

In the Emergency Department (ED) we’re always thinking about the “ABC’s”. You’ve also probably heard of “DEFG: Don’t Ever Forget Glucose”. This usually refers to hypoglycemia in our critically ill patients—those with decreased level of consciousness, new onset seizures, sepsis, and so on. But what about hyperglycemia? Much ink has been spilled over diabetic ketoacidosis (DKA), and the related entity hyperosmolar hyperglycemic state (HHS), but many patients present with hyperglycemia without meeting criteria for these clinical entities. How do you treat them? Fluids? Insulin? If so, how much? How do you plan their disposition? Let’s take a look at some of the evidence supporting our management of hyperglycemia in the ED.
Diabetes and hyperglycemia are a frequent chief complaint, representing 1% of ED encounters [1], making it one of the most prevalent chronic diseases we see. These numbers are expected to increase, as Diabetes Canada estimates that prevalence in this country will increase by 44% over the decade leading up to 2025 [2]. As always, our ED population is at higher risk than most. In a recent ED study, 36% of diabetics presenting to the ED have what would be considered “very poor control”, compared to 18% in Endocrinology clinics and 19% in Family Medicine clinics [3]. Although hypoglycemia rates have gone down by 22% in the last five years, hyperglycemia in the ED has been increasing, especially among older adults [4].
Despite these numbers, many emergency physicians find it hard to get fired up over hyperglycemia. In a 2010 multicenter survey, 3/4 of emergency physicians (EP’s) claimed they routinely refer patients with isolated hyperglycemia—but many barriers emerged; the most frequently cited were “limited follow-up”, “insufficient time/resources”, and the feeling it’s “outside our scope of practice” [5].
Intravenous Fluids
Although many EP’s reflexively give a litre or two of crystalloid to reduce blood glucose levels, there is very little literature to support this practice. In a 2014 study from USC Los Angeles [6], patients with an ED glucose > 14 mmol/L were randomized to either a 2L bolus of normal saline or PO water, resulting in a 2h drop of blood glucose of 4.0 and 3.4 mmol/L, respectively. Although the authors conclusion was that “oral and intravenous fluids were equally efficacious in lowering blood glucose levels”, I would suggest that a decrease of 3-4 mmol/L of glucose is unlikely to be clinically significant and that both treatments were equally ineffective. #glasshalfempty
Insulin
We’re not wanting for studies examining insulin for glycemic control on inpatient outcomes or hyperglycemia secondary to other pathology (stroke, cardiac events, sepsis, etc). However, there’s surprisingly little published about administration of insulin for hyperglycemia in the ED. One quasi-experimental study from an academic centre in Chicago [7] used an ED rapid acting insulin protocol with q2h glucose checks to see if it would have an impact on the degree of hyperglycemia, ED and hospital length of stay (LOS), and adverse events including hypoglycemia. The hope was they could reach the goal of a blood glucose <10 mmol/L (as per the American Diabetes Association recommendation) to expedite discharge from the ED. In the end, the more aggressive ED protocol did result in better glycemic control by an additional 5 mmol/L and a 36h reduction in hospital LOS. However, it did not affect ED LOS and the rate of hypoglycemia was 7.4% (or roughly 1 in 14 patients). Insulin is effective, although not without risk!
Discharge Glucose Target
When someone has moderate-severe hyperglycemia without DKA/HHS, what is an appropriate target glucose level before discharge? Many of us have a number in mind (for example, less than 20mmol/L) and presumably we think this will reduce short-term adverse outcomes.
Driver et al. asked if glucose level at time of discharge from the ED was associated with 7-day ED revisits or hospitalization [8]. They looked at 566 encounters over two years of patients with hyperglycemia defined as ≥ 22mmol/L to see if there was an association between discharge glucose and 7-day adverse outcomes including rates of DKA/HHS, repeat ED visits, or admission to hospital for any reason.
The rates of 7-day adverse outcomes are summarized here:
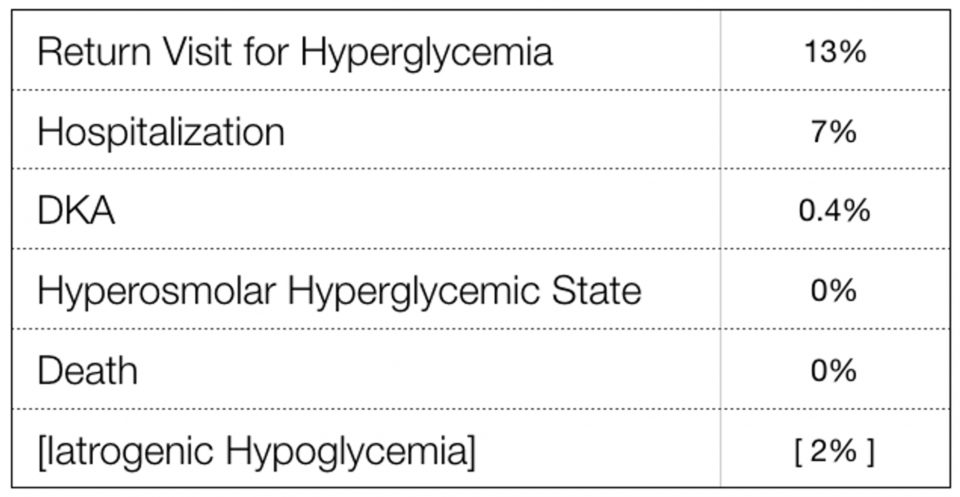
They performed a statistical analysis using something called “generalized estimation equations” to adjust for confounders, and found that an elevated discharge glucose level was not associated with increased risk of repeat ED visit or hospitalization within 7 days. This was still the case even with a dichotomous analysis at a threshold of 19.4 mmol/L for “low” and “high” glucose discharge levels. So it seems there’s no rationale for the arbitrary target of “less than 20 mmol/L” for a safe discharge home. While it’s important to remember that this study excluded patients with Type 1 Diabetes, this is the best evidence so far telling us the approach to asymptomatic hyperglycemia, should be focused on ensuring appropriate outpatient follow-up and treatment for long-term glycemic control, instead of aiming for a “safe” glucose threshold before discharge.
This article was also featured in our “Top 10 Most Important Articles of 2016”
More recently, a Canadian study by Yan et al. [9] tried to determine if there were risk factors for repeat ED visits in patients presenting with hyperglycemia from any cause, and this time included Type 1 diabetics. Of the 833 index visits, about half were discharged home, and 156 (19%) of them returned to ED within 30 days. After a regression analysis, they found 5 risk factors and 2 protective factors (all statistically significant), summarized here:
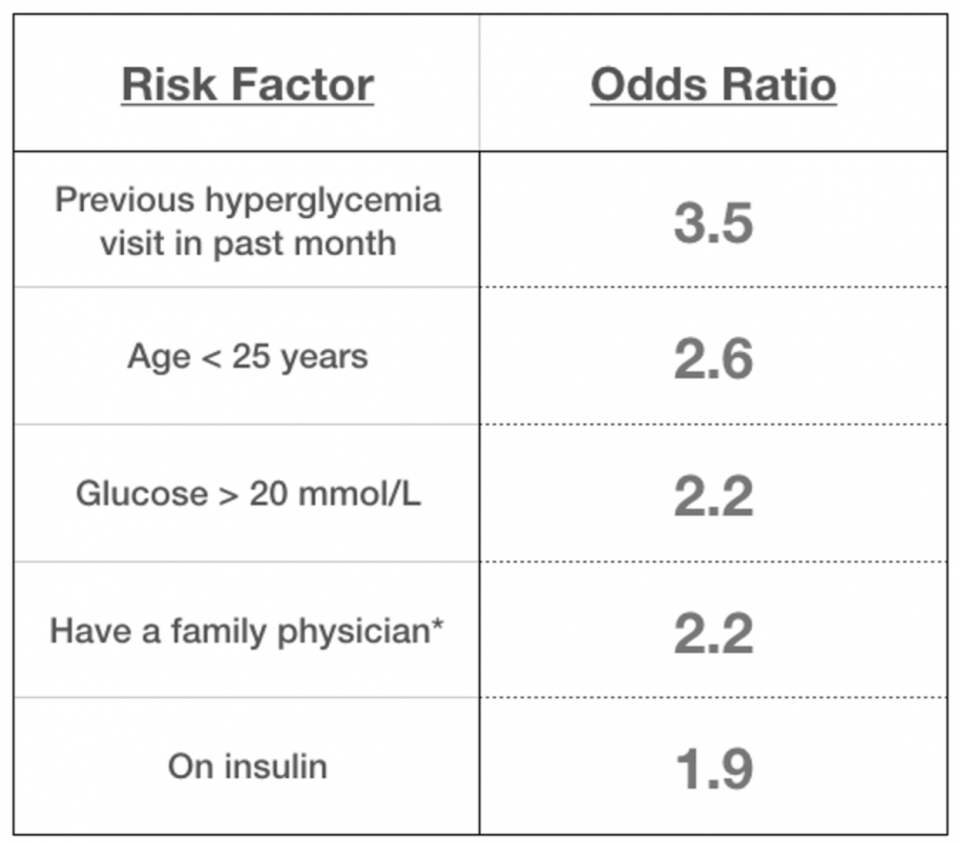
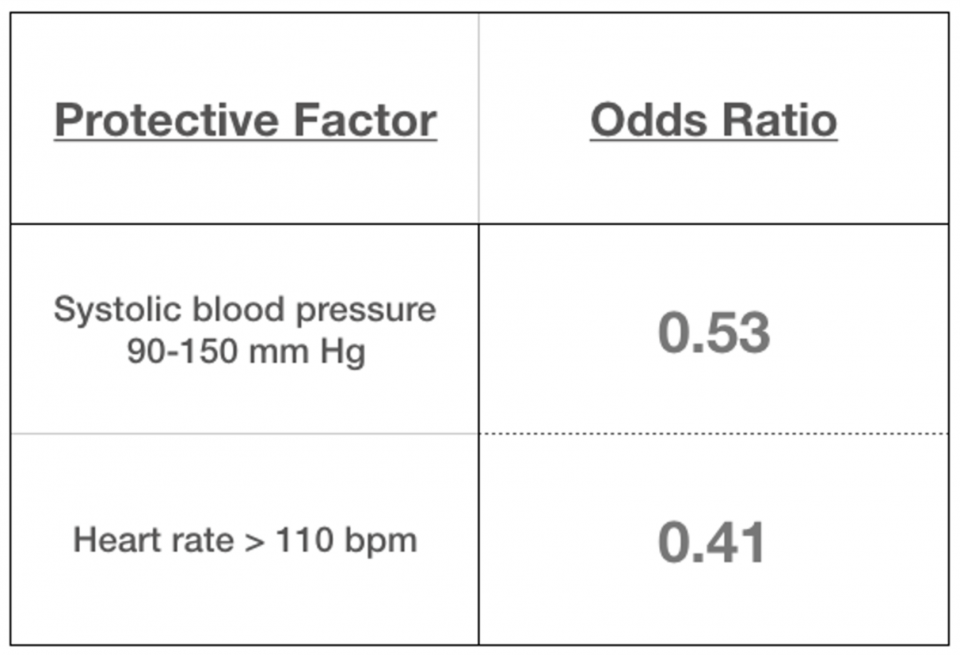
On the surface, this study might seem to argue against the conclusions of the Driver study from Annals—here a discharge glucose >20mmol/L was a risk factor for a return visit. It’s important to note the Yan study included type 1 diabetics and that two thirds of the patients had an index visit because of medication/insulin non-compliance, under-dosing, or poor control. These are potentially modifiable precipitants with some combination of counselling with educational interventions and, maybe most importantly, close follow-up (just like the Driver study suggested).
Summary
- Administration of intravenous crystalloid is probably unnecessary unless the patient is truly volume deplete.
- Insulin is effective for reducing the degree of hyperglycemia, but obviously not without risk.
- In patients with asymptomatic hyperglycemia (without Type 1 DM) who are otherwise well, it is likely safe to discharge home with a blood sugar > 20mmol/L, so long as you can ensure close follow up with a primary care physician.
References
[1] Washington RE, Andrews RM, Mutter R. Emergency Department Visits for Adults With Diabetes, 2010: Statistical Brief #167. Rockville, MD: Agency for Health Care Policy & Research; 2006.
[2] https://www.diabetes.ca/how-you-can-help/advocate/why-federal-leadership-is-essential/diabetes-statistics-in-canada#_ftnref1
[3] Josephsen, G., & Rusnak, R. (2017). Poor glycemic control in diabetic patients seeking care in the ED. The American Journal of Emergency Medicine, 24(6), 721–724.
[4] Wang, J., Geiss, L. S., Williams, D. E., & Gregg, E. W. (2015). Trends in emergency department visit rates for hypoglycemia and hyperglycemic crisis among adults with diabetes, United States, 2006-2011. PLoS ONE, 10(8), 2006–2011.
[5] Ginde, A. A., Delaney, K. E., Pallin, D. J., & Camargo, C. A. (2010). Multicenter survey of emergency physician management and referral for hyperglycemia. The Journal of Emergency Medicine, 38(2), 264–70.
[6] Arora, S., Probst, M. A., Andrews, L., Camilion, M., Grock, A., Hayward, G., & Menchine, M. (2014). A randomized, controlled trial of oral versus intravenous fluids for lowering blood glucose in emergency department patients with hyperglycemia. Cjem, 16(3), 214–219.
[7] Munoz, C., Villanueva, G., Fogg, L., Johnson, T., Hannold, K., Agruss, J., & Baldwin, D. (2011). Impact of a subcutaneous insulin protocol in the emergency department: Rush Emergency Department Hyperglycemia Intervention (REDHI). The Journal of Emergency Medicine, 40(5), 493–8.
[8] Driver, B. E., Olives, T. D., Bischof, J. E., Salmen, M. R., & Miner, J. R. (2016). Discharge Glucose Is Not Associated With Short-Term Adverse Outcomes in Emergency Department Patients With Moderate to Severe??Hyperglycemia. Annals of Emergency Medicine, 68(6), 697–705.e3.
[9] Yan, J. W., Gushulak, K. M., Columbus, M. P., van Aarsen, K., Hamelin, A. L., Wells, G. A., & Stiell, I. G. (2017). Risk factors for recurrent emergency department visits for hyperglycemia in patients with diabetes mellitus. International Journal of Emergency Medicine, 10(1), 23.


Trackbacks/Pingbacks