Mechanical CPR is a technology whereby a machine performs chest compressions in place of a human provider. These devices are becoming increasingly prevalent in the prehospital and in-hospital arenas, and it is inevitable that healthcare providers will interact with them in some capacity. Given the variable evidence in the literature, the indications for when to apply these devices is not clear. After reading this post, we hope you will:
- Understand the background of CPR, current guideline recommendations, and the physiologic advantages and disadvantages of manual and mechanical CPR
- Recognize the features and limitations of the two most commonly used mechanical devices, the LUCAS and Autopulse
- Appraise the current evidence as it pertains to prehospital, in-hospital, and emergency department locations
- Appreciate the data regarding safety in mechanical CPR
- Learn special circumstances in which mechanical CPR can be applied, including air ambulance transport and ECMO
Background

- 1891 – First documented case of closed cardiac massage was by Dr. Friedrich Maass. He was a surgical resident in Germany at the time and performed the procedure on two pediatric patients. He noticed that it resulted in a palpable carotid pulse.
- 1901- First open cardiac massage was performed, and this becomes the standard of care until the 1960s. During this period resuscitation was usually performed in the operating room, and therefore surgical techniques dominated the field.
- 1957 – Closed cardiac massage is re-introduced by Dr. James Jude and electrical engineers William Kouwenhoven and Guy Knickerbocker. They were perfecting closed chest heart defibrillation and noticed a slight rise in blood pressure when the electrodes were placed upon the chest wall.
- 1961- The first mechanical CPR devices are created
- 1980s – Vest CPR devices enter the market – these were the predecessors of the modern Autopulse
- 2000s – LUCAS device enters the market
CPR – Why do we do it?
- CPR is used to sustain basic perfusion to critical organs including the heart and brain during cardiac arrest
- Analogy:
- When a catastrophe occurs during flight, one pilot’s only task is to fly the plane and “keep it in the air”, while the other pilot tries to figure out the problem and fix it. CPR is similar – it is merely a holding pattern until you can figure out why the patient arrested and fix it.
- Crisis resource management (CRM) perspectives to consider:
- Manual CPR likely increases the cognitive load of the code leader who must split their attention between diagnosing the cause of arrest and ensuring high-quality CPR is being performed at all times.
- This line-up of people waiting to do CPR can be noisy, visually distracting, and obstruct vascular access.

CPR Physiology – Man or Machine?
When we examine basic physiologic parameters, what do you think will perform better, mechanical or manual CPR? How about a machine that can be dialed in to hit guideline parameters almost perfectly, never gets tired, has a suction cup to ensure full recoil, a built-in backboard, and lets you shock anytime without risk of injury? Let’s focus just on physiology for a second; we’ll take a look at what the data shows.
Manual CPR
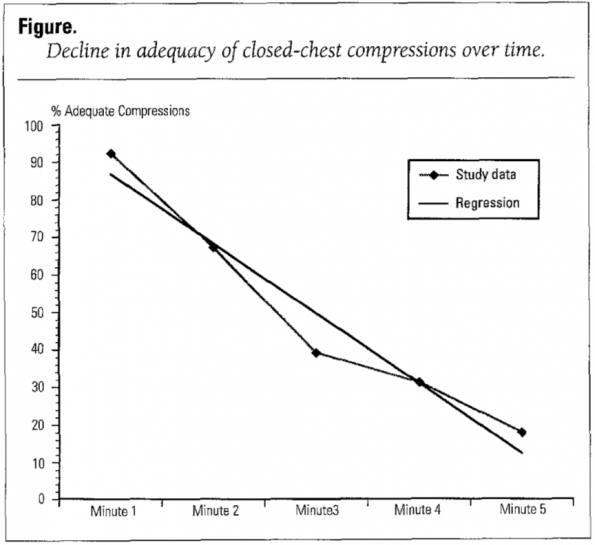
- Hightower 1995 [1]
- Human CPR performance steadily declines over time. They found 92.9% of compressions performed during minute 1 to be correct. The percentages for minutes 2 through 5 were as follows: 67.1%, 39.2%, 31.2%, and 18.0%.
- Most concerning, however, was that candidates had little self-awareness of this drop in performance when asked to self-evaluate their skill over time.
- Abella 2005 [2]
- Humans performed CPR at a rate of less than 90 compressions per minute for a third of the duration of the cardiac arrest, with compressions being too shallow about 40% of the time.
Mechanical CPR (compared to manual CPR)
- Increased mean diastolic BP [3]
- Increased MAP [3]
- Increased ETCO2 [4]
- Increased cortical cerebral blood flow [5]
Mechanical CPR Devices

LUCAS
- “Lund University Cardiac Arrest System”
- Developed in Sweden in the early 2000s
- Manufactured by Physio-Control, a company owned by Stryker
- Battery powered
- Uses a piston device that adjusts to patient’s circumference to deliver compressions
- The piston device has a suction cup to ensure active decompression and full recoil
- Compresses at a rate of 100 compressions/min, with a depth of 4-5 cm
- While they state there is no maximum weight, the person must obviously be able to fit within the circumference of the device

Autopulse
- Manufactured by Zoll after it was acquired in 2003
- Uses a load-distributing band design that uses an electric motor to pull the two ends of the band in a rhythmic cyclic fashion
- Because of its unique circumferential design, it compresses at a rate of 80 beats per minute and a depth of 20% of the AP height
- The backboard can support up to 300 lb and can fit a circumference of 130 cm
Guidelines
ILCOR 2015
- Suggest against the routine use of automated mechanical chest compression devices to replace manual chest compressions (weak recommendation, moderate-quality evidence)
- Suggest that automated mechanical chest compression devices are a reasonable alternative to high-quality manual chest compressions in situations where sustained high-quality manual chest compressions are impractical or compromise provider safety (weak recommendation, low-quality evidence)
AHA 2015
- The evidence does not demonstrate a benefit with the use of mechanical piston devices for chest compressions versus manual chest compressions in patients with cardiac arrest.
- The use of mechanical piston devices may be considered in specific settings where the delivery of high-quality manual compressions may be challenging or dangerous for the provider (e.g., limited rescuers available, prolonged CPR, during hypothermic cardiac arrest, in a moving ambulance, in the angiography suite, during preparation for extracorporeal CPR), provided that rescuers strictly limit interruptions in CPR during deployment and removal of the devices. (Class IIb)
ERC 2015
- The routine use of mechanical chest compression devices is not recommended, but they are a reasonable alternative in situations where sustained high-quality manual chest compressions are impractical or compromise provider safety.
Prehospital Literature
Observational trials
Casner 2005 [6]
- One of the first prehospital observational studies was a case-control study looking at ROSC outcomes after the San Francisco Fire Department started using an Autopulse device during their cardiac arrests
- Evaluated 69 cases where an Autopulse was used
- Results:
- Higher rates of ROSC with mechanical CPR (39%) versus manual CPR (29%)
- When they looked only at shockable rhythms, they found no difference in ROSC
- Limitations:
- Observational nature and selection bias
Ong 2006 [7]
- A before/after observational study of 783 patients with the Richmond, Virginia EMS group after they changed from manual CPR to the Autopulse device
- Results:
- Increased ROSC (34.5% vs. 20.2%) and improved survival to discharge (9.7% vs. 2.9%) with mechanical CPR vs. manual CPR
- Limitations:
- Faster EMS response times and more EMS witnessed arrests in the mechanical CPR group
- One hospital instituted a hypothermia protocol in the “after” group
Randomized Controlled Trials
Hallstrom 2006 [8]
- Industry-sponsored multicenter RCT of 1071 patients comparing mechanical (Autopulse) to manual CPR in US/Canadian setting
- Results:
- 4 hour survival (29.5% manual vs 28.5% mechanical)
- Time from 911 call to shock (9.7 min manual vs. 11.8 min mechanical)
- Time to shock 2.1 minutes longer in the mechanical group, likely from time to fit and apply the device
- Survival with good neuro outcome (7.5% manual vs 3.1% mechanical, P = 0.006)
- Their study was stopped early at the first planned interim analysis due to worse neuro outcomes in the mechanical CPR arm. The authors came up with a few reasons for harm associated with mechanical CPR:
- Hawthorne effect
- The “superior blood flow” from the machine could have resulted in increased levels of cerebral epinephrine and increased reperfusion injury
- Their study was stopped early at the first planned interim analysis due to worse neuro outcomes in the mechanical CPR arm. The authors came up with a few reasons for harm associated with mechanical CPR:
CIRC 2014 [9]
- Industry-sponsored multicenter RCT of 4231 patients comparing mechanical (Autopulse) to manual CPR in US/European setting
- Powered to detect equivalence, superiority, or inferiority in their primary outcome of survival to hospital discharge
- Inclusion/Exclusion criteria to note:
- The arrest must have been from presumed cardiac origin
- Excluded patients presumed too large for the device and EMS units that arrived over 16 minutes after the initial call
- Results
- Survival to hospital discharge (11.0% manual vs. 9.4% mechanical)
- ROSC (32.3% manual vs 28.6% mechanical)
- Good neuro outcome (5.3% manual vs. 4.1% mechanical)
- CPR quality data
- CIRC was one of the few trials to provide robust CPR quality data. While they did not report any information about compression depth, they were able to report compression fraction in almost of all the cases studied.
- CPR fraction:
- At 5 min: manual 79% vs. 74.7% mech
- At 20 min: manual 80.2% vs. 80.4% mech
- Notice that you are losing out on CPR fraction in the first 5 minutes. This is likely due to the time required to apply the device. This fraction then closes and by 20 minutes it is equivalent to manual CPR.
- Limitations:
- Very high compression fraction in the manual group of almost 80%, much higher than the 50-60% usually reported in out of hospital trials [8]. This focus on “ensuring perfect CPR” is one of the major criticisms of this trial as it may have overestimated the quality of manual CPR compared to what we see in real-life settings and may limit the generalizability of these results.
LINC 2014 [10]
- Industry-sponsored multicenter RCT of 2589 patients comparing mechanical (LUCAS) to manual CPR in Europe
- Results:
- 4 hour survival (23.7% manual vs. 23.6% mechanical)
- Survival to discharge (9.2% manual vs. 9.0% mechanical)
- Good neuro outcome (7.3% manual vs. 8.1% mechanical)
- Limitations:
- It should be noted that this trial used a significantly modified treatment algorithm in the mechanical CPR arm. In this arm, manual CPR was performed until the device could be applied as per usual. But after this, they used a 3-minute CPR cycle instead of the usual 2 minutes. Additionally, everybody getting mechanical CPR was shocked at the 90 second mark without checking the rhythm.
- This modified treatment algorithm limits generalizability
PARAMEDIC 2015 [11]
- Academia sponsored pragmatic multicenter RCT of 4470 patients comparing mechanical (LUCAS) to manual CPR in the UK
- Results:
- 30 day survival (7% manual vs. 6% mechanical)
- 30 day survival with an initial shockable rhythm (24% manual vs. 18% mechanical)
- Good neuro outcome (6% manual vs. 5% mechanical)
- Limitations:
- Only 60% of patients randomized to the mechanical CPR arm actually received it
Systematic Review
Gates 2015 [12]
- This systematic review pooled the data from all 5 RCTs and found no difference in favorable neuro outcome or 30 day survival for mechanical CPR compared to manual CPR
Summary
Looking at all of the data, my recommendations for OOHCA are the following:
- I would avoid applying mechanical CPR early in resuscitation and instead focus on minimizing time to shock
- Certain cases exist where mechanical CPR may be of benefit, including:
- Refractory VF/VT arrest
- Hypothermia
- Situations where CPR cannot be performed effectively
- In the back of a moving ambulance, helicopter ,or during prolonged extrication
- In all situations, training should be performed to ensure pit crew-like performance in minimizing CPR interruptions when applying the device
In-Hospital Literature
As we can all attest to, in-hospital cardiac arrests can be quite different in nature compared to the prehospital scene. There are often more resources available, and in many cases, providers have quicker response times. Given these differences, it may be possible to train providers to provide rapid application of mechanical devices as well as use it as a bridge to further therapies including ECMO.
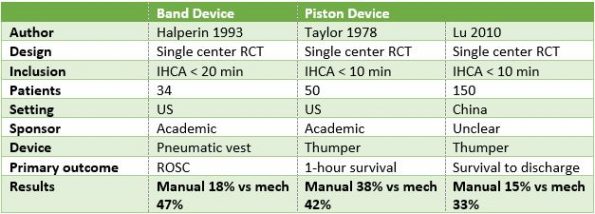
- The evidence is very scarce in this arena, with only three RCTs in total, and only one in the last 20 years. [13-15] The trials are summarized in this table:
Couper 2016 [16]
- This meta-analysis compiled the results of the 3 RCTs shown above as well as 3 additional observational studies
- Results:
- Improved odds of 30-day survival with mechanical CPR (OR 2.3)
- These results are interesting in that they differ significantly from the prehospital environment. While the overall quality of evidence is weak, this may reflect actual differences, i.e. mechanical devices may be more effective than manual chest compressions in the hospital setting.
- Currently, a feasibility study is underway called COMPRESS-RCT that is looking to see if a larger in-hospital RCT will be possible in the future.
Summary for IHCA
- Low-quality evidence to suggest mechanical CPR may improve outcomes
- We suggest use in the following scenarios:
- Limited personnel to perform CPR
- Refractory VF/VT
- Bridge to ECMO/PCI
- Hypothermia
Emergency Department Literature
The emergency department is heterogeneous environment where we treat our own de novo cardiac arrests, but also handle those that occur out of hospital and are brought to us by our EMS colleagues. Emergency physicians arguably have the most experience with cardiac arrests and see the highest patient volumes in terms of the arrested patient. EDs also vary tremendously in the amount of resources that they have. Imagine you are working in a rural ED overnight with only 2 nurses, and a hypothermic arrest comes into your department. A mechanical CPR device may free up significant resources.
Evidence
- Unfortunately, the evidence is scarce when looking specifically at the emergency department population. There are no RCTs and only a few observational trials.
Hayashida 2017 [17]
- A recent Japanese multicenter observational trial that included over 6500 patients. It found reduced odds of ROSC and survival to discharge with mechanical CPR. Unfortunately, the study was severely biased as the decision to apply the device was made on a case-per-case basis by the emergency physician, and the actual device used was not reported in two-thirds of cases.

Ong 2012 [18]
- This was a before/after observational study in two Singapore emergency rooms involving about 1000 patients. They found contrasting results, with improved hospital survival and neuro outcome in patients treated with mechanical CPR in the emergency department.
- Interestingly, the team that deployed the device in this study had received focussed pit crew training to minimize pauses associated with its use. Significant emphasis was placed on teamwork, minimizing delay in applying the device, and minimizing interruptions to CPR.
- This study may be a signal that in highly trained teams, for example as found in an emergency department resuscitation bay, these devices may show a benefit.
Safety
Mechanical CPR devices at first glance look rather menacing. Everyone has heard their share of anecdotes reporting serious injuries with these devices. But are they as dangerous as they may appear? Let’s take a look at the evidence.
Koster 2017 [20]
- A randomized non-inferiority trial specifically made to answer the question of safety of both LUCAS and Autopulse devices. It featured 340 patients from in-hospital and out-of-hospital cardiac arrests.
- Primary outcome: safety via serious visceral damage assessed by autopsy, post-mortem CT, or clinical outcome
- Results:
- LUCAS device was non-inferior to manual CPR (7.4% LUCAS vs. 6.4% manual)
- For Autopulse, an increase in serious damage could not be excluded (11.6% Autopulse vs. 6.4% manual)
- No difference in the secondary outcome of combined rib and sternum fractures (45.6% Autopulse, 39.8% LUCAS, 41.3% manual)
Summary
- The LUCAS device is non-inferior when compared to manual CPR with regards to causing serious injuries
- For the Autopulse device, more damage cannot be excluded
- This difference may be due to the inherent difference in the mechanism of the devices
Special Circumstances

HEMS
Air ambulances represent a special population that would likely greatly benefit from having mechanical CPR device on board. You can appreciate that performing high-quality CPR in the small enclosed space of a moving helicopter would be extremely difficult, if not impossible.
- Interestingly, the ERC Guidelines addressed this in 2015
- Mechanical chest compression devices enable delivery of high-quality chest compressions in the confined space of an air ambulance, and their use should be considered. If a cardiac arrest during flight is thought to be a possibility, consider fitting the patient within a mechanical chest compression device during packaging before a flight.
- There is currently a paucity of evidence to support or refute the use of mechanical CPR devices in air ambulance transport.
Until there are better trials, I recommend bringing this device on all flights where there is a high possibility of cardiac arrest.
ECMO
For situations arising where a patient is in refractory cardiac arrest and is being considered for ECMO, mechanical CPR may serve as an excellent bridge. It allows for consistent high-quality CPR and frees up hands to allow for cannulation. Evidence wise, there are no randomized controlled trials here, but one trial we should examine is the CHEER trial, performed in 2015 [21]
- This was a small prospective trial that included 26 patients with refractory OOH/IHCA.
- Inclusion criteria:
- Patients 18-65 with suspected cardiac etiology
- Compressions started within 10 minutes by EMS or bystanders
- Initial rhythm VF
- Mechanical CPR device readily available
- Protocol:
- Apply the Autopulse device
- Induce hypothermia
- Cannulate the patient and put them on ECMO
- Perform definitive therapy with PCI
- Results:
- Overall 54% survival to discharge rate with CPC = 1
- In this study the median time from collapse to initiation of ECMO was just under 1 hour, suggesting that mechanical CPR may be a good tool for very select patients in a refractory arrest of presumed cardiac etiology to bridge to ECMO
Summary
We will leave you with our final recommendations given all of the current evidence. Situations when you should consider mechanical CPR:
- Limited resources available (such as in a rural emergency department)
- Hypothermic arrest
- Refractory VF/VT
- Ground or air ambulances
- Bridge to/during PCI
- Preparation for ECMO
Finally:
- Avoid mechanical CPR early in cardiac arrest
- Almost all of the trials have data pointing to worse outcomes in cases where these devices are applied to patients with initial shockable rhythms
- Lastly, don’t forget the basic foundations of cardiac resuscitation! Emphasis should always remain on rapid defibrillation, minimizing pauses, and performing high-quality CPR.
References
- Hightower D, Thomas SH, Stone CK, Dunn K, March JA. Decay in quality of closed-chest compressions over time. Annals of Emergency Medicine 1995;26(3):300–3.
- Abella BS, Alvarado JP, Myklebust H, et al. Quality of cardiopulmonary resuscitation during in-hospital cardiac arrest. JAMA 2005;293(3):305–10.
- Duchateau F-X, Gueye P, Curac S, et al. Effect of the AutoPulse™ automated band chest compression device on hemodynamics in out-of-hospital cardiac arrest resuscitation. Intensive Care Med 2010;36(7):1256–60.
- Axelsson C, Karlsson T, Axelsson ÅB, Herlitz J. Mechanical active compression–decompression cardiopulmonary resuscitation (ACD-CPR) versus manual CPR according to pressure of end tidal carbon dioxide (PETCO2) during CPR in out-of-hospital cardiac arrest (OHCA). Resuscitation 2009;80(10):1099–103.
- Rubertsson S, Karlsten R. Increased cortical cerebral blood flow with LUCAS; a new device for mechanical chest compressions compared to standard external compressions during experimental cardiopulmonary resuscitation. Resuscitation 2005;65(3):357–63.
- Casner M, Andersen D, Isaacs SM. The impact of a new CPR assist device on rate of return of spontaneous circulation in out-of-hospital cardiac arrest. Prehospital Emergency Care 2005;9(1):61–7.
- Ong MEH, Ornato JP, Edwards DP, et al. Use of an automated, load-distributing band chest compression device for out-of-hospital cardiac arrest resuscitation. JAMA 2006;295(22):2629–37.
- Hallstrom A, Rea TD, Sayre MR, et al. Manual chest compression vs use of an automated chest compression device during resuscitation following out-of-hospital cardiac arrest: a randomized trial. JAMA 2006;295(22):2620–8.
- Wik L, Olsen J-A, Persse D, et al. Manual vs. integrated automatic load-distributing band CPR with equal survival after out of hospital cardiac arrest. The randomized CIRC trial. Resuscitation 2014;85(6):741–8.
- Rubertsson S, Lindgren E, Smekal D, et al. Mechanical Chest Compressions and Simultaneous Defibrillation vs Conventional Cardiopulmonary Resuscitation in Out-of-Hospital Cardiac Arrest. JAMA 2014;311(1):53–9.
- Perkins G, Lall R, Quinn T, et al. Mechanical versus manual chest compression for out-of-hospital cardiac arrest (PARAMEDIC): a pragmatic, cluster randomised controlled trial. The Lancet 2015;385(9972):947–55.
- Gates S, Quinn T, Deakin CD, Blair L, Couper K, Perkins GD. Mechanical chest compression for out of hospital cardiac arrest: Systematic review and meta-analysis. Resuscitation 2015;94:91–7.
- Taylor GJ, Rubin R, Tucker M, Greene HL, Rudikoff MT, Weisfeldt ML. External cardiac compression. A randomized comparison of mechanical and manual techniques. JAMA 1978;240(7):644–6.
- Halperin HR, Tsitlik JE, Gelfand M, et al. A preliminary study of cardiopulmonary resuscitation by circumferential compression of the chest with use of a pneumatic vest. N Engl J Med 1993;329(11):762–8.
- Lu X, Kang X, Gong D. The clinical efficacy of Thumper modal 1007 cardiopulmonary resuscitation: a prospective randomised control trial. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2010;22(8):496–7.
- Couper K, Yeung J, Nicholson T, Quinn T, Lall R, Perkins GD. Mechanical chest compression devices at in-hospital cardiac arrest: A systematic review and meta-analysis. Resuscitation 2016;103:24–31.
- Hayashida K, Tagami T, Fukuda T, et al. Mechanical Cardiopulmonary Resuscitation and Hospital Survival Among Adult Patients With Nontraumatic Out‐of‐Hospital Cardiac Arrest Attending the Emergency Department: A Prospective, Multicenter, Observational Study in Japan (SOS‐KANTO [Survey of Survivors after Out‐of‐Hospital Cardiac Arrest in Kanto Area] 2012 Study). J Am Heart Assoc 2017;6(11):1–12.
- Ong MEH, Fook-Chong S, Annathurai A, et al. Improved neurologically intact survival with the use of an automated, load-distributing band chest compression device for cardiac arrest presenting to the emergency department. Critical Care 2012;16(4):R144.
- Baumeister R, Held U, Thali MJ, Flach PM, Ross S. Forensic imaging findings by post-mortem computed tomography after manual versus mechanical chest compression. Journal of Forensic Radiology and Imaging 2015;3(3):167–73.
- Koster RW, Beenen LF, van der Boom EB, et al. Safety of mechanical chest compression devices AutoPulse and LUCAS in cardiac arrest: a randomized clinical trial for non-inferiority. Eur Heart J 2017;38(40):3006–13.
- Stub D, Bernard S, Pellegrino V, Smith K, Walker T, Sheldrake J, et al. Refractory cardiac arrest treated with mechanical CPR, hypothermia, ECMO and early reperfusion (the CHEER trial). Resuscitation 2015;86:88–94.