

Emergency medicine is a diverse specialty. We’ve all had the shift where you go from suturing an elderly woman’s scalp, to managing an anxious patient with chest pain, to running a cardiac arrest as EMS patches in with a trauma. We wear many hats throughout a single shift and it’s the greatest part of our chosen specialty. Perhaps the area we are the most keen on continuously building and expanding upon is our resuscitation skills.
What does it mean to be a resuscitationist? What are the qualities and abilities that encompass a great resuscitationist? How can we remain composed and initiate quality care when faced with the sickest of the sick? When that two-year-old multi-trauma patient arrives at your ED, how will you perform?
To quote Cliff Reid, Emergency Physician / Intensivist and previous Flight Physician with HEMS London, “It’s not enough to know what to do, you have to know how to make it happen.”
In a podcast episode about resuscitation, Dr. Scott Weingart states that, “Amateurs discuss strategy, experts discuss logistics.” Strategy is what you would recite on your oral exams, logistics is the ability to make it happen in real life. The resuscitationist needs to be a master of logistics.
Objectives:
- Recognize and appreciate the important role of human factors and logistics in the resuscitation room
- Go through key logistical issues that are encountered regularly in the three phases of resuscitation – prior to patient arrival, during the resuscitation, and after the patient has left.
- Briefly look at some solutions for these issues and some evidence behind them
- Understand some challenges and limitations of these solutions
- Gain a few key logistical pearls to use on the next shift
Before the Resuscitation Starts
Environment and Equipment Control
Our equipment and our environment define our ability to act in a moment of stress. If you are unfamiliar with a certain chest tube set, you may not be able to use it in the moment. Similarly, with our environment, if there’s no room around the bed to do the FAST exam because 400 people encircle the patient, you may abandon the task or it may be forgotten.
Mary Patterson from Akron, OH implemented an in-situ simulation program in her pediatric ED to detect latent safety threats (LST) that arose around critical patient care. Latent safety issues are “system-based threats to patient safety that are unrecognized by healthcare providers.” Over the course of 90 simulations, they identified 73 latent safety issues, of which 26 (34%) were equipment or environment related.
In the same vein, our centre conducted a similar analysis in 2016. We ran 43 cases of in situ sim in 1 year and identified 147 LST. The majority were knowledge gaps, however, 19% of the time it was related to equipment issues.
Local experience:
- From 2016:
- 43 cases run over 1 year
- Various clinical presentations involving many ED staff
- 147 LST identified
- Majority (45%) resulted from knowledge gaps
- Subdivided into: errors of omission (27%), team lack of awareness (29%), loss of team understanding (14%), incorrect action for problem (15%), incorrectly performed procedure (15%)
- 19% overall resulted from equipment issues
Someone find me the chest tube tray!
Drs. Fan, Petrosoniak, Hicks, and the team at St. Michael’s Hospital in Toronto are undertaking a similar study called TRUST (Trauma Resuscitation Using in-Situ Simulation Team Training) to identify latent safety threats. This includes video-taping 12 unannounced in-situ simulations to conduct a framework analysis and identify targets for intervention.
To highlight the importance of equipment and environment control they used a human tracing tool to follow the footsteps of the treating physician and a nurse. As you can see, we are not standing stoically at the end of the bed like we all think. According to Chris Hicks, “nurses and physicians spend an inordinate amount of time and traverse a surprising distance to collect the relevant clinical equipment.”

For certain procedures, if has been identified that if a specific object is hard to find, implement a procedure bundle for this task. While the patient is deteriorating is not the time to be searching drawers for the cricothyrotomy kit.
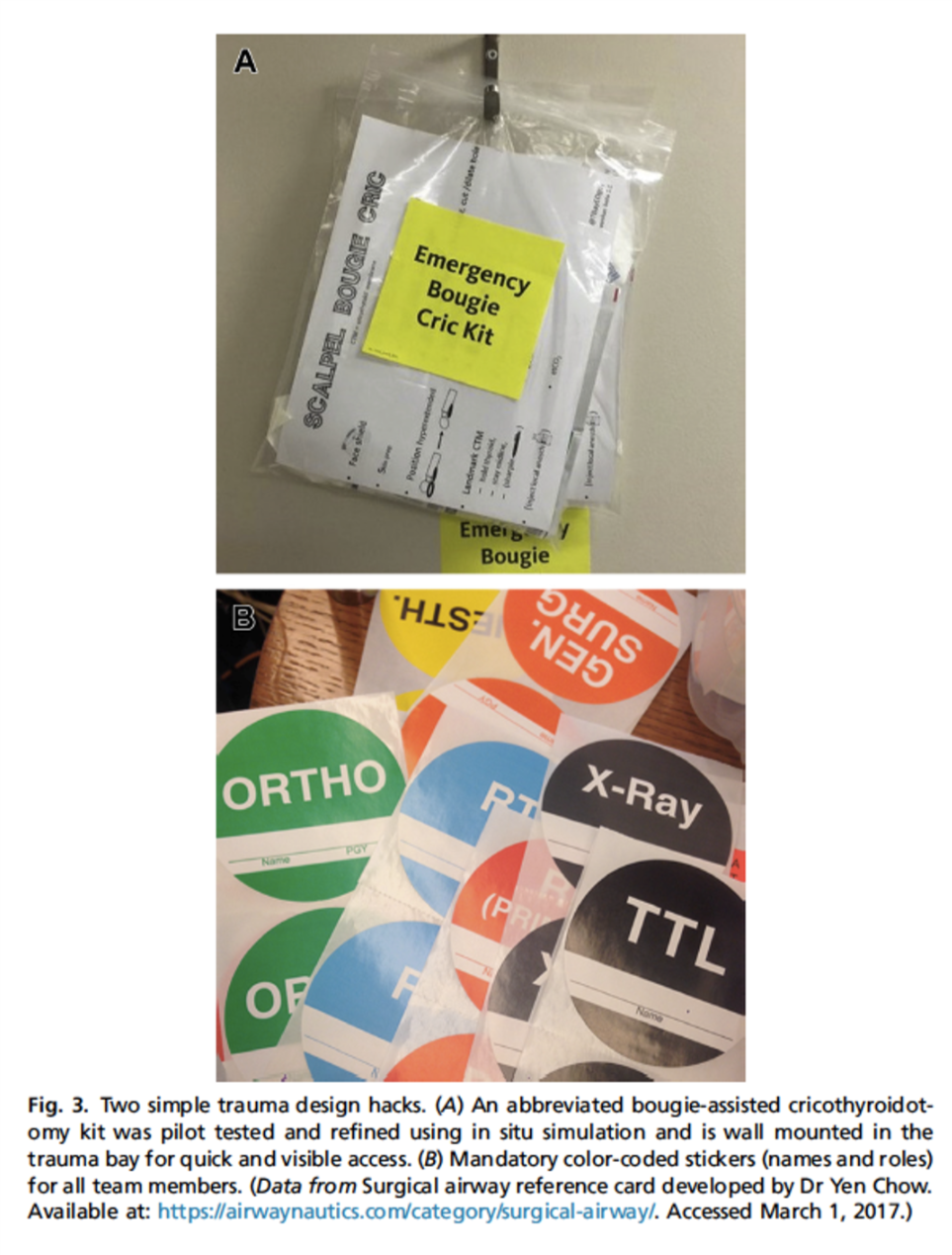
In our own department, we are currently looking into procedure bundles. The resuscitation committee is currently in the finalization stages regarding complete chest tube trays.
Another idea that the resuscitation committee has come up with is the idea of procedure towers which carry all the necessary items needed for common emergent procedures. These are quite expensive however, at about $12,000 each and therefore the cost-benefit ratio will have to be closely scrutinized.
Team Huddle
Football is a game of strategy and logistics. The team would not be in sync and would run an unsuccessful play every time if they did not huddle prior to the play (unless you’re the New England Patriots). So why do we run a resuscitation, which is a team sport, without first going over our plan?

Both logistical and cognitive preparation is extremely helpful in reducing stress and anxiety, allowing the team to act quicker and more synchronously in the moment.
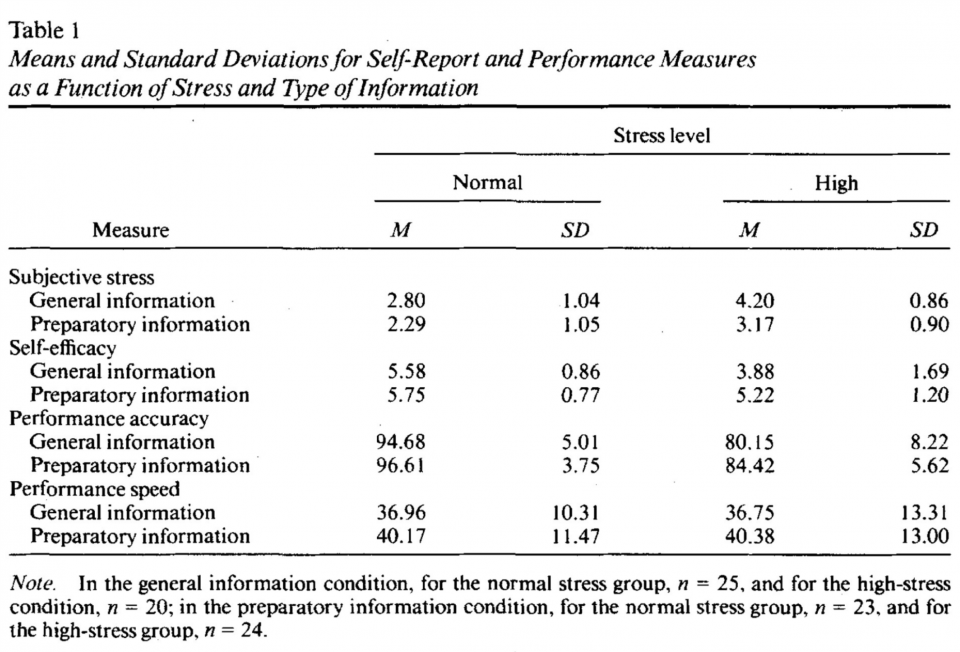
An article by Inzana et al. in the Journal of Applied Psychology looked at the effect of preparatory information on performance of Navy-enlisted personnel during high-stress conditions.
They define three types of preparatory information: sensory, procedural, and instrumental. Sensory information provides information regarding how the individual is likely to feel in the situation. Procedural information describes events that are likely to occur in the stressful environment. For example, prior to parachuting, you may be informed of what occurs prior to jumping, during, and after. Finally, instrumental information describes what to do to counter the undesirable consequences of stress.
They took 92 Navy enlisted personnel at a Navy technical school and subjected them to 2 decision-making computer-based scenarios under normal and high stress environments with either general or preparatory information prior to proceeding.
Those who received preparatory information had less subjective stress, increased confidence, and made fewer performance errors.
The Pre-Briefing
Hicks and Petrosoniak describe a 4-step structured approach to pre-briefing prior to a trauma arrival that should be essential prior to any sick patient arriving in the ED. It is also applicable to medical patients.
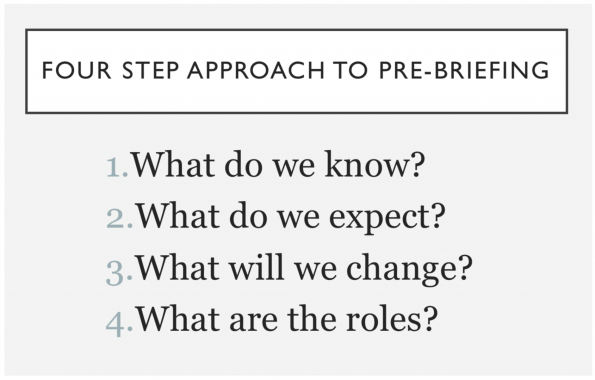
- What do we know:
- Age, situation, known medical history, vitals, issues identified on scene
- What do we expect (Plan A):
- Anticipated problems (i.e. Need for procedures, need for early medications, need for blood)
- What will we change (Plan B):
- Secondary approach including when to deviate from primary approach (2 attempts at IV → IO, 2 attempts at airway → surgical airway)
- Roles:
- Identify anticipated early needs and priorities, assign personnel to each task in alignment with plan (PLAN A = airway team, chest tube insertion, pelvic binder, IV starts, etc.)
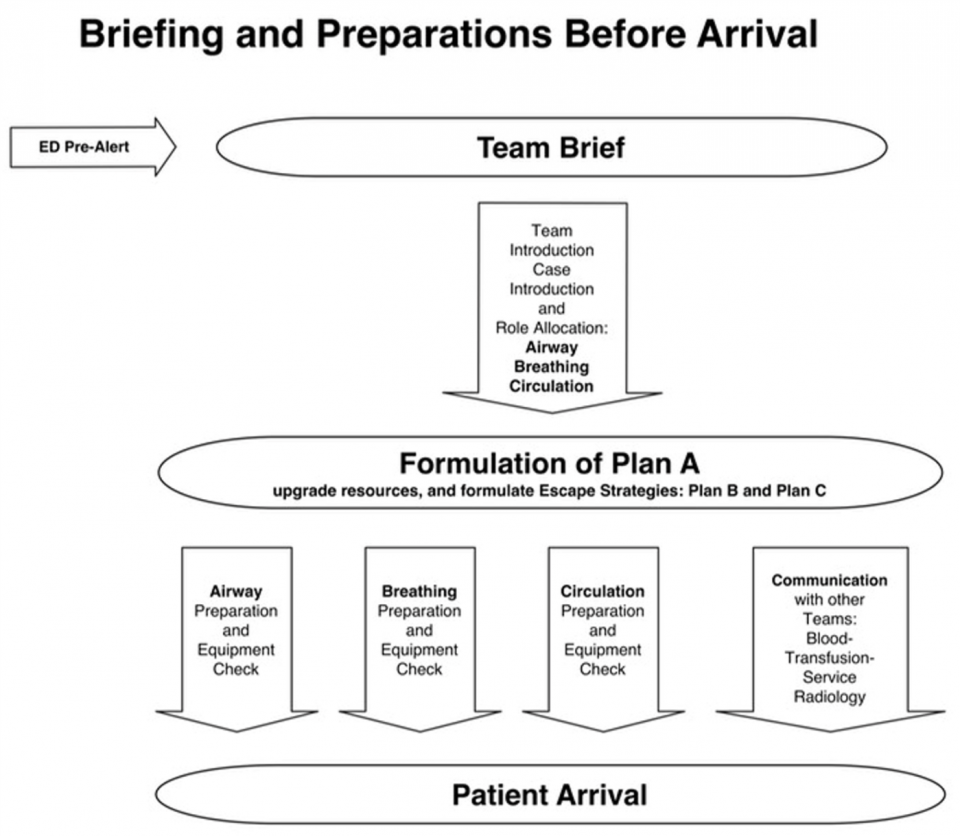
The European Trauma Course has actually published workflows to aid in trauma resuscitation and pre-briefing; this can be used as a model to structure your pre-briefing. It is their belief that pre-briefing can facilitate preparation and establish shared mental models prior to patient arrival which coordinates the team better during the resuscitation.
During the Resuscitation
Cognitive Aids
Cognitive aids are an important part of double-checking and cognitive forcing to avoid commonly forgotten issues in care. They can help integrate safety behaviours into situations where omissions are otherwise more common or the situation is extremely high-stakes.
As everyone can remember going through in medical school and residency, pre-operative checklists are commonplace in the OR. But why is this?
After implementation of the WHO Surgical Safety Checklist, they demonstrated reduction in death rates from 1.5% to 0.8% and decreased serious complication rate from 11% to 7.6% in the OR. So why can’t this concept apply to resuscitation where there is, arguably, more stress and confusion at times, and the acuity is higher.
Arguably, there are few procedures that are higher acuity in medicine than emergency airway management, especially if a difficult airway is predicted. Often, when airways go wrong, it usually not a lack of skill or knowledge required but cognitive overload in a situation of stress which compromises our ability to properly evaluate a situation and recall available rescue strategies. This is often compounded by the inability of the clinical team to function in unison during this stressful event. Rather than failure to prepare, it is often a failure of implementation of rescue techniques that occurs.
Approach to the Failed Airway

In 2016, an anesthesiologist named Dr. Nicholas Chrimes developed the Vortex Approach to airway management. His goal was to create a guidance tool that would be effective in reducing implementation errors in emergency airway management.
Type of Guidance Tools
First, we need to look at the type of guidance tools out there.
- Foundational tools are guidelines, protocols, and procedures that are used for review or knowledge acquisition PRIOR to the event occurring to promote memory. These are often too difficult and cumbersome to use during a high acuity moment.
- Implementation tools are guidance tools designed to be used in the moment during a high stress event. These can be high acuity (e.g. cardiac arrest, difficult airway) or low acuity (e.g. anesthetic machine check, pre-op checklist).
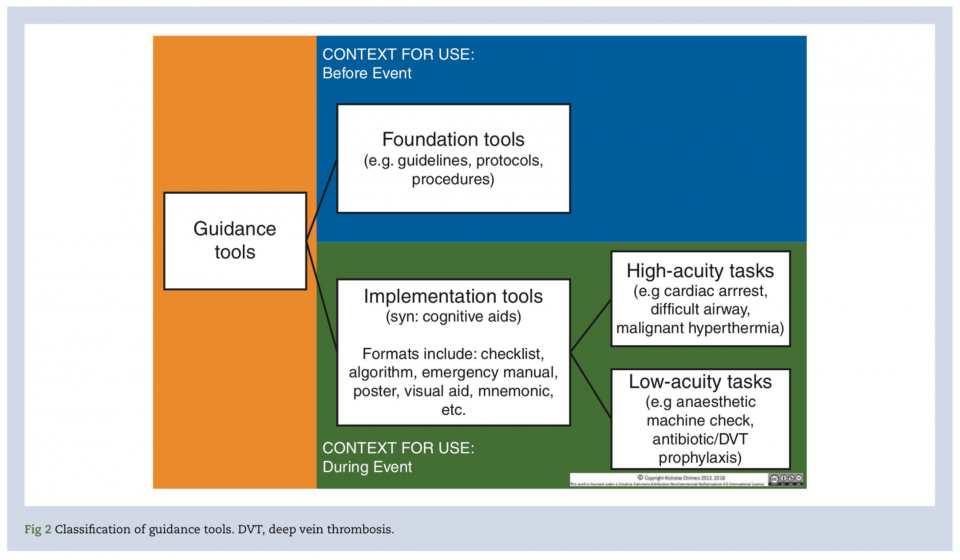
The Vortex airway approach is a high-acuity implementation tool designed to support teamwork and decision making during emergency airway management.
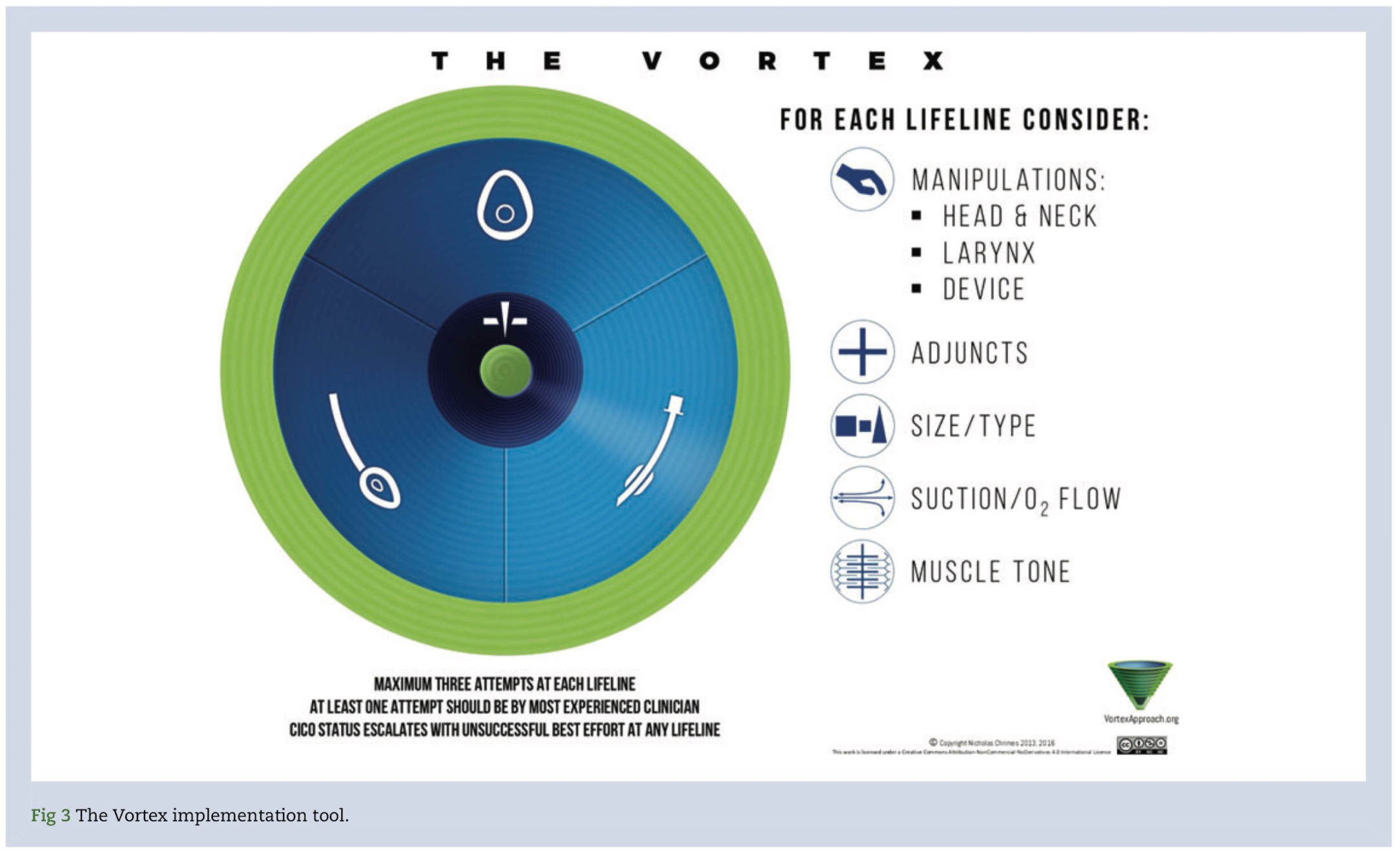
Vortex is based on the principal that there are three non-surgical airway techniques (face mask, supraglottic device, and ETT). If a best effort at each of these three is exhausted a ‘CICO – Can’t intubate, can’t oxygenate’ rescue is initiated. Vortex uses this graphic depicting three zones arranged in a circular fashion around a central area representing the CICO rescue. Green is safe, blue is tenuous and dark blue is CICO situation.
If a ‘best effort’ at any of the three lifelines fails it mandates movement inward to the next lifeline. A best effort has a strict definition which is “up to three attempts, however minimal should be used. Any repeated attempt at a best effort need to have modifications undertaken based on the five optimization categories beside the graphic.” As lifelines fail, you move down the vortex towards the CICO rescue.
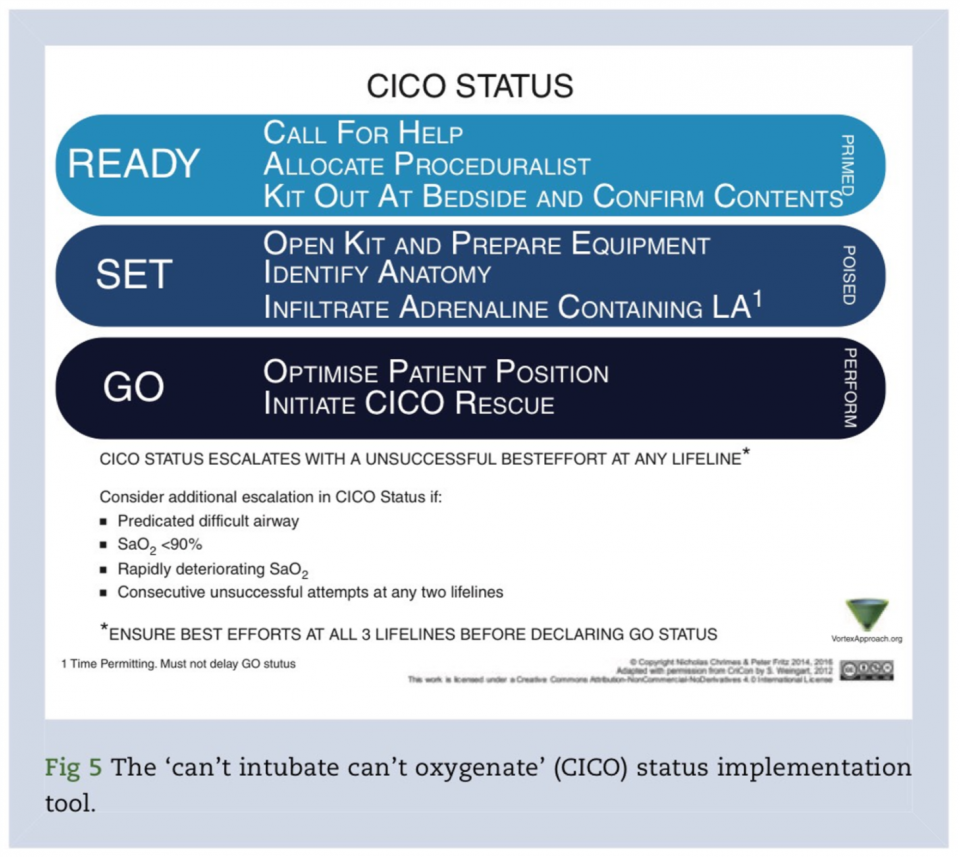
As you exhaust your final lifeline, it is mandated that a CICO rescue is declared. Pre-defined actions then take place in a “ready-set-go” approach.
The Importance of Critical Language
The Vortex tool also provides a common template and language to maintain team situational awareness. Terms such as “green zone” “CICO rescue” “best effort” give context and tag moments as significant. Declaring “green zone status” tells members of the team in few words what the next steps are. It is similar to cardiac arrest management where the terms “no pulse” or “shockable rhythm” tag moments for team members and trigger actions. Common and critical language harmonizes team efforts especially when team members of differing specialities and backgrounds are present which is the norm in the ED
Trauma Checklists
Continuing the theme of checklists I’d like to look briefly at a lower acuity implementation tool, the WHO trauma care checklist. This checklist outlines key patient safety issues that are often forgotten. The list was developed and validated by a large global collaboration and published in the World Journal of Surgery in April 2017.
In the study, they looked at 11 hospitals of variable economic strata, including urban trauma centers in the US and Canada, from 2010-2012 and using a step-wedge pre- and post-intervention comparison they attempted to evaluate the effectiveness of implementing this tool.
They collected data on 1641 patients pre-intervention and 1781 patients post intervention from 11 centers.
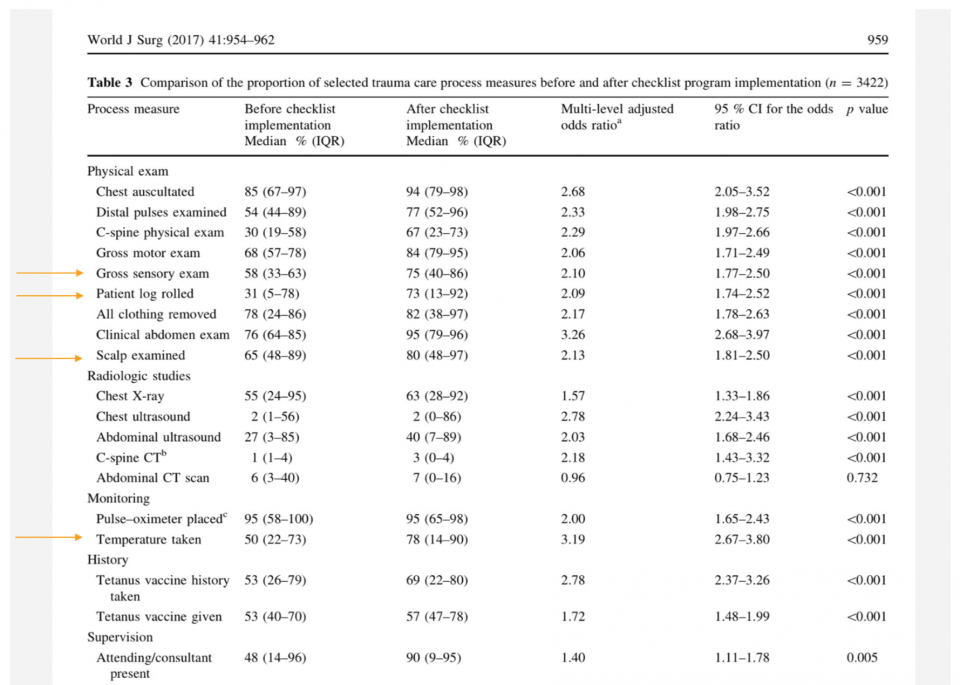
With exception of CT scanning the abdomen, each study process measure improved post-intervention. For example, 85% vs 94% received clinical chest auscultation pre and post, respectively. Commonly forgotten things were less forgotten including 31 vs 73% having a log roll completed, 58% vs 75% having a gross sensory exam completed, 65% vs 80% having a scalp examination performed, and 50 vs 78% having a temperature taken and recorded.
These data seem to indicate that a checklist improves adherence to “standard of care” for trauma patients especially commonly forgotten aspects.
After the Resuscitation
The patient is gone up to the ICU, high fives all around, and another life is saved. You’re off to see your next patient.
But what can we do to ensure we continue to maintain and improve our resuscitation logistics?
Debriefing
Debriefing is defined as “facilitated or guided reflection in the cycle of experiential learning.” It is an important quality improvement and educational tool. It increases team effectiveness and studies have demonstrated increased ROSC rates, improved neuro outcomes, and decreased time delay to first compression with teams that debrief.
However, a needs assessment survey completed in 10 pediatric EDs across Canada in 2013 showed that about half of responders indicated that debriefing occurred less than 25% of the time despite 88% of responders believing it was important. Only 14% indicated that debriefing occurred more than 75% of the time.

Potential barriers identified included:
- ED workload and environment does not allow sufficient time to debrief (90%)
- No interest or need (24%)
- Lack of qualified/trained facilitators (44%)
- No setting available (42.5%)
- Did not feel comfortable discussing the event in the group/team environment (18%)
- Felt criticized and judged (13%)
- Too soon or late after event (28%)
- Lack of admin support for debriefing (32%)
In order to address some of these issues and facilitate debriefing, Kessler et al. outlined a practical approach in 2014 in Annals of Emergency Medicine using a 5Ws/1H approach (WHO, WHAT, WHEN, WHERE, WHY, AND HOW) to create and maintain a standardized debriefing program in your ED.
Key aspects include:
- Determining the:
- Facilitator
- Participants
- Timing
- Location
- Objectives
- Standardized format
Likely, the biggest hurdle is how to discuss all of this? After all, we are trained as physicians, not discussion facilitators. Start with a friendly atmosphere, use open ended questions, honest dialogue, and identify behaviours or perceptions that led to improved outcomes. The goal is to identify targets for intervention, not blame people for mistakes.
There are two common debriefing methods, the plus-delta method and reflective inquiry. Often they are combined.
- “Plus-delta” involves group-based reflection and assessment as to what went well, what did not go well, and what needs to be changed to improve care. The goal is to engage participants in an active assessment of performance and use their observations as starting points to generate discussion on improvements
- Reflective inquiry is a strategy to engage participants in a deeper discussion to uncover rationales for decisions, behaviours, and actions
For example:
- During plus-delta we determine that the incorrect dose of epi is given
- Switching to reflective inquiry we discover WHY the incorrect dose was given
- We then learn from the nurse that dosing was based on pounds not kilograms
- The emphasis is not on the error but on discovering why it happened
There are also many debriefing tools and scripts to help guide facilitators through the process and help bring out key learning objectives.
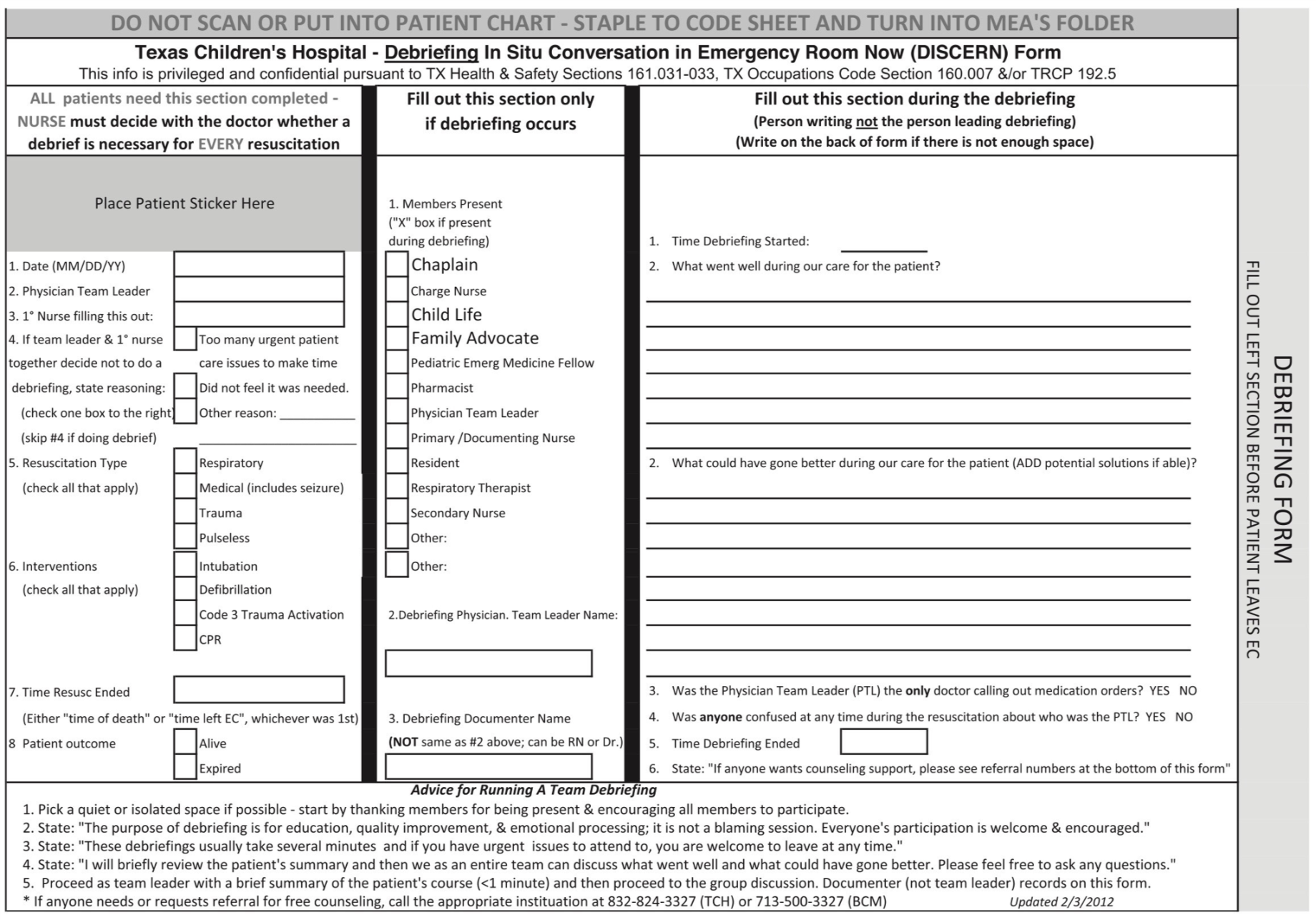
One example of a standardized tool is the DISCERN tool (Debriefing In Situ Conversation after Emergency Resuscitation Now). It gives a template to follow to prompt discussion around the case and generate ideas. It can be useful for novice debriefers to get into the habit of completing the task.
Retrospective Analysis
The final aspect of resuscitation logistics I’d like to discuss is the idea of retrospective or “After-Action” review.
Quoting again from Dr. Scott Weingart, he claims that all good resuscitationists “agonize” over their cases. Meaning they review, dissect, and reflect on cases good as well as bad. One way to do this in a more objective fashion is by video review of cases and identification of latent safety issues and targetable issues for change
A 2017 article in The Journal of Trauma and Acute Care Surgery by Wurster et al., looked at the use of a standardized assessment tool and video review of pediatric trauma primary surveys to improve compliance with ATLS standards. They developed an ATLS Primary Assessment Completion (PACT) tool and graded the performance of staff on completion of standard ATLS procedures for each case.
They looked at 142 videos over a one-year period from various Level 1 trauma centers. After video review and scoring of performances they intervened by implementing intensive educational efforts. These included bimonthly mock traumas, resident education, monthly reviews of scores at trauma performance improvement meetings, and including PACT scores for each surgeon’s ongoing professional practice evaluation.
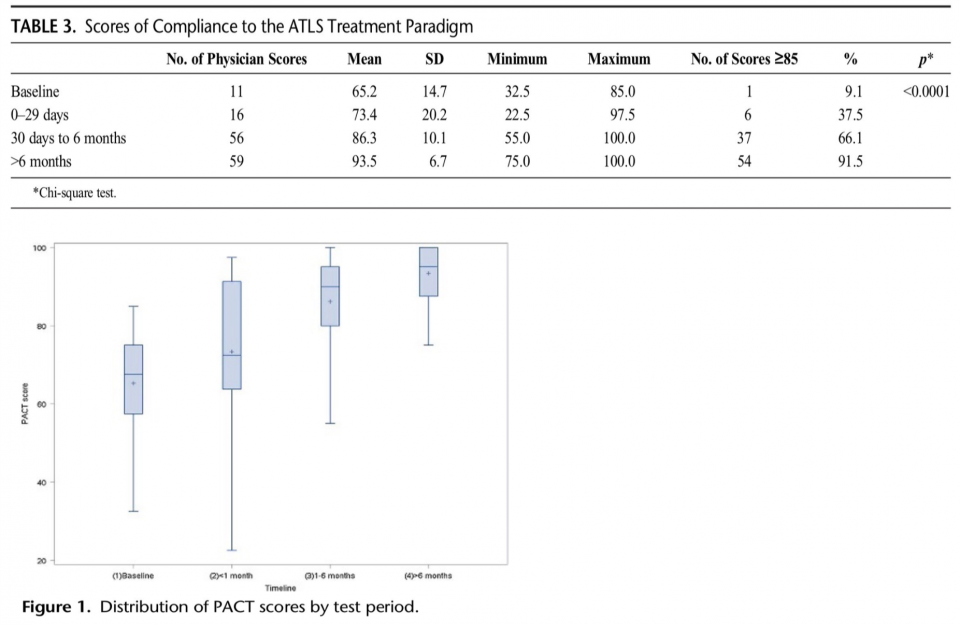
They were able to demonstrate progressively increasing compliance with ATLS protocols and increased numbers of passing grades. They also saw more consistency with decreased variability between providers. Though these are surrogate outcomes, it is difficult to argue that maintaining a more consistent standard of care for trauma patients is a bad thing.
This form of evaluation, however, is quite controversial and there is a lot of anxiety and hesitation towards it. There are many important hurdles that must be addressed prior to implementation of this kind of tool.
Some non-exhaustive challenges highlighted by Lowe et al. include:
-
- Time consuming and tedious process
- Outputs and video analysis are highly sensitive to both patients and providers
- We need standardized and accepted evaluation tools which do not currently exist
- Ethical and legal issues
While video review appears to have significant educational and quality improvement benefits, it likely will require acceptance within the culture of your department and overcoming significant ethical and legal hurdles. It is best to meet with department heads and decision makers to determine if it is right for your ED.
Conclusion
- Human factors play an important role in the logistics of resuscitation
- There are aspects of logistics that we can improve upon in the three phases of resuscitation
- These include:
- Optimization and preparation of environment and equipment
- Pre-arrival briefing
- Use of high and low acuity cognitive aids
- Task specific sub-teams
- Regular, standardized debriefing
- Retrospective, after-action review and report
- Things I was unable to get to but would be worth looking into if interested:
- Structured EMS handover
- RN led codes
- Technological cognitive aids
References
- Chrimes, N. (2016). The Vortex: a universal ‘high-acuity implementation tool’ for emergency airway management. British Journal of Anaesthesia, 117, pp.i20-i27.
- Davis, T. (2018). Lessons from the Bromiley Case • LITFL • Life in the Fast Lane Medical Blog. [online] LITFL • Life in the Fast Lane Medical Blog. Available at: https://lifeinthefastlane.com/lessons-bromiley-case/ [Accessed 4 Jan. 2018].
- com. (2018). Workflow of an ETC scenario – European Trauma Course – The Team Approach to Trauma. [online] Available at: http://europeantraumacourse.com/workflow-of-an-etc-scenario/ [Accessed 4 Jan. 2018].
- Hicks, C. and Petrosoniak, A. (2018). The Human Factor. Emergency Medicine Clinics of North America, 36(1), pp.1-17.
- Inzana, C., Driskell, J., Salas, E. and Johnston, J. (1996). Effects of preparatory information on enhancing performance under stress. Journal of Applied Psychology, 81(4), pp.429-435.
- Kessler, D., Cheng, A. and Mullan, P. (2015). Debriefing in the Emergency Department After Clinical Events: A Practical Guide. Annals of Emergency Medicine, 65(6), pp.690-698.
- Lashoher, A., et al. (2016). Implementation of the World Health Organization Trauma Care Checklist Program in 11 Centers Across Multiple Economic Strata: Effect on Care Process Measures. World Journal of Surgery, 41(4), pp.954-962.
- Lowe, D., Dewar, A., Lloyd, A., Edgar, S. and Clegg, G. (2016). Optimising clinical performance during resuscitation using video evaluation. Postgraduate Medical Journal, 93(1102), pp.449-453.
- Nolan, B., Zakirova, R., Bridge, J. and Nathens, A. (2014). Barriers to implementing the World Health Organization’s Trauma Care Checklist. Journal of Trauma and Acute Care Surgery, 77(5), pp.679-683.
- Patterson, M., Geis, G., Falcone, R., LeMaster, T. and Wears, R. (2012). In situ simulation: detection of safety threats and teamwork training in a high risk emergency department. BMJ Quality & Safety, 22(6), pp.468-477.
- Sandhu, N., Eppich, W., Mikrogianakis, A., Grant, V., Robinson, T. and Cheng, A. (2014). Postresuscitation debriefing in the pediatric emergency department: a national needs assessment. CJEM, 16(05), pp.383-392.
- http://www.who.int/emergencycare/publications/trauma-care-checklist.pdf [Accessed 4 Jan. 2018].
- Wurster, L., Thakkar, R., Haley, K., Wheeler, K., Larson, J., Stoner, M., Gewirtz, Y., Holman, T., Buckingham, D. and Groner, J. (2017). Standardizing the initial resuscitation of the trauma patient with the Primary Assessment Completion Tool using video review. Journal of Trauma and Acute Care Surgery, 82(6), pp.1002-1006.
- Mastoras, G. (2016). Stress-testing the Resus Room: Latent threats to patient safety identified during interprofessional in-situ simultiaon in the Emergency Department.


Trackbacks/Pingbacks