

In this post, we will review the anatomy, essential history, and common presentations of tracheostomy patients in the ED, including obstruction, decannulation, bleeding, tracheal stenosis, and infection.
Anatomy of a tracheostomy tube
- Outer cannula
- Sits directly in the tracheal stoma
- Proximal end designed to allow tube to be easily secured in place
- Distal end may or may not be cuffed
- Inner cannula
- Secured inside the outer cannula by locking mechanisms which vary by brand
- Not present in all types of tracheostomy tube; for example, not used in pediatrics, because it takes off 1 mm from the internal diameter
- Obturator
- Only used to facilitate insertion into the trachea and should be removed immediately after outer cannula is in place
- Can be kept readily available for reinsertion in the event of tracheostomy tube displacement
- Caps
- Used during decannulation process to allow air to travel through the oropharynx
- Never place a cap on a patient with the cuff inflated
Types of tracheostomy tubes
- Cuffed versus uncuffed
- Cuffed tubes are preferred by the American College of Chest Physicians because they allow for positive pressure ventilation (create a seal between trachea and tracheostomy tube)
- Also beneficial for management of secretions and minimizing aspiration
- Addition of the cuff does cause some narrowing of internal diameter
- Cuffed tubes are preferred by the American College of Chest Physicians because they allow for positive pressure ventilation (create a seal between trachea and tracheostomy tube)
- Fenestrated
- Opening on trach allows air to pass up the larynx to allow phonation
- Sizing
- Not standardized between models or manufacturers
- Shiley very different from Portex in terms of internal/outer diameter and length of tube at proximal, radial, and distal portions
Indications for a tracheostomy:
- Chronic ventilation
- Upper airway obstruction, typically a mass
- Post-operative total laryngectomy patients
- Failure to protect airway
- Inefficient swallowing
- Ineffective cough mechanism
ED Approach to the Tracheostomy Patient
- Important questions to ask trached patients in the ED can be remembered as 3-2-1W’s

- What (3)?
- What kind of tracheostomy? What size?
- Cuffed or uncuffed?
- What other tracheostomy complications have they had?
- When (2)?
- When was the tracheostomy tube placed?
- Stoma takes 7-10 days to mature
- If decannulated, when did it come out?
- When was the tracheostomy tube placed?
- Why (1)?
- Important to know indications for tracheostomy placement
- Patients with large oropharyngeal masses will have different management strategies than those with difficulty swallowing
- Recent American College of Chest Physicians guidelines recommend that all patients with tracheostomies that present to the emergency department should be managed in the resuscitation area because they can decompensate rapidly
Replacing a Tracheostomy Tube
- Ensure you have proper equipment:
- Tracheostomy tubes – same size and size below
- 6.0 cuffed endotracheal tube
- Suction catheter
- Water based lubricant
- Bougie, nasogastric tube, or tube exchanger
- Trach ties
- Ambu-bag with pediatric and adult masks
- Place the patient supine with a rolled towel under their shoulders to extend the neck
- Preoxygenate the patient via their stoma and mouth
- Examine and assemble the new tracheostomy tube, inserting the obturator
- Apply thin layer of water based lubricant to end of tracheostomy tube, being mindful not to leave large amounts at the end of the tube
- Remove the trach ties and deflate the cuff
- Remove the existing tube with an “out-then-down” movement during exhalation
- Pull it out so it is against the anterior tracheal wall and then pull it down towards the patient’s chest along the anterior wall of the trach
- Insert the new tube into the stoma at a 90-degree angle to the cervical axis such that the end of the trach is against the posterior wall to minimize your chances of creating a false passage
- Promptly remove the obturator and insert the inner cannula
- Secure the trach in place with neck ties and attach to vent if necessary
- Tips and tricks:
- In a crash situation, it is best to have two people doing the procedure to minimize time to oxygenation
- If unable to obtain a tracheostomy of appropriate size, can use 6.0 endotracheal tube cut down to 12 cm; insert no more than 1 cm past the cuff
- If there are concerns about a difficult tube exchange, recommend using a modified Seldinger technique with a Bougie, tube exchanger, or nasopharyngeal endoscope
Common ED Presentations for Tracheostomy Patients
Obstruction
- Most commonly reported acute complication with an incidence around 2.5%
- Higher risk of mucous plugging because of thick secretions
- Thicker because they lose the moistening and warming effects of the nasopharynx
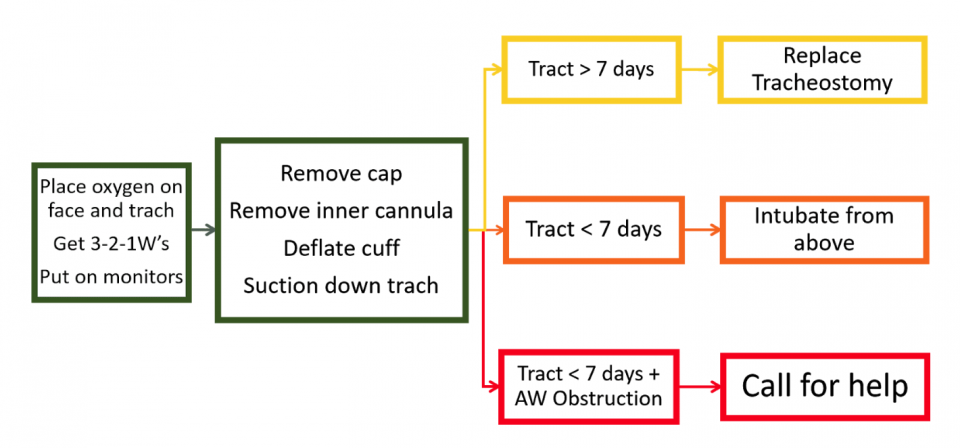
- Place oxygen on patient’s face and tracheostomy site
- Get history if possible
- Remove any caps, remove the inner cannula, and deflate the cuff if present
- Suction down the trach and reassess; this should be effective most of the time
- If no improvement or unable to pass suction through the tracheostomy:
- If tract is older than 7 days, plan to remove and replace tracheostomy
- If unable to obtain a tracheostomy of appropriate size, can use 6.0 endotracheal tube; insert no more than 1 cm past the cuff
- If tract is younger than 7 days, plan to intubate from above
- Intubate as per your normal practice
- Ensure to cover the stoma post-intubation to maintain seal
- If tract is younger than 7 days AND have an upper airway obstruction
- Prepare for difficult intubation, page Anesthesia, page ENT, and if possible obtain a fiberoptic scope
- Remove the tracheostomy tube. This is crucial. An obstructed tracheostomy tube is not a patent airway, and there is no benefit from keeping it in place but potential for significant harm.
- Use LMA or pediatric bag mask to create a seal and bag over the stoma
- Consider using a nasopharyngeal scope with an endotracheal tube to enter the stoma like a fiberoptic intubation
- If tract is older than 7 days, plan to remove and replace tracheostomy
Decannulation
- Important to re-insert tracheostomy promptly
- Even stoma’s greater than one week old can become stenosed by more than 50% within 12 hours of decannulation
- May need dilation if having difficulty re-inserting tracheostomy, so consider calling ENT first if patients are stable and decannulated for greater than 8 hours
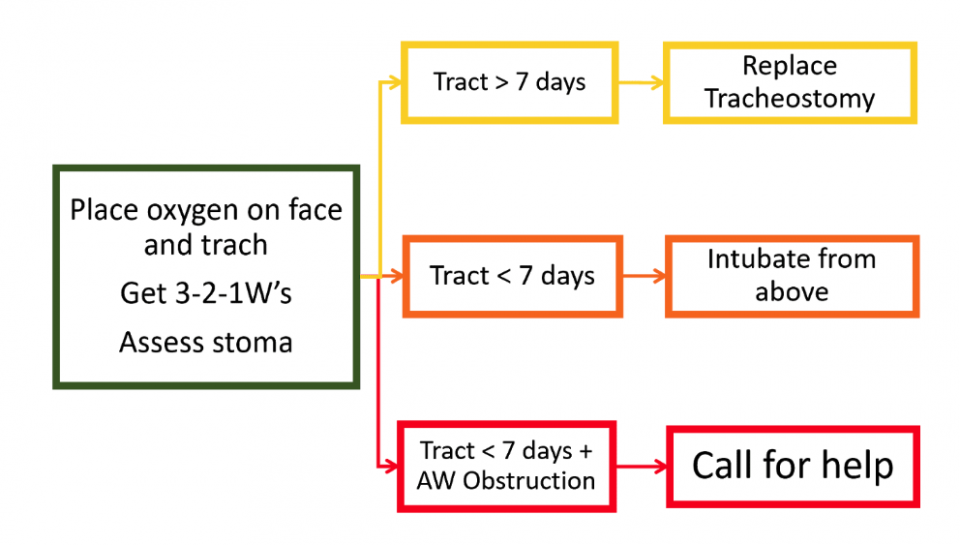
- Place oxygen on patient’s face and tracheostomy site
- Assess the stoma and the patient
- If patient is stable and maintaining their oxygenation and ventilation, have airway equipment close by and discuss with ENT
- If unstable:
- If tract is older than 7 days, plan to replace tracheostomy
- If tract is younger than 7 days, plan to intubate from above
- If tract is younger than 7 days AND have an upper airway obstruction:
- Prepare for difficult intubation, page Anesthesia, page ENT, and if possible obtain a fiberoptic scope
- Use LMA or pediatric bag mask to create a seal and bag over the stoma
Bleeding
- All patients with bleeding from the tracheostomy must be seen by ENT in the department prior to discharge
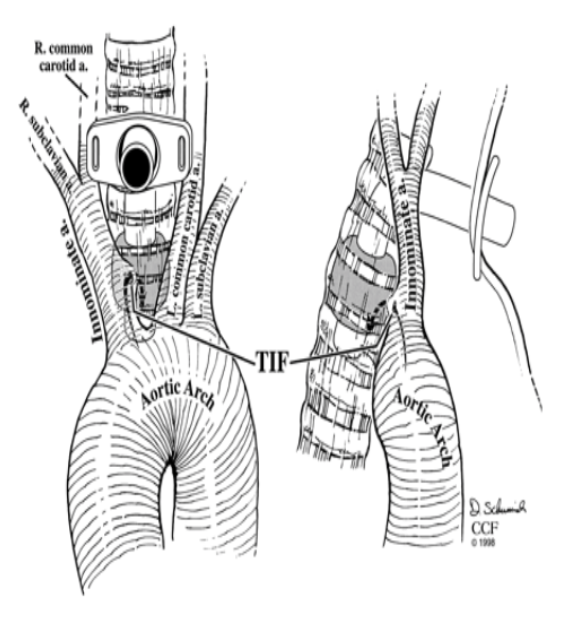
- Most concerning complication is the development of a tracheoinnominate fistula (TIF)
- Pressure from tracheostomy tip or cuff erodes into the innominate artery that lies anterior to the trachea
- Occurs in 0.7% of tracheostomy patients
- Can develop acutely and chronically; 78% occur between week 3 and 4 post-tracheostomy
- Typically present with mild, sentinel bleed within a week of a major bleed
- More common in younger patients compared to the average tracheostomy patient population (31.20 years vs 68.27 years)
- If the patient is stable, CT angiography is needed to make the diagnosis
- The emergent surgery itself carries a 50% mortality rate; the overall survival rate is 14.3%
- All tracheostomy bleeds should be assumed TIF until proven otherwise
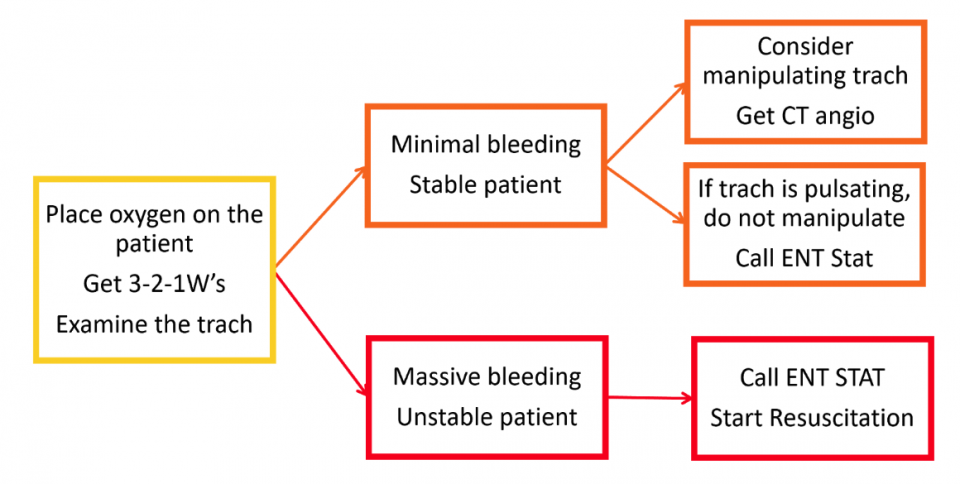
- Place oxygen on patient’s face and assess the tracheostomy site
- If the bleeding is minimal/controlled, consider mildly manipulating the trach. Be cautious as this can acutely worsen the bleeding. If you see a pulsating tracheostomy tube, do not manipulate it.
- If you see bleeding granulation tissue at the stoma, could consider applying silver nitrate to stop it
 If massive bleed, call ENT stat and start resuscitative measures (IV access, fluids/blood)
If massive bleed, call ENT stat and start resuscitative measures (IV access, fluids/blood)- If the trach has a cuff, inflate it with 5.0 cc of air
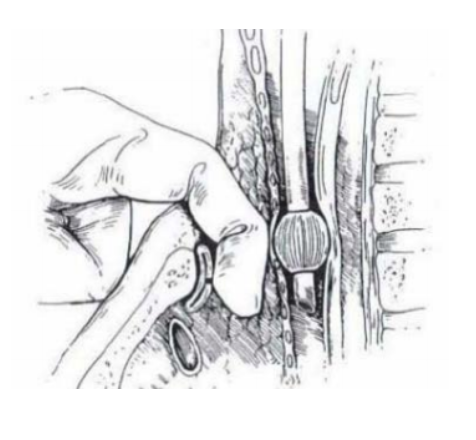
- If still ongoing bleeding, gently withdraw the trach and apply anterior pressure
- If there is no cuff or bleeding continues, prepare to intubate from above. Withdraw the trach and insert a finger into the stoma and down the trachea to hook and pull it anteriorly against the sternum.
- Consider inserting a Foley catheter and suturing it in place if you are the only physician (this frees you to perform other interventions)
Tracheal Stenosis
- Narrowing of the lumen due to scar tissue at, above, or below the level of the stoma
- Recurrent stomal infection increases the likelihood of subglottic stenosis
- Typically have slow, progressive symptoms like difficulty clearing secretions, increasing cough, or dyspnea on exertion
- A concerning feature would be stridor because it typically occurs once the lumen is less than 5 mm
- If a patient presents in respiratory distress, and stenosis is likely a factor, intubation from above will also be difficult
- Diagnosis can be made by laryngoscopy, flexible fiberoscopy, or CT scan
- Thankfully, symptomatic stenosis occurs in less than 12% of patients because it is only an issue once the lumen narrows 50-75%; it is typically diagnosed prior to acute deterioration
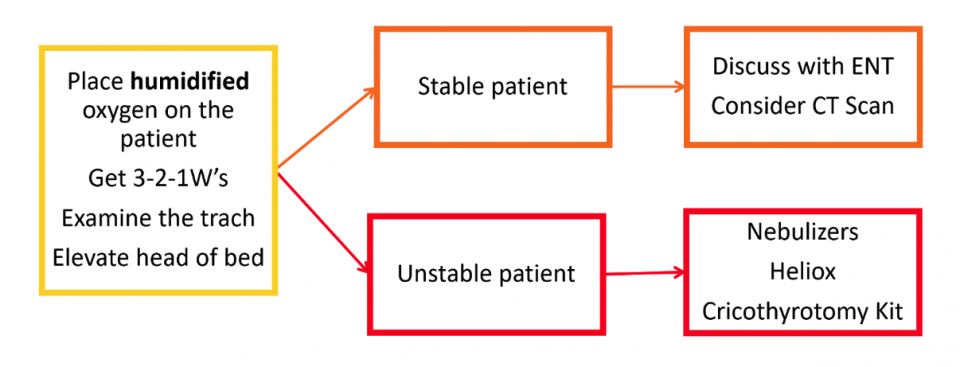
- Management strategies:
- Elevate the head of the bed
- Place high-flow humidified oxygen on both their oral airway and stoma
- Consider nebulized bronchodilators or racemic epinephrine to loosen secretions and minimize edema
- Consider using Heliox to allow better laminar flow through the narrowed airway
- Have cricothyrotomy kit available
Infection
- Occurs as: tracheitis, cellulitis around the stoma, or ventilator associated pneumonia
- Typically caused by pathogenic oropharyngeal flora that colonize the airway
- For stomal infections, good wound care with silver containing products should be used
- Typical organisms include: Staphylococcus aureus, Pseudomonas, Acinetobacter, and other mixed oral flora
- Have low threshold for chest x-ray in patients with stoma infections because of higher risk of pneumonia and progression to severe infections like mediastinitis or osteomyelitis of the clavicles
- Often require broad spectrum intravenous antibiotics and admission
- Would recommend starting broad spectrum like Vancomycin and Pip-tazo which will cover gram positives, MRSA, and pseudomonas
- Looking to see if there are previous cultures with sensitivities doesn’t always work because its often new pathogenic bacteria that disrupts their normal flora that causes the infection
- Consider Candida albicans infection in immunocompromised patients, or with persistent infection despite adequate antibacterial coverage
General Tips and Summary:
- Tracheostomy history – ask the 3-2-1W’s
- Oxygenation is the number one priority!
- Securing the airway is only necessary if oxygenation is becoming an issue
- Ensure oxygen is applied to both airways
- Use an LMA or pediatric bag mask to create a seal and bag over the stoma
- Suction only after removing the inner cannula
- A non-functioning tracheostomy should be promptly removed
- All tracheostomy bleeds are TIF until proven otherwise
- If you diagnose a stomal infection think chest x-ray
References
- De Leyn P, Bedert L, Delcroix M, Depuydt P, Lauwers G, Sokolov Y, et al. Tracheotomy: clinical review and guidelines. Eur J Cardio-Thorac Surg Off J Eur Assoc Cardio-Thorac Surg. 2007;32(3):412–421.
- Goldenberg D, Ari EG, Golz A, et al. Tracheotomy complications: a retrospective study of 1130 cases. Otolaryngol Head Neck Surg 2000;123:495-500.
- Grant CA, Dempsey G, Harrison J, Jones T. Tracheo-innominate artery fistula after percutaneous tracheostomy: three case reports and a clinical review. Br J Anaesth 2005;1(96):127–31.
- Greenwood, JC and Winters, ME. “Chapter 7 – Tracheostomy Care” Roberts and Hedges’ Clinical Procedures in Emergency Medicine and Acute Care (7th ed.). Philadelphia, PA: W.B. Saunders (2017). Accessed via ClinicalKey.com
- Hsu YC, Huang YC, Hsu CW. Tracheocarotid artery fistula: An unusual cause of tracheostomy bleeding. QJM. 2015;11:210.
- Inaba, Kenji. “Bleeding Tracheostomy.” Essentials of Emergency Medicine. Sept 2016. www.facebook.com/EssentialsofEM/videos/1163679590380038/
- Long, B. “Managing the Tracheostomy Patient” Emergency Physicians Monthly. Published on November 4, 2016. www.epmonthly.com/article/managing-tracheostomy-patient/
- Long B, Koyfman A. Resuscitating the tracheostomy patient in the ED. American Journal of Emergency Medicine 2016;34:1148-1155.
- McGrath BA, Bates L, Atkinson D, Moore JA. National Tracheostomy Safety Project. Multidisciplinary guidelines for the management of tracheostomy and laryngectomy airway emergencies. Anaesthesia 2012 Sep;67(9):1025-41.
- Scalise P, Prunk SR, Healy D, Votto J. The incidence of tracheoarterial fistula in patients with chronic tracheostomy tubes: a retrospective study of 544 patients in a long-term care facility. Chest 2005;128(6):3906–9.
- Starmer, H. “A practical approach to tracheostomy tubes and ventilators”. American Speech-Language-Hearing Association. Convention 2007. Accessed online at: www.asha.org/Events/convention/handouts/2007/1651_Starmer_Heather_3
- Townsley RB, Baring DE, Clark LJ. Emergency department care of a patient after a total laryngectomy. Eur J Emerg Med 2014 Jun;21(3):164-9.
- Vaidya N Strauchler D Guelfguat M. Computed tomography angiography diagnosis of tracheo-innominate fistula: a case report and review of literature. Quant Imaging Med Surg 2013; 3:121–5.
- Weingart S. Podcast 195 – Management of Tracheostomy (Trach) and Laryngectomy Emergencies. EMCrit Blog. Published on March 20, 2017. Accessed on April 18th 2018. Available at [https://emcrit.org/racc/tracheostomy-emergencies/]


This is an informative & concise reference.
I am a nurse and unfortunately also a trached ventilator patient.
Living in a rural Wisconsin community, its been in my best interest to teach and help train our volunteer EMTS and local paramedics.
This article will be an asset for those working in the field as well as in the ER.
Thank you.
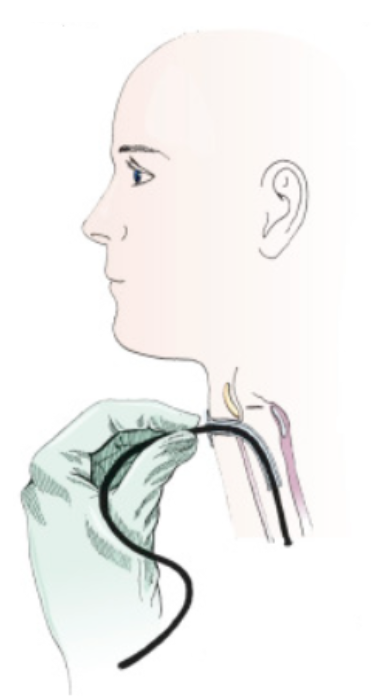
Hello, I am an otolaryngology resident. Thank you so much for writing this article. I just wanted to make a few comments regarding the difference between a tracheostomy and a laryngectomy. The picture at the top of the article actually displays a patient with a laryngectomy stoma, which is not the same as a typical tracheostomy. This is important because a patient with a total laryngectomy has had their voice box removed and no longer has a connection between their trachea and their mouth or nose (ie, they are a neck-breather). It is impossible to intubate these patients from above, so this is an incredibly important distinction to make. In addition, under the headings “Indications for a tracheostomy”, post operative total laryngectomy patients are listed. Again, it is important to note that these patients do NOT have a typical tracheostomy. They have a laryngectomy, or sometimes called an “end tracheo-stoma”, though this term is not typically used as it can be confusing. The opening in their neck is their ONLY airway and this is an important note to make in education.
Thank you for making this comment. I am a Respiratory Therapist and was going to make the same points. The initial picture is of a laryngectomy tube and is completely different from a tracheostomy tube.
Heya.
In order to save time we had a mist machine at the hospital in question where I worked. I trained to be a tracheotomy nurse. I used a blue pen in addition to make some brief summary notes on each single patient. I made urgent referrals if needed. Good luck. I love to read your posts by the way. They are helpful to read.
I also talked to their families in question here. Part of my role was to offer more advice to families of a baby with a tracheostomy tube. I worked really hard. Often I gave out free leaflets. And I also handed out information sheets as well. Leaflets help.
Other helpful tips include a working camera in any case. It is a good idea to talk to a pulmonary doctor. He or she can provide tips on getting a sleep study done and so on. Also see if someone can help with other matters.