
For other ultrasound cases see our POCUS archives
Case Vignette
63-year-old male presents with a two-day history of groin pain and swelling. He has a history of hypertension and smoking. He takes an anti-hypertensive medication and an atypical antipsychotic for sleeping. The patient denies abdominal pain, nausea/vomiting, back pain, fevers, trauma.
At triage he is alert, oriented and in no acute distress. He appears comfortable and is breathing normally. His vitals are as follows:
- Temperature 36.8°C
- Heart Rate 99/min
- Blood Pressure 91/57
- O2 Sat 99% RA
His abdominal, cardiac and respiratory exams are normal.
With only the information provided think of you differential and how POCUS can help narrow your probability of certain diagnoses.
Differential
- Testicular torsion
- Epididymitis/Epididymo-orchitis
- Fournier’s gangrene
- Pelvic abscess
- Incarcerated hernia
- AAA
- Renal colic
- Cellulitis
- Torsion of the appendix testis
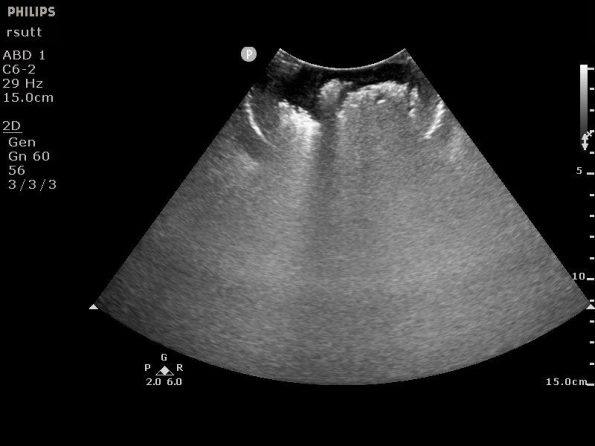
With your differential in mind you initially complete an aortic scan and renal scan. As with any POCUS scan, we have a clinical question that we are attempting to answer. In this situation we have a gentleman with groin pain and hypotension, our clinical question is as follows, “Is there a AAA – yes or no” and, “Is there hydronephrosis – yes or no.”
While looking through the scans attempt to generate an opinion on our question.
These are normal scans. Based on the literature, we can confidently rule out AAA as the source of our patient’s hypotension [1]. Additionally, we can say that, at the current moment, this patient does not have hydronephrosis.
Moving on in the case, you decide the next step is to examine the area in question. On examination of the external genitalia, you find an uncircumcised penis with an edematous foreskin, extensive erythema of the scrotum extending to the base of the scrotum and superiorly to the base of the penile shaft, and inferior-posteriorly to the anus with an area of erythema overlying the left initial tuberosity. There is mild tenderness throughout. There appears to be fluid within the scrotum itself.
This narrows your differential quite substantially. You are now quite concerned about an infectious process involving the perineum and scrotum, quite possibly Fournier’s gangrene. Fluids are running, antibiotics are in and while considering your next step, you elect to perform a bedside testicular scan to assess the testes and scrotum.
Again, try to generate an interpretation as you are looking at the scans.

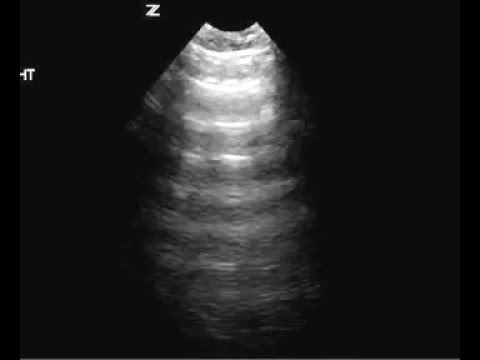
This is a very atypical appearance of the scrotum and testes. For reference, here is the ultrasonographic appearance of the testicles normally.
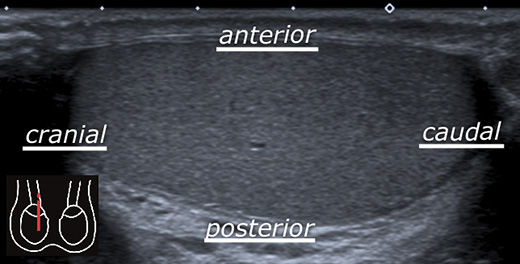
From http://www.startradiology.com/internships/urology/scrotum/scrotal-ultrasound/
These images demonstrate subcutaneous thickening of the scrotal skin, fluid within the scrotum and a significant amount of air artifact including dirty shadowing, ring-down artifact . These findings are consistent with a diagnosis of necrotizing fasciitis or Fournier’s gangrene.
Urology is paged to come assess the patient as you continue resuscitation. The patient stabilizes prior to OR and is taken for CT scan for operative planning.
It demonstrates:
- Extensive gas tracking throughout the scrotal wall, the perineum and along the spermatic cords. A small amount of gas is also seen in the left ischial rectal fossa. No perianal abscess is shown. No significant fluid collection or drainable abscess.
The patient is taken to the OR that night for debridement and wash-out. He does well and is discharged a few weeks later.
POCUS Pearls: Diagnosis of Necrotizing Fasciitis using Ultrasound
Necrotizing fasciitis is a time sensitive diagnosis with significant morbidity and some mortality associated with it. History and physical exam alone can be unreliable especially in the early stage of the disease process [3]. XR may be helpful, but has little diagnostic capability, and CT, while accurate, requires the patient leave the department for a length of time when they may be too unwell to do so [2]. POCUS is a readily available alternative if you know what to look for.
Castleberg et al, describe a three-step approach to look for necrotizing fasciitis using POCUS named the STAFF approach [2,3]. The mnemonic stands for subcutaneous thickening, presence of air and fascial fluid. In the context of Fournier’s gangrene, thickened and edematous scrotal wall, peri-testicular fluid and soft tissue air would suggest the diagnosis readily.
Like a lot of POCUS, it is not likely that there will be a large, multi-centre randomized controlled evidence to support some of its use. Yen and colleagues, in 2008, looked at 62 patients with suspected necrotizing fasciitis of the limbs and prospectively followed them comparing POCUS to pathological findings. Unfortunately, patients with genital involvement were excluded. Additionally, the STAFF protocol did not include an assessment looking for air. Interpreting the results with a grain of salt given study design, methodology and sample size they found that POCUS had a sensitivity of 88.2% (63.6 – 98.5%) and specificity of 93.3% (81.7 – 98.6%) [4].
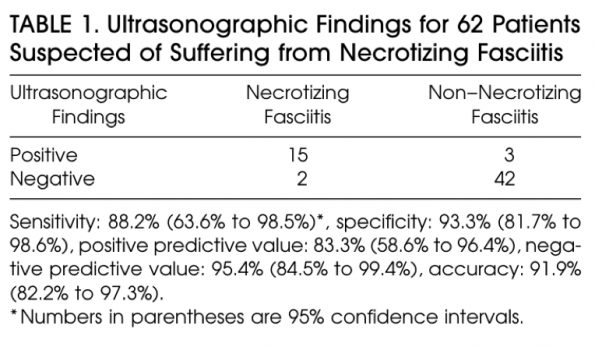
Yen, Z. (2002). Ultrasonographic Screening of Clinically-suspected Necrotizing Fasciitis. Academic Emergency Medicine, 9(12), pp.1448-1451.
Air Artifact and its Use in POCUS
The detection of air in areas of the body where it should not be can be extremely helpful clinically. Air can be found in pathological anatomic locations using POCUS however its presence may be subtle. Therefore, an understanding of the artifacts it creates is essential for a critical care POCUS provider.
If you’ve done any scanning of the lungs or abdomen, you know what air looks like on ultrasound. It will display ring down artifact, ‘dirty shadowing’ and reverberation artifact (A line pattern). Dirty shadowing (seen below) is due to a phenomenon known as impedance mismatch [2]. When the sound beams encounter an interface of two substances that impede the beam progression at different rates (air and solid), they are reflected therefore limiting the penetration of the beam and the image generated [2]. This can be ‘clean’ or ‘dirty’. Clean shadowing occurs with structures such as bone, which absorb sound, while dirty shadowing typically occurs at air-tissue interfaces which reflect sound [2]. The presence of dirty shadowing in the abdomen can be normal (ie. when looking for the appendix, this is the typical appearance of the cecum) however when present in other anatomical locations can indicate pathology.
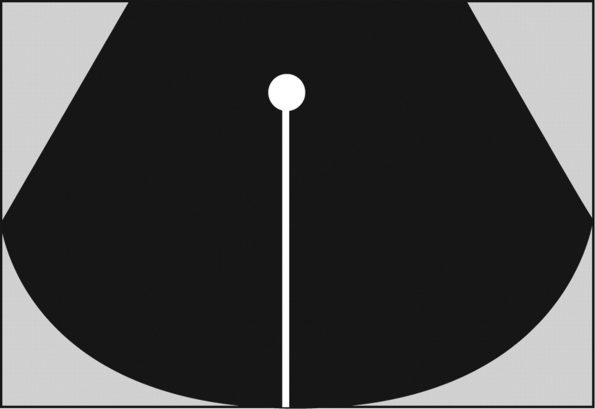
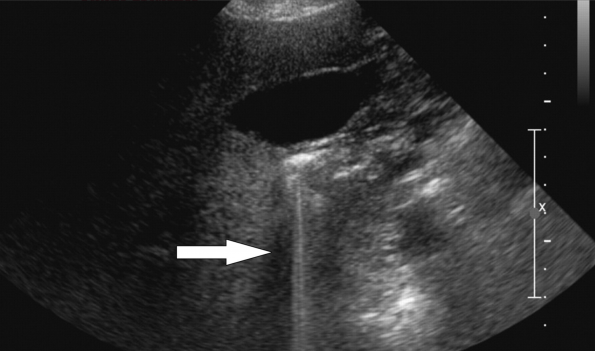
Ring down artifact can appear similar to comet-tail artifact in the lung and occurs when gas bubbles are trapped within tissue with fluid [5]. The fluid trapped within gas bubbles will resonate and create a continuous signal back to the probe. This appears as a bright reflector with an echogenic line extending downwards off the screen [6]. Again, this can be normal when seen in the duodenum (as in the image below) but pathological when seen in the gallbladder wall.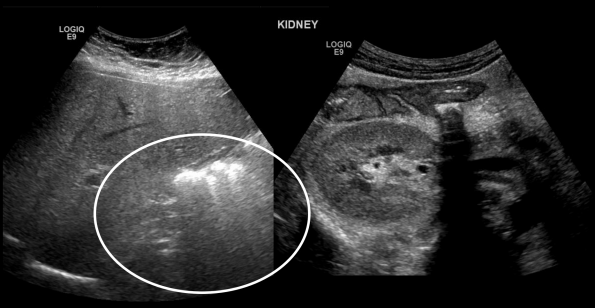
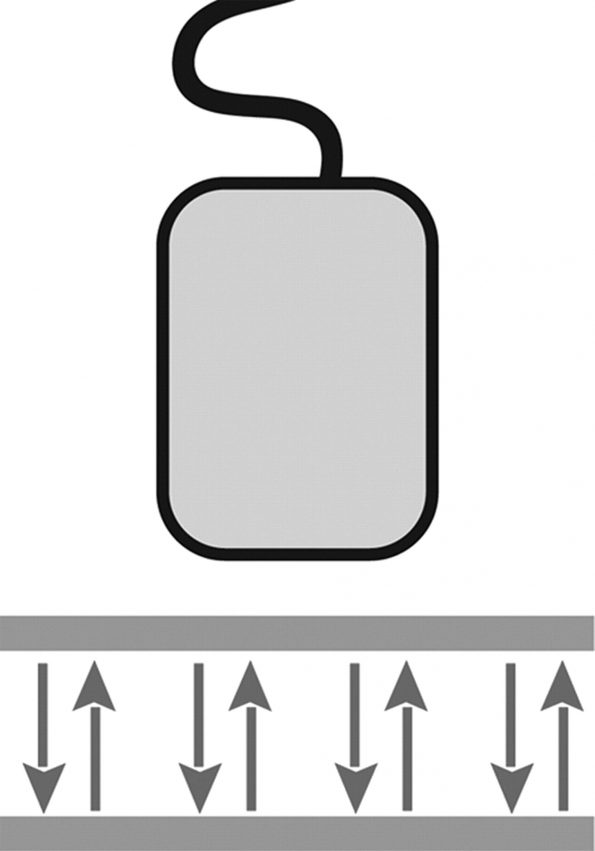
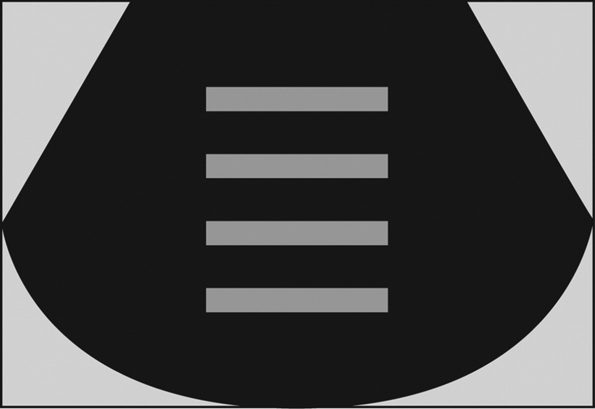
Finally, air can demonstrate reverberation artifact which is seen in the lungs as an ‘A-line pattern’ and comet-tail artifacts. The ultrasound transducer assumes that any echoes it is receiving back are from a single reflection and uses the time it takes for the sound beams to return to generate a distance/depth for this reflection [6]. When a highly reflective medium is encounters (such as air) the echoes can be repeatedly reflected back and forth between the medium and the transducer. The transducer assumes these are all new reflections and because each one takes exactly double the amount of time to return, it will generate a similar image exactly twice as far away from the probe as the previous one [6]. Comet-tail artifacts are a form of reverberation artifact [6]. Unlike ring-down artifact, this is not specific to air however it can suggest the presence of air.
Conclusions
POCUS can be a helpful adjunct in the diagnostic algorithm for necrotizing fasciitis and can help rule in the diagnosis when patient presentation is equivocal. However, it should not be used to rule out necrotizing fasciitis as there is no current evidence demonstrating sufficient test characteristics for this indication. This remains an area of gestalt and composing the entire clinical picture with a high pretest probability POCUS should not alter your decision for specialist consultation and appropriate resuscitation and antibiotic therapy.
References:
- Rubano, E., Mehta, N., Caputo, W., Paladino, L. and Sinert, R. (2013). Systematic Review: Emergency Department Bedside Ultrasonography for Diagnosing Suspected Abdominal Aortic Aneurysm. Academic Emergency Medicine, 20(2), pp.128-138.
- Buttar, S., Cooper, D., Olivieri, P., Barca, M., Drake, A., Ku, M., Rose, G., Siadecki, S. and Saul, T. (2017). Air and its Sonographic Appearance: Understanding the Artifacts. The Journal of Emergency Medicine, 53(2), pp.241-247.
- Castleberg, E., Jenson, N. and Dinh, V. (2014). Diagnosis of Necrotizing Faciitis with Bedside Ultrasound: the STAFF Exam. Western Journal of Emergency Medicine, 15(1), pp.111-113.
- Yen, Z. (2002). Ultrasonographic Screening of Clinically-suspected Necrotizing Fasciitis. Academic Emergency Medicine, 9(12), pp.1448-1451.
- Bost, N. and Morgan, M. (2018). Ring down artifact. [online] Radiopaedia. Available at: https://radiopaedia.org/articles/ring-down-artifact-1https://radiopaedia.org/articles/ring-down-artifact-1 [Accessed 29 Nov. 2018].
- Feldman, M., Katyal, S. and Blackwood, M. (2009). US Artifacts. RadioGraphics, 29(4), pp.1179-1189.
- Paushter, D. (2015). Primer and Clinical Significance of Artifacts in Ultrasound. [online] Radiology.uchicago.edu. Available at: https://radiology.uchicago.edu/sites/radiology.uchicago.edu/files/uploads/Lectures/1505012_UCCME%20Radiology_Review.pdf [Accessed 29 Nov. 2018].
