health data stored in their wearables and apps, we are now forced to develop new technological competency as we work with patients to understand their health data and determine whether the information they bring in represents an emergency or not.
Evolving Workflows
Handheld electronics are now more powerful than ever and wearables seem to be here to stay. One particular wearable that never seemed to gain traction was Google Glass, but recently companies have been finding unique applications for this technology – health care included. Imagine if each patient encounter involved everything except the charting afterward? This is exactly what the team at a company called Augmetix are exploring. The provider wears Google Glass connecting them to a scribe on the other end who documents the encounter and generates a note ready for review by the provider at the end of the exchange. 12 Currently it has been implemented into ambulatory settings but it is not hard to imagine it having a role in the fast paced and busy environment of the Emergency Department.
What about discharge instructions? There may come a day where patients not only leave with a paper summary of discharge instructions but instead have a summary sent to an application on their smart device such as the one created by DashMD. The goal behind this application is to not only lay out the plan but also empower patients to follow this plan by connecting them to key resources in the community to support the shared treatment plan. 13
Conclusion
This post has covered a lot of ground and I hope that this overview has been informative and given you some interesting things to think about as we continue to practice Emergency Medicine in an increasingly digital world.
Electronic health information continues to grow in Canada’s provinces and territories. As health information exchanges continue to develop and evolve within our regional location, we need to continue advocating for data exchange that is relevant and readily accessible to us on the front lines of patient care.
The transition to a fully electronic health system within our local Emergency Departments also comes with a number of benefits and new challenges. As this transition takes place, it is necessary to have realistic expectations during its implementation and use a multidisciplinary approach to ensure it is as smooth as possible. The new digital environment will take some getting used to but also provides an opportunity to re-evaluate processes and re-imagine the workflow of a department to make it more efficient. As familiarity with the powerful features of these new tools grows, it will be necessary for each department to take the time to harness the potential it holds so that we can deliver better care for our patients.
Finally, technology is never standing still. As it continues to evolve, it will be important to use it to our advantage so that we can continue generating knowledge, empowering our patients, and innovating health solutions that ultimately enhance the delivery of Emergency Medicine.
References
-
- Canada Health Infoway. (2014, October 24) Accelerating Clinical Interoperability in Canada: A Path Forward. Retrieved from: http:// https://www.infoway-inforoute.ca/en/component/edocman/2329-accelerating-clinical-interoperability-in-canada-the-path-forward-2/view-document?Itemid=101
- eHealth Ontario from: https://www.ehealthontario.on.ca/en/
- MyHealthNS from: https://www.myhealthns.ca/
- Alberta Netcare EHR (2017). The History of the EHR. Retrieved from: http://www.albertanetcare.ca/History.htm
- Alberta Health Services (2017, December). Connect Care: Frequently Asked Questions. Retrieved from: https://www.albertahealthservices.ca/assets/info/cis/if-cis-faq.pdf
- Coffey, C., Wurster, L. A., Groner, J., Hoffman, J., Hendren, V., Nuss, K., Haley, K., Gerberick, J., Malehorn, B., & Covert, J. (2015). A comparison of paper documentation to electronic documentation for trauma resuscitations at a level I pediatric trauma center. Journal of Emergency Nursing, 41(1), 52-56.
- Handel, D. A., & Hackman, J. L. (2010). Implementing electronic health records in the emergency department. Journal of Emergency Medicine, 38(2), 257-263.
- Ward, M. J., Landman, A. B., Case, K., Berthelot, J., Pilgrim, R. L., & Pines, J. M. (2014). The effect of electronic health record implementation on community emergency department operational measures of performance. Annals of emergency medicine, 63(6), 723-730.
- Risko, N., Anderson, D., Golden, B., Wasil, E., Barrueto, F., Pimentel, L., & Hirshon, J. M. (2014, September). The impact of electronic health record implementation on emergency physician efficiency and patient throughput. In Healthcare (Vol. 2, No. 3, pp. 201-204). Elsevier.
- Bookman, K., West, D., Ginde, A., Wiler, J., McIntyre, R., Hammes, A., Carlson, N., Steinbruner, D., Solley, M. & Zane, R. (2017). Embedded Clinical Decision Support in Electronic Health Record Decreases Use of High Cost Imaging in the Emergency Department: EmbED study. Academic Emergency Medicine.
- Heitz, C., Morgenstern, J., & Milne, W. K. (2018). Hot off the Press: Embedded Clinical Decision Support in Electronic Health Record Decreases Use of High‐cost Imaging in the Emergency Department: EmbED Study. Academic Emergency Medicine, 25(1), 41-43.
- Augmetix from: https://www.augmedix.com/
- DashMD from: http://www.dashmd.co/

