

Chest pain is a common presenting complaint to Emergency Departments (ED) worldwide. Massive resource investment is required to differentiate benign from sinister causes of chest pain, and for the treatment, referral, and risk stratification of chest pain patients. A cardiac etiology of chest pain is found in roughly 15% of those presenting to EDs. Emergency Physicians use a combination of history, physical, ECG, and biochemical markers of cardiac injury to diagnose acute coronary syndromes (STEMI, NSTEMI, and unstable angina). The biomarkers used to diagnose acute coronary syndrome have evolved greatly over the last 50 years, changing from relatively non-specific biomarkers such as AST, LDH, myoglobin, Creatine Kinase (CK), and CK-MB, to the very sensitive and specific cardiac troponin assays.
As healthcare spending continues to rise it becomes increasingly necessary to critically appraise the utility of routine testing practices. For example, does your institution order chest pain “Bundles”? Every chest pain patient presenting to our institution gets a total creatine kinase and a troponin ordered at least once. Does the creatine kinase change our ability to diagnose and manage ACS in the ED?
Physiology of Troponin and Creatine Kinase: simplified for emergency medicine brains!
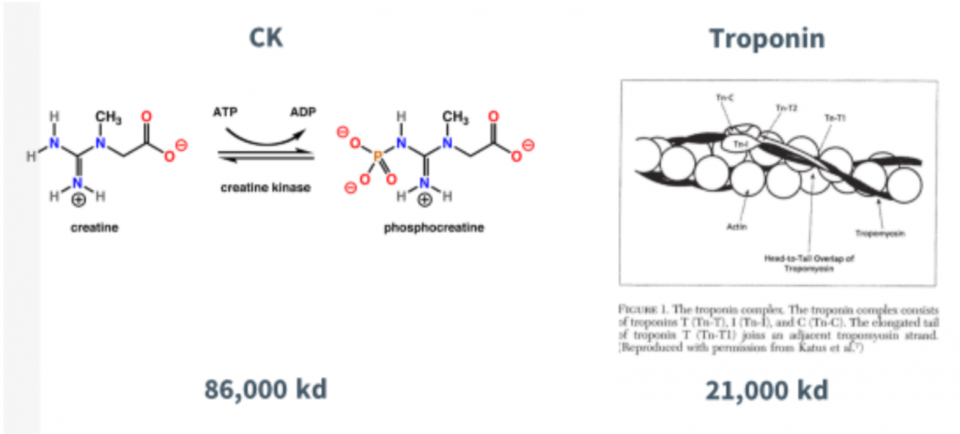
There are different flavours of troponin (I, C and T) and they modulate the calcium-mediated interaction between actin and myosin in skeletal and cardiac muscle tissue.
Briefly, a nerve impulse causes calcium to be released in muscle cells of the heart. This calcium binds the Troponin subunit which is bound to tropomyosin. This causes a physical change in the tropomyosin and allows myosin to bind actin; the resulting interaction leads to muscle contraction. The action of myosin requires ATP, therefore, energy released from ATP powers muscle contraction. Creatine Kinase’s role is to replenish ATP stores, converting ADP back into ATP via conversion of phosphocreatine to creatine. So, we can see that creatine kinase and troponin are intimately related to muscle contraction.
The unique cardiac specific troponin I (cTnI) and cardiac troponin T (cTnT) can be detected by blood tests.
There are also different types of creatine kinase such as CK-muscle and CK-brain that we historically measured. These assays are no longer available to us; our hospital currently measures total CK –which is expressed in all sorts of muscle types in the body, decreasing specificity and utility. HAVE YOU EVER BEEN TO CROSSFIT?
A few questions about Creatine Kinase
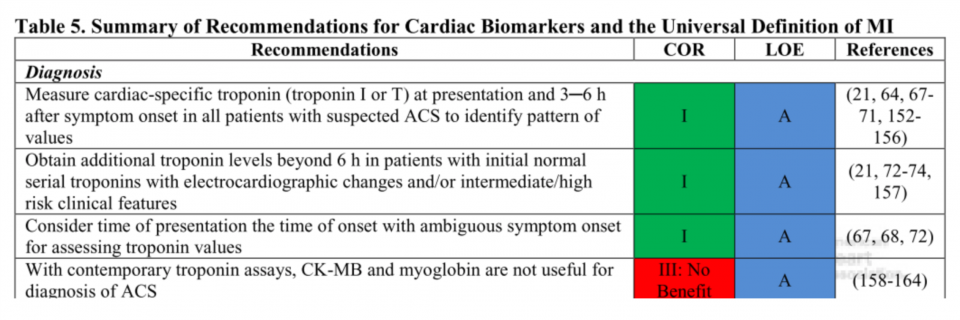
1. Do the European Society of Cardiology (ESC), American College of Cardiology (ACC), or American Heart Association (AHA) recommend ordering both troponin and CK when considering the diagnosis of ACS?
NO!
Cardiac troponins are more sensitive and specific markers of cardiomyocyte injury than creatine kinase (CK), its MB isoenzyme (CK-MB), and myoglobin.
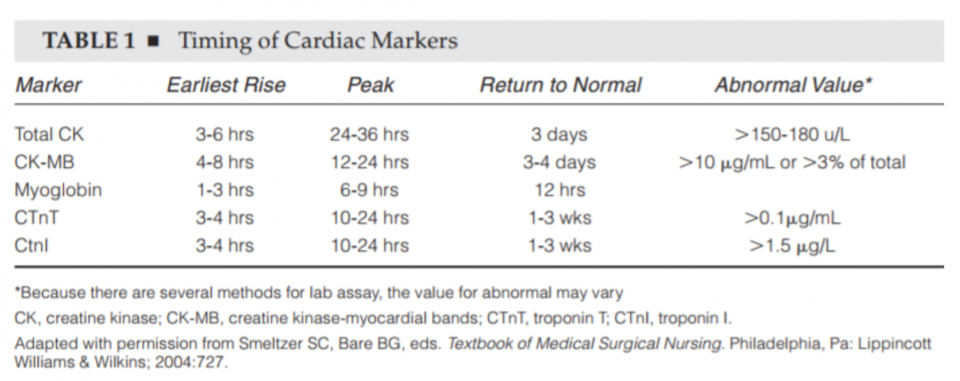
 2. Does Creatine Kinase rise earlier than Troponin?
2. Does Creatine Kinase rise earlier than Troponin?
NO!
Why does this matter?
Local data suggests that our institution orders approximately 92,000 troponins a year across two hospital sites, and roughly 87,000 concurrent CK assays.
That’s ~ 87,000 tests that are of dubious value.
Criticism: Some may say “Well, CK tells us more about the infarct size and because the size of the infarct is the largest predictor of mortality in ACS we need to order CK”
Let’s do a thought experiment:
Imagine that CK was useful and it could help tell us where the infarct occurred and how much damage was done. Imagine a chart that said for a given value of CK there would be a certain reduction of LV function.
That would be useful right?
If only such an investigation existed… wait a second, what about an ECHO? An ECHO tells you what part of a patient’s heart was hit and how much damage occurred. There is no chart or table that says “CK of whatever number is going to result in this much heart failure and therefore they need an ICD for prevention of arrhythmia.”
We can continue this logic… imagine the following 2 patients who present with 5 hours of chest pain and ECGs that are not indicative of STEMI.

Do these numbers change our ultimate medical management or disposition in the ED? Well, Patient 1 gets medical management and Patient 2 gets PCI right?
NO, we treat the patient in front of us. The downstream investigations and therapies are tailored on a case-by-case basis.
- Troponin is a more sensitive and specific biomarker. It also tells you about infarct size!
- There are no head to head trials comparing a CK value to a troponin value and their ability to accurately predict future development of heart failure
- We know that BOTH higher CK and higher troponin levels generally mean bigger infarcts! Furthermore, troponin also tells you about small infarcts too—THAT’S WHY WE INVENTED IT
- There is a ton of evidence showing that a CK (-) , Troponin (+) patient has a very real increased mortality rate
What about a discordant biomarker?
E.g. A patient where the CK came back positive and the troponin came back negative.
- CK is 4x larger than a troponin molecule. Why then would it ever leak out of an ischaemic cell when troponin does not?
- The release kinetics of these molecules are similar when a cell becomes ischaemic. They therefore rise in the same time frame
- Stay tuned for a systematic review on discordant biomarkers!
- Spoiler alert—the evidence consistently shows troponin is more sensitive and more specific
- Local data involving over 1000 patients has not shown a CK (+) and a Troponin (-) that led to a diagnosis of ACS
In Summary:
- Health care spending is rising every year
- Chest pain is a common emergency presentation
- CK is useless for the screening of ACS; use troponin
- If the troponin is elevated: decide on the type of ACS (eg. Type 1 or Type 2 (supply demand)), treat, and refer accordingly
- CK is useful in predicting who is going to get an AKI after they attend crossfit, not who is having a heart attack
References
Abadie, J. M. (2002). Cardiac injury markers and a failed algorithm: can accurate assessment of acute myocardial infarction be cost effective? Military Medicine, 167(8), 683–687. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi T=JS&PAGE=reference&D=med4&NEWS=N&AN=12188242%5Cnhttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed5&NEWS=N&AN=2002287478
Abadie, Jude, Military, & Medicine. (2002). Cardiac injury markers and a failed algorithm: Can accurate. Nursing & Allied Health Database Pg, 167(8). Retrieved from http://search.proquest.com.proxy.bib.uottawa.ca/docview/217050650/fulltextPDF/F2255DE449014CD8PQ/1?accountid=14701
Alan HB. (1999). Biochemical markers of cardiac damage: from traditional enzymes to cardiac-specific proteins WUa for IFCC Subcommittee on Standardization of Cardiac Markers (S-SCM). ScandJClin Lab Invest, 59(Suppl230), 74–82. Retrieved from https://regroup-production.s3.amazonaws.com/documents/ReviewReference/37595428/1999_-_Alan_H_B_Wu_-_BiochemicalmarkersofcardiacdamageFromtraditionalen%5Bretrieved-2017-08-21%5D.pdf?AWSAccessKeyId=AKIAIH6DLCYZGRZ772MQ&Expires=1507047812&Signature=%2BiHwif6bjo2LPzKV0A6QV%2BZJ%2FTs%3D
AlKhenizan, A., & Evans, M. F. (2000). What tests for suspected myocardial infarction? Serum cardiac troponin I or creatine kinase? Canadian Family Physician, 46(8). Retrieved from http://www.cfp.ca/content/46/8/1585.long
Almeda, F. Q., Calvin, J. E., Parrillo, J. E., Sun, F. G., & Barron, J. T. (2001). Prevalence of angiographically significant stenosis in patients with chest pain and an elevated troponin I level and normal creatine kinase and creatine kinase-MB levels. American Journal of Cardiology, 87(11), 1286–1289. https://doi.org/10.1016/S0002-9149(01)01522-3
Alpert, J. S., Thygesen, K., Antman, E., & Bassand, J. P. (2000). Myocardial infarction redefined–a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. Journal of the American College of Cardiology, 36(3), 959–69. https://doi.org/10.1053/euhj.2000.2305
Amsterdam, E. A., Wenger, N. K., Brindis, R. G., Casey, D. E., Ganiats, T. G., Holmes, D. R., … Yancy, C. W. (2014). 2014 AHA/ACC guideline for the management of patients with non-st-elevation acute coronary syndromes: A report of the American college of cardiology/American heart association task force on practice guidelines. Circulation (Vol. 130). https://doi.org/10.1161/CIR.0000000000000134
Apple, F. S., Johari, V., Hoybook, K. J., Weber-Shrikant, E., Davis, G. K., & Murakami, M. M. (2003). Operationalizing cardiac troponin I testing along ESC/ACC consensus guidelines for defining myocardial infarction: Increasing rate of detection [1]. Clinica Chimica Acta, 331(1–2), 165–166. https://doi.org/10.1016/S0009-8981(03)00120-7
Apple, F. S., & Saenger, A. K. (2013). The State of Cardiac Troponin Assays: Looking Bright and Moving in the Right Direction. Clinical Chemistry, 59(7), 1014–1016. https://doi.org/10.1373/clinchem.2013.203307
Aviles, R. J., Wright, R. S., Aviles, J. M., Mcdonald, F., Ballman, K., Harker-Murray, A., … Jaffe, A. S. (n.d.). Long-Term Prognosis of Patients With Clinical Unstable Angina Pectoris Without Elevation of Creatine Kinase But With Elevation of Cardiac Troponin I Levels. Retrieved from http://ac.els-cdn.com.proxy.bib.uottawa.ca/S0002914902027121/1-s2.0-S0002914902027121-main.pdf?_tid=c0ce934e-9803-11e7-8288-00000aab0f01&acdnat=1505252935_7fc8520dca8e8588de7fc2b897f1e6e9
Aviles, R. J., Wright, R. S., Aviles, J. M., McDonald, F., Ballman, K., Harker-Murray, A., … Jaffe, A. S. (2002). Long-term prognosis of patients with clinical unstable angina pectoris without elevation of creatine kinase but with elevation of cardiac troponin i levels. The American Journal of Cardiology, 90(8), 875–878. Retrieved from http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=12372578
B.R., M., & J.S., A. (2002). Diagnosis of myocardial injury by biochemical markers: Problems and promises. Cardiology in Review, 10(5), 306–317. https://doi.org/10.1097/01.CRD.0000027247.58164.6A
Babuin, L., & Jaffe, A. S. (2005). Troponin: the biomarker of choice for the detection of cardiac injury. CMAJ : Canadian Medical Association Journal = Journal de l’Association Medicale Canadienne, 173(10), 1191–202. https://doi.org/10.1503/cmaj/051291
Balk, E. M., Ioannidis, J. P. A., Salem, D., Chew, P. W., & Lau, J. (2001a). Accuracy of biomarkers to diagnose acute cardiac ischemia in the emergency department: A meta-analysis. Annals of Emergency Medicine, 37(5), 478–494. https://doi.org/10.1067/mem.2001.114905
Balk, E. M., Ioannidis, J. P. A., Salem, D., Chew, P. W., & Lau, J. (2001b). Accuracy of biomarkers to diagnose acute cardiac ischemia in the emergency department: A meta-analysis. Annals of Emergency Medicine, 37(5), 478–494. https://doi.org/10.1067/mem.2001.114905
Ben-Dor, I., Hasdai, D., Behar, S., Zahger, D., Leor, J., Hammerman, H., … Gottlieb, S. (2006). Prognostic implications of increased cardiac biomarkers and ST segment depression in non-ST elevation acute coronary syndromes: lessons from the acute coronary syndrome Israeli survey (ACSIS) 2002. Heart (British Cardiac Society), 92(4), 547–548. https://doi.org/10.1136/hrt.2005.069625
Brooks, G. C., Lee, B. K., Rao, R., Lin, F., Morin, D. P., Zweibel, S. L., … Olgin, J. E. (2016). Predicting Persistent Left Ventricular Dysfunction Following Myocardial Infarction the PREDICTS Study. Journal of the American College of Cardiology, 67(10), 1186–1196. https://doi.org/10.1016/j.jacc.2015.12.042
Brown, C. S., & Bertolet, B. D. (1997). Cardiac troponin: See ya later, CK! Chest, 111(1), 2–4. https://doi.org/10.1378/chest.111.1.2
Chia, S., Senatore, F., Raffel, O. C., Lee, H., Wackers, F. J. T., & Jang, I. K. (2008). Utility of Cardiac Biomarkers in Predicting Infarct Size, Left Ventricular Function, and Clinical Outcome After Primary Percutaneous Coronary Intervention for ST-Segment Elevation Myocardial Infarction. JACC: Cardiovascular Interventions, 1(4), 415–423. https://doi.org/10.1016/j.jcin.2008.04.010
Christenson, R H; Newby, L K; Ohman, E. M. (1997). Cardiac markers in the assessment of acute coronary syndromes. Baltimore: Maryland medical Journal.
Collinson, P. O., Gaze, D. C., Morris, F., Morris, B., Price, A., & Goodacre, S. (2006). Comparison of biomarker strategies for rapid rule out of myocardial infarction in the emergency department using ACC/ESC diagnostic criteria. Annals of Clinical Biochemistry, 43(Pt 4), 273–80. https://doi.org/10.1258/000456306777695555
Di Chiara, A., Plewka, M., Werren, M., Badano, L. P., Fresco, C., & Fioretti, P. M. (2006). Estimation of infarct size by single measurements of creatine kinase levels in patients with a first myocardial infarction. Journal of Cardiovascular Medicine (Hagerstown, Md.), 7(5), 340–346. https://doi.org/10.2459/01.JCM.0000223256.01439.1b
DJ, K., DL, K., Karras, D. J., Kane, D. L., & D.J., K. (2001). Serum markers in the emergency department diagnosis of acute myocardial infarction. Emergency Medicine Clinics of North America, 19(2), 321–337. Retrieved from http://www.elsevier.com/inca/publications/store/6/2/3/2/9/3/index.htt%5Cnhttp://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=emed5&NEWS=N&AN=2001185398%5Cnhttp://ezproxy.library.usyd.edu.au/login?url=http://search.ebscohost.com/login.aspx?direct=true
Dolci, ☆ A, & Panteghini, M. (2006). The exciting story of cardiac biomarkers: From retrospective detection to gold diagnostic standard for acute myocardial infarction and more. https://doi.org/10.1016/j.cca.2006.02.042
Ferguson, J. L., Beckett, G. J., Stoddart, M., Walker, S. W., & Fox, K. a a. (2002). Myocardial infarction redefined: the new ACC/ESC definition, based on cardiac troponin, increases the apparent incidence of infarction. Heart (British Cardiac Society), 88(4), 343–347. https://doi.org/10.1136/heart.88.4.343
Goodman, S. G., Steg, P. G., Eagle, K. A., Fox, K. A. A., López-Sendón, J., Montalescot, G., … Gurfinkel, E. P. (2006). The diagnostic and prognostic impact of the redefinition of acute myocardial infarction: Lessons from the Global Registry of Acute Coronary Events (GRACE). American Heart Journal, 151(3), 654–660. https://doi.org/10.1016/j.ahj.2005.05.014
Graven, T., Kruger, O., & Bronstad, G. (2001). Epidemiological consequences of introducing new biochemical markers for detection of acute myocardial infarction. Scandinavian Cardiovascular Journal, 35(4), 233–237. https://doi.org/10.1080/14017430152581332
Halkin, A., Stone, G. W., Grines, C. L., Cox, D. A., Rutherford, B. D., Esente, P., … Mehran, R. (2006). Prognostic implications of creatine kinase elevation after primary percutaneous coronary intervention for acute myocardial infarction. Journal of the American College of Cardiology, 47(5), 951–961. https://doi.org/10.1016/j.jacc.2005.12.003
Hallén, J. (2012). Troponin for the estimation of infarct size: What have we learned? Cardiology, 121(3), 204–212. https://doi.org/10.1159/000337113
Hasdai, D., Behar, S., Boyko, V., Danchin, N., Bassand, J.-P., & Battler, A. (2003). Cardiac biomarkers and acute coronary syndromes–the Euro Heart Survey of Acute Coronary Syndromes Experience. European Heart Journal, 24(13), 1189–94. https://doi.org/10.1016/S0195-668X(03)00204-5
Jaffe, A. S. (2013). Third Universal Definition of Myocardial Infarction. Clinical Biochemistry, 46(1–2), 1–4. https://doi.org/10.1016/j.clinbiochem.2012.10.036
Jesse, E., & Vickie, A. (1998). Cardiac biomarkers : Past , present , and future.
Keffer, J. H. (1996). Myocardial Markers of Injury. Evolution and Insights. American Journal of Clinical Pathology, 105 (3), 305–320. Retrieved from https://watermark.silverchair.com/api/watermark?token=AQECAHi208BE49Ooan9kkhW_Ercy7Dm3ZL_9Cf3qfKAc485ysgAAAfIwggHuBgkqhkiG9w0BBwagggHfMIIB2wIBADCCAdQGCSqGSIb3DQEHATAeBglghkgBZQMEAS4wEQQMGaU6Ey7WBF2x8AzDAgEQgIIBpR-18yqGtC9_ZKlSXR8WLkdPyqpITpBFhfyyST_ulMLdj
Korff, S., Katus, H. A., & Giannitsis, E. (2006). Differential diagnosis of elevated troponins. Heart, 92(7), 987–993. https://doi.org/10.1136/hrt.2005.071282
Le, R. D., Kosowsky, J. M., Landman, A. B., Bixho, I., Melanson, S. E. F., & Tanasijevic, M. J. (2015). Clinical and financial impact of removing creatine kinase-MB from the routine testing menu in the emergency setting. American Journal of Emergency Medicine, 33(1). https://doi.org/10.1016/j.ajem.2014.10.017
Leibundgut, G., Gick, M., Morel, O., Ferenc, M., Werner, K.-D., Comberg, T., … Neumann, F.-J. (2016). Discordant cardiac biomarker levels independently predict outcome in ST-segment elevation myocardial infarction. Clinical Research in Cardiology, 105(5), 432–440. https://doi.org/10.1007/s00392-015-0938-9
Lim, J. Hawkins, R.C., Ng, K. Chan, S.P., Cheng, A. NG, K. S. (2002). A Preliminary Study of the utility of combined cardiac markers in the evaluation of patients presenting early with suspected acute coronary syndrome. Annals of Academic Medicine Singapore, 31, 772–6.
Mair, J., Morandell, D., Genser, N., Lechleitner, P., Dienstl, F., & Puschendorf, B. (1995). Equivalent early sensitivities of myoglobin, creatine kinase MB mass, creatine kinase isoform ratios, and cardiac troponins I and T for acute myocardial infarction. Clinical Chemistry, 41(9), 1266–1272.
Newby, L. K., Jesse, R. L., Babb, J. D., Christenson, R. H., Fer, T. M. De, Diamond, G. A., … Weintraub, W. S. (2012). ACCF 2012 expert consensus document on practical clinical considerations in the interpretation of troponin elevations: A report of the American College of Cardiology Foundation Task Force on clinical expert consensus documents. Journal of the American College of Cardiology, 60(23), 2427–2463. https://doi.org/10.1016/j.jacc.2012.08.969
Newby, L. K., Roe, M. T., Chen, A. Y., Ohman, E. M., Christenson, R. H., Pollack, C. V., … Peterson, E. D. (2006). Frequency and clinical implications of discordant creatine kinase-MB and troponin measurements in acute coronary syndromes. Journal of the American College of Cardiology, 47(2), 312–318. https://doi.org/10.1016/j.jacc.2005.08.062
Newby, L. K., Storrow, A. B., Gibler, W. B., Garvey, J. L., Tucker, J. F., Kaplan, A. L., … Ohman, E. M. (2001). Clinical Investigation and Reports Bedside Multimarker Testing for Risk Stratification in. Circulation, 1832–1837.
Nusier, M. K., & Ababneh, B. M. (2006). Diagnostic efficiency of creatine kinase (CK), CKMB, troponin T and troponin I in patients with suspected acute myocardial infarction. Journal of Health Science, 52(2), 180–185. https://doi.org/10.1248/jhs.52.180
Panteghini, M., Cuccia, C., Bonetti, G., Giubbini, R., Pagani, F., & Bonini, E. (2002). Single-point cardiac troponin T at coronary care unit discharge after myocardial infarction correlates with infarct size and ejection fraction. Clinical Chemistry, 48(9), 1432–1436.
Penttila, I., Penttila, K., & Rantanen, T. (2000). Laboratory diagnosis of patients with acute chest pain. Clinical Chemistry and Laboratory Medicine, 38(3), 187–197. https://doi.org/10.1515/CCLM.2000.027
Pichot, S., Mewton, N., Bejan-Angoulvant, T., Roubille, F., Rioufol, G., Giraud, C., … Ovize, M. (2015). Influence of cardiovascular risk factors on infarct size and interaction with mechanical ischaemic postconditioning in ST-elevation myocardial infarction. Open Heart, 2(1), e000175. https://doi.org/10.1136/openhrt-2014-000175
Rao, S. V., Ohman, E. M., Granger, C. B., Armstrong, P. W., Gibler, W. B., Christenson, R. H., … Newby, L. K. (2003). Prognostic value of isolated troponin elevation across the spectrum of chest pain syndromes. American Journal of Cardiology, 91(8), 936–940. https://doi.org/10.1016/S0002-9149(03)00107-3
Roger, V. L., Weston, S. A., Gerber, Y., Killian, J. M., Dunlay, S. M., Jaffe, A. S., … Jacobsen, S. J. (2010). Trends in incidence, severity, and outcome of hospitalized myocardial infarction. Circulation, 121(7), 863–869. https://doi.org/10.1161/CIRCULATIONAHA.109.897249
Rosalki, S. B., Roberts, R., Katus, H. A., Giannitsis, E., & Ladenson, J. H. (n.d.). Cardiac Biomarkers for Detection of Myocardial Infarction: Perspectives from Past to Present. https://doi.org/10.1373/clinchem.2004.041749
Rubini Giménez, M., Hoeller, R., Reichlin, T., Zellweger, C., Twerenbold, R., Reiter, M., … Mueller, C. (2013). Rapid rule out of acute myocardial infarction using undetectable levels of high-sensitivity cardiac troponin. International Journal of Cardiology, 168(4), 3896–3901. https://doi.org/10.1016/j.ijcard.2013.06.049
Sandoval, Y., Smith, S. W., Thordsen, S. E., & Apple, F. S. (2014). Supply/demand type 2 myocardial infarction should we be paying more attention? Journal of the American College of Cardiology, 63(20), 2079–2087. https://doi.org/10.1016/j.jacc.2014.02.541
Shavadia, J., Zheng, Y., Dianati Maleki, N., Huber, K., Halvorsen, S., Goldstein, P., … Armstrong, P. W. (2015). Infarct Size, Shock, and Heart Failure: Does Reperfusion Strategy Matter in Early Presenting Patients With ST-Segment Elevation Myocardial Infarction? Journal of the American Heart Association, 4(8), e002049. https://doi.org/10.1161/JAHA.115.002049
Singh, G., & Baweja, P. S. (2014). Creatine Kinase–MB The Journey to Obsolescence. Am J Clin Pathol, 141, 415–419. https://doi.org/10.1309/AJCPBIK3G4BWEJKO
Sobel, B. E., & Lewinter, M. M. (2000). Ingenuous interpretation of elevated blood levels of macromolecular markers of myocardial injury: A recipe for confusion. Journal of the American College of Cardiology, 35(5), 1355–1358. https://doi.org/10.1016/S0735-1097(00)00516-7
Stokke, M., Gronvold, T., Siebke, A. M., Skjaeggestad, O., & Stromme, J. H. (1998). Serial measurements of cardiac markers to rule in or out acute myocardial damage less than 3 h after admission in acute chest pain patients without ECG-signs of acute myocardial infarction. Scand J Clin Lab Invest, 58(4), 331–338. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9741821
Storrow, A. B., Lindsell, C. J., Han, J. H., Slovis, C. M., Miller, K. F., Gibler, W. B., … Pollack, C. V. (2006). Discordant cardiac biomarkers: frequency and outcomes in emergency department patients with chest pain. Annals of Emergency Medicine, 48(6), 660–5. https://doi.org/10.1016/j.annemergmed.2006.05.016
Turer, A. T., Mahaffey, K. W., Gallup, D., Weaver, W. D., Christenson, R. H., Every, N. R., & Ohman, E. M. (2005). Enzyme estimates of infarct size correlate with functional and clinical outcomes in the setting of ST-segment elevation myocardial infarction. Current Controlled Trials in Cardiovascular Medicine, 6, 12. https://doi.org/10.1186/1468-6708-6-12
Williams, S. G., Silas, J. H., Joseph, F., Jackson, M., Rittoo, D., & Currie, P. (2004). Troponin T: how high is high? Relationship and differences between serum cardiac markers according to level of creatine kinase and type of myocardial infarction. Postgraduate Medical Journal, 80(948), 613–4. https://doi.org/10.1136/pgmj.2003.016253
Wong, S. (1996). Strategic utilization of cardiac markers for the diagnosis of acute myocardial infarction. Annals of Clinical & Laboratory Science, 26(4), 301–312. Retrieved from http://www.annclinlabsci.org/content/26/4/301.short
Wu, Apple, Gibler, Jesse, Warshaw, and Valdes, JrBiochemistry, N. A. of C. (1998). Recommendations for the Use of Cardiac Markers In Coronary Artery Diseases: NACB. Chicago, IL.
Yan, A. T., Yan, R. T., Tan, M., Chow, C. M., Fitchett, D., Stanton, E., … Goodman, S. G. (2004). Troponin is more useful than creatine kinase in predicting one-year mortality among acute coronary syndrome patients. European Heart Journal, 25(22), 2006–2012. https://doi.org/10.1016/j.ehj.2004.08.010
Yee, K. C., Mukherjee, D., Smith, D. E., Kline-Rogers, E. M., Fang, J., Mehta, R. H., … Eagle, K. A. (2003). Prognostic significance of an elevated creatine kinase in the absence of an elevated troponin I during an acute coronary syndrome. American Journal of Cardiology, 92(12), 1442–1444. https://doi.org/10.1016/j.amjcard.2003.08.055
Younger, J. F., Plein, S., Barth, J., Ridgway, J. P., Ball, S. G., & Greenwood, J. P. (2006). Troponin-I concentration 72 h after myocardial infarction correlates with infarct size and presence of microvascular obstruction. Heart, 93(12), 1547–1551. https://doi.org/10.1136/hrt.2006.109249

